Pancreatic ductal adenocarcinoma contributes significantly to global cancer-related deaths, featuring only a 10% survival rate over five years. The quest for novel tumor markers is critical to facilitate early diagnosis and tailor treatment strategies for this disease, which is key to improving patient outcomes. In pancreatic ductal adenocarcinoma, these markers have been demonstrated to play a crucial role in early identification, continuous monitoring, and prediction of its prognosis and have led to better patient outcomes. Nowadays, biopsy specimens serve to ascertain diagnosis and determine tumor type. However, liquid biopsies present distinct advantages over conventional biopsy techniques. They offer a noninvasive, easily administered procedure, delivering insights into the tumor’s status and facilitating real-time monitoring. Liquid biopsies encompass a variety of elements, such as circulating tumor cells, circulating tumor DNA, extracellular vesicles, microRNAs, circulating RNA, tumor platelets, and tumor endothelial cells.
1. Impact of Liquid Biopsy in Early and Differential Diagnosis of Pancreatic Ductal Adenocarcinoma DAC
The challenge in the clinical practice in this pathology (pancreatic intraepithelial neoplasia (PanIN) or early stage PDAC) lies in the early detection to improve the prognosis of PDAC.
L
iquid biopsy (LB)B holds the potential to enhance detection without subjecting the patient to the risks associated with aggressive diagnostic tools
[1][5]. A systematic review and meta-analysis from Zhu and colleagues described the studies performed on LB methods in detecting PDAC
[2][3]. The sensitivity and specificity of LB were 80% and 89%, respectively, with an area under the curve (AUC) of 0.936
[1][2][3,5] (
Figure 1 and
Table 1).
The analysis of various body fluids, including pancreatic juice, saliva and urine, has been investigated for the early detection of PDAC. Mutations in K
risten rat sarcoma (KRAS
) have been detected in the pancreatic juice and in biliary cytobrush specimens, where selective detection has been observed in PDAC patients over benign lesions
[3][17]. Mutation levels of KRAS2 were higher in patients with PDAC compared to chronic pancreatitis (CP). In CP, telomerase activity and alterations in genes such as CDKN2A/p16, TP53 and SMAD4/DPC4 could aid in PDAC diagnosis
[4][5][18,19]. The analysis of biomarkers in saliva offers an easy and noninvasive way to search for mutations in RNAs and miRNAs of genes such as MBD3L2, KRAS, ACRV1 and DPMI, among others, which could assist in differentiating pancreatic cancer patients from CP patients and healthy control
[6][20]. Other biomarkers in RNAs and miRNAs have been described
[7][8][21,22]. Analysis of genetic mutations in urine could also facilitate detection of PDAC
[9][10][23,24].
Importantly, the efficacy of LB to detect PDAC varies depending on the tumor stage and biomarker type. For example,
circ
ulating tumor DNA (ctDNA)tDNA is less frequently detected in patients with resectable disease compared to those with unresectable disease
[1][5]. Here,
rwe
searchers outline the utility of various biomarkers in detecting PDAC within the general population and among specific risk groups (
Figure 1 and
Table 1).
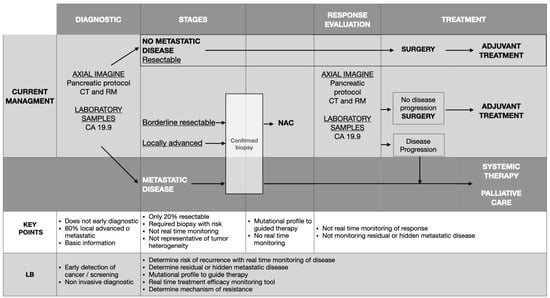
Figure 1. Clinical application of liquid biopsy in pancreatic ductal adenocarcinoma [11]. LB: Liquid biopsy; NAC: Neoadjuvant chemotherapy. Clinical application of liquid biopsy in pancreatic ductal adenocarcinoma [9]. LB: Liquid biopsy; NAC: Neoadjuvant chemotherapy.
