Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Tie Zhou and Version 2 by Sirius Huang.
In the absence of early detection and initial treatment, prostate cancer often progresses to an advanced stage, frequently spreading to the bones and significantly impacting patients’ well-being and healthcare resources. Therefore, managing patients with prostate cancer that has spread to the bones often involves using bone-targeted medications like bisphosphonates and denosumab to enhance bone structure and minimize skeletal complications. Additionally, researchers are studying the tumor microenvironment and biomarkers to understand the mechanisms and potential treatment targets for bone metastases in prostate cancer.
- prostate cancer
- bone metastasis
- bone-targeted therapies
- skeletal-related event
1. Introduction
Prostate cancer (PCa) is a prevalent malignant tumor in the United States, ranking second in terms of mortality rate after lung cancer [1]. There exists a significant disparity in the occurrence rate of prostate cancer between China (10.2/100,000) and North America (73.0/100,000), with both the incidence and mortality rates showing a consistent upward trend in recent years [2][3][2,3]. The 2014 China Multicenter Report revealed that a significant proportion of Chinese patients (approximately 30.5%) diagnosed with prostate cancer had already developed distant metastases at the time of initial diagnosis, which is considerably higher compared to the rates observed in North America [4]. Nowadays, the treatment options for patients diagnosed with metastatic prostate cancer (mPCa) have shown significant advancements in recent years. Androgen deprivation therapy (ADT) serves as the primary treatment for this condition. Additional treatment options encompass chemotherapy, new generation hormone therapy, radium-223, and, more recently, radioligand therapy. Special considerations should be directed toward the management of bone health and the prevention of treatment-induced bone loss in these patients [5]. Among individuals diagnosed with castration-resistant prostate cancer (CRPC), bone metastasis is commonly detected in 70% to 90% of patients through imaging examinations [6]. Bone metastases give rise to the occurrence of skeletal-related events (SREs), which encompass severe pain, pathological fracture, spinal cord/intervertebral nerve compression, and hypercalcemia [5]. Preventing and reducing the occurrence of SREs, relieving pain caused by bone metastases, and improving patients’ quality of life are the goals of treatment. The management of bone metastases in prostate cancer has undergone significant advancements due to the enhanced comprehension of the disease’s progression, signaling pathways, mutational characteristics, and mechanisms of drug resistance. Table 1 and Figure 1 summarize the main pathways and mechanisms of action of the principal PC therapeutic agents. However, there exists a dearth of data analysis pertaining to drug trials and their progression over the previous decade.