Table 1. Comparison between biomarkers of pancreatic ductal adenocarcinoma [12][13][14]. Comparison between biomarkers of pancreatic ductal adenocarcinoma [4,6,8].
| |
ctDNA |
Circulating Tumor CellCs (CTCs) |
Extracellular Vesicles (EVs) |
| Target |
KRAS, TP53, CDKN2A, SMAD4, BRAF, PIK3CA, ADAMTS1, BNC1, 5MC, H2AZ, H2A1.1, H3K4me2, h2ak119ub |
CD45, CEP8, CK, EpCAM |
KRAS, TP53, RNA: miRNA, longRNA
Proteins markers: EFGR, EPCAM, MUC-1, GPC-1, WNT2 |
| Isolation |
Blood |
Blood |
Body fluids |
| Tumor information |
Epigenetic information |
DNA, RNA, Protein |
DNA, RNA, Protein |
| Technological approaches |
qPCR, dPCR, ddPCR, NGS, commercial kits |
Immunoaffinity, Physical methods (size and density) |
Density-based, size-based, affinity-based, commercial kits |
| Advantages |
qPCR: Fast and low-cost
dPCR: High sensitivity/Specificity
NGS: capability to screen for a broad range of genetic variants using high DNA input |
Immunoaffinity: Specific, label-free obtained
Physical methods: Fast, simple, Low-cost, label-free obtained |
Density-based: low cost. Independent of marker expression.
Size-based: Low-cost, fast, Independent of marker expression.
Affinity-based: Specificity. High purity.
Commercial kits: Simple, fast. |
| Disadvantages |
General: No early stages
qPCR: Low sensitivity. Only points mutations.
dPCR: High cost. Only points mutations.
NGS: Variable sensitivity. High cost. |
General: Isolation complex and expensive. Technical variability
Immunoaffinity: capture only one subpopulation. Low purity.
Physical methods: Needs immuno-labeling techniques to distinguish CTCs |
General: Isolation complex by contamination and expensive
Density-based: Time, high volume sample, can damage EVs.
Size based: contamination.
Affinity-based: low sample yield.
Commercial kits: High cost. |
| Sensitivity (S) (%) |
34–71%
KRAS mutations: codons 12, 13, 61, in different stages. |
73–76%
CD45/CEP8
100% Mt, 58% resectable
Anti-EpCAM portal vein Blood |
67% ES, 80% LA, 85% Mt
KRAS mutations in exoDNA
50% ES
GPC1
miRNAs
Increased expression |
| Specificity (Sp) (%) |
75–81%
Mutations KRAS exon 2 |
68%
CD45/CEP8 |
90% ES
GPC1 |
| Combined techniques (%) |
S: 85–98%, Sp: 77–81%
ctDNA (KRAS exon 2) with CA19.9
S: 47%
ctDNA (KRAS MAFs) with CA19.9 |
S: 100%, Sp: 80%
CTCs.with EVs |
NR |
| Application |
No suitable for screening of PDAC
Monitoring postoperative minimal residual disease
Predictor of disease recurrence and prognosis |
Not present in healthy controls
Variable sensitivity in early diagnosis
Excellent specificity.
Follow-up of disease recurrence and prognosis
Functional analysis drug resistance |
The highest sensitivity and specificity in early detection
Evaluated response of resection or any therapy
Biotherapeutic application |
1.1. Circulating Tumor tDNA
Some studies found that cfDNA is detected at higher levels from PDAC patients compared to pancreatic neuroendocrine tumors or CP patient
[15][25] and have been associated with poor disease-specific survival
[15][16][17][25,26,27]. Of all mutated genes detected from ctDNA in PDAC patients, KRAS is the one most frequently found (50–90%). Although mutations can also be found in healthy controls and patients with CP, its mutation levels are significantly higher in PDAC
[16][18][7,26].
In their review, Zhu and colleagues emphasized that although the sensitivity of ctDNA is marginally lower than that of CTCs, ctDNA provides considerably higher specificity
[2][3]. Notably, while the detection of ctDNA is deemed appropriate for the diagnosis of PDAC, it is not considered suitable for screening purposes. The limited sensitivity of ctDNA in early-stage PDAC is attributed to minimal cellular necrosis at this stage, resulting in the release of only a small quantity of ctDNA into the peripheral bloodstream
[2][3].
1.2. Circulating Tumor CellCs
Pancreatic cells can indeed be identified in the bloodstream even before tumor development. In contrast to healthy individuals, these cells are detectable in 33% of patients with cystic lesions
[19][28] and in 73% of those with PDAC
[19][20][28,29]. Furthermore, other studies have noted the presence of CTCs in varying proportions in benign, premalignant, or malignant lesions, but not in healthy controls
[21][30].
The diagnostic efficacy of CTCs, however, has been a topic of debate among researchers due to their inconsistent sensitivity, which ranges from 21% to 100%
[22][31]. In a study by Ankeni and colleagues, a NanoVelcro CTCs microfluidic chip was employed to analyze 100 sequential samples from pretreatment PDAC patients. The results showed CTCs in 54 out of 72 confirmed PDAC patients, demonstrating a sensitivity of 75% and a specificity of 96.4% when used for diagnostic purposes
[23][32].
Given the technical variability in detecting CTCs, some researchers recommend combining the detection of CTCs with other biomarkers to enhance sensitivity up to 100% and specificity to 80%
[24][33]. Although the specificity of CTCs is lower than that of EVs, their utilization still presents considerable diagnostic potential in PDAC detection
[2][3].
1.3. Extracellular Vesicles
EVs from pancreatic cells are easily detectable in peripheral blood owing to their abundant levels, a consequence of the exocrine function of these cells, and possess a longer half-life compared to ctDNA. Interestingly, KRAS mutations in ctDNA were found in 7.4% and 14.8% of healthy donors when tested from exosomal DNA (exoDNA) or cfDNA, respectively
[25][34], and in 13% of CP patients
[26][35]. Research by Melo et al. demonstrated that glypican-1 (GPC1) levels in EVs were significantly higher in PDAC patients compared to those with benign pancreatic diseases or healthy individuals, showcasing remarkable sensitivity and specificity (100%)
[27][36]. Moreover, studies by Zhang et al.
[28][37] and Lewis et al.
[29][38] employed ‘chips’ to detect GPC1, aiming to enhance sensitivity and specificity in distinguishing PDAC from healthy samples. Other studies have shown that combining EVs analysis with CA19-9 could improve specificity
[30][39]. Notably, EVs analysis proves useful for both diagnosing and screening PDAC, offering superior diagnostic value compared to other techniques, partly due to its high AUC of 0.9819
[2][3]. To summarize, among various detection methods, EVs exhibit the highest diagnostic efficacy, sensitivity, and AUC
[2][3].
1.4. miRNAs
miRNAs are noncoding, single-stranded RNA molecules up to 22 nucleotides long that function as posttranscriptional gene expression regulators
[31][40]. Various miRNAs have been utilized to differentiate PDAC patients from those with benign lesions, CP, and healthy controls, and a JAMA-published study reported 38 significantly dysregulated miRNAs in PDAC patients compared to controls
[32][41]. These include miR-223, miR-23b-3p, miR-100, miR-205, miR-192-5p, a six-miRNA panel, miR-483-3p, miR-99 (a and b), miR-21, miR-25, and miR-205, among others. The detection of diverse miRNAs could enhance diagnostic accuracy and distinguish PDAC from healthy individuals
[33][42]. In pancreatic conditions such as intraductal papillary mucinous neoplasm
[34][43] or pancreatic intraepithelial neoplasia
[35][44], miRNAs have been instrumental in differentiating patients with high-grade dysplasia or early-stage PDAC from healthy controls. Importantly, a meta-analysis revealed that miRNAs offer a sensitivity of 79% and specificity of 74% for early PDAC diagnosis. Similar to other biomarkers, combining analysis of miRNAs with CA19-9 analysis improved the quality of data, yielding an AUC of 0.84
[36][45]. Moreover, whilst miRNA analysis from pancreatic juice demonstrated a specificity of 88% and sensitivity of 87%, the inclusion of serum CA19-9 levels enhanced sensitivity to 91% and specificity to 100%
[37][46]. In saliva samples, hsa-miR-21, hsa-miR-23a, hsa-miR-23b, and miR-29c were significantly upregulated in PDAC patients compared to controls, reporting sensitivities of 71.4%, 85.7%, 85.7%, and 57%, respectively, and a specificity of 100%
[38][47].
Numerous studies exploring biomarker combinations in healthy individuals, CP, and PDAC patients
[39][40][48,49] have produced various results, with a common trend pointing towards higher specificity when combining biomarkers. For instance, one study demonstrated that using at least two biomarkers among CA19-9, CTCs, or ctDNA achieved a sensitivity and specificity of approximately 80% and 90%, respectively
[41][42][50,51]. Another study confirmed that combining CTCs with CA19-9 elevated the positive diagnostic rate for PDAC to 97.5%
[43][52].
2. Role of Liquid Biopsy after Resection of Pancreatic Ductal AdenocarcinomaDAC
Surgery stands as the singular potentially curative intervention for PDAC, given the tumor’s notable resistance to chemotherapy, radiation, and immunotherapy. Attaining an R0 resection represents the optimal opportunity for patients to achieve a favorable prognosis, resulting in an enhanced 5-year survival rate ranging from 8% to 25%
[1][2][12][13][14][18][44][45][3,4,5,6,7,8,10,11]. Despite undergoing curative resection, disease recurrence significantly impacts postoperative outcomes, with over 70% of resected PDAC patients succumbing to recurrent disease
[1][2][12][13][14][18][3,4,5,6,7,8]. Consequently, there is a critical need for an effective strategy to identify minimal residual disease (R1) during or postsurgery and to anticipate the risk of recurrence
[45][11]. LB emerges as a promising approach to monitor disease progression in PDAC following surgical intervention
[1][2][12][13][14][18][44][45][3,4,5,6,7,8,10,11] (
Figure 1 and
Table 1).
2.1. Circulating Tumor tDNA
Despite the initial hypothesis suggesting that tumor components are released into the bloodstream following manipulation, a recent meta-analysis revealed that surgical resection of resectable primary tumors plays a role in the negativization of ctDNA
[45][11]. However, this comprehensive analysis failed to establish a significant impact of ctDNA negativization on the overall survival (OS) and disease-free survival (DFS) rates of PDAC patients. The authors emphasized the considerable heterogeneity observed within the analyzed studies, attributing it to variations in postoperative determinations of ctDNA, which extended beyond 24 h after the removal of surgical specimens. Considering the relatively short half-life of ctDNA, ranging from minutes to hours, delayed determinations increase the likelihood of encountering false-negative results. On the other hand, the elevation in ctDNA levels induced by surgical trauma can persist for 2 to 4 weeks, potentially concealing persistent ctDNA in patients experiencing relapse. Consequently, the authors recommended conducting LB between 2 and 4 weeks postsurgery to minimize the risk of false negatives
[1][2][12][13][14][18][3,4,5,6,7,8].
Recent studies have indicated that the detection of ctDNA in preoperative blood samples from PDAC patients may identify candidates for NAC. Additionally, elevated ctDNA levels were associated with an increased risk of death, and patients with a LB after surgery showing as positive for ctDNA exhibited a higher recurrence rate
[45][11]. The persistence of ctDNA positivity postsurgical resection is predictive of a shorter DFS, possibly indicating the presence of occult micrometastases or residual local disease, supporting the consideration of additional adjuvant treatment
[14][18][44][45][7,8,10,11].
2.2. Circulating Tumor CellCs
In a recent randomized trial, the authors implemented a no-touch pancreaticoduodenectomy, involving the manipulation of the tumor only after the complete isolation of vascular and lymphatic drainage vessels
[46][12]. The study reported a reduction in CTCs in the portal vein when employing the no-touch technique but no discernible improvement in OS compared to standard surgery. In contrast, a meta-analysis conducted by Vidal and colleagues failed to demonstrate a decreased release of tumoral components after surgical manipulation employing the no-touch technique, and no superior OS and DFS were observed compared to standard surgery
[45][11].
Importantly, the presence of CTCs has been shown to progressively increase in advanced diseases. For instance, a study revealed that patients with occult metastases of PDAC exhibited significantly higher CTCs counts than those without metastatic disease. Therefore, considering CTC levels becomes crucial in understanding the disease state and thus determining whether NAC should be favored over surgical treatment
[44][10]. Additionally, a prospective study assessed CTC levels in preoperative PDAC patients, establishing a direct correlation between elevated CTC levels and disease recurrence at one year in patients undergoing resection
[14][8].
2.3. Extracellular Vesicles
Several studies have suggested that EVs derived from tumors can serve as indicators of the response to surgery and treatment, offering a potential avenue for a reliable marker in PDAC. Similar to other markers, the levels of miRNAs originating from EVs return to normal within 24 h of PDAC resection. However, persistently elevated levels postsurgery may indicate the presence of hidden metastasis. Such cases warrant vigilant follow-up, and individuals may require additional treatment following surgery
[44][10]. A study investigating miR-451a, miR-4525, and miR-21 from EVs obtained from portal venous blood during pancreatectomy revealed elevated levels emerging as an independent prognostic factor for OS and DFS
[14][8].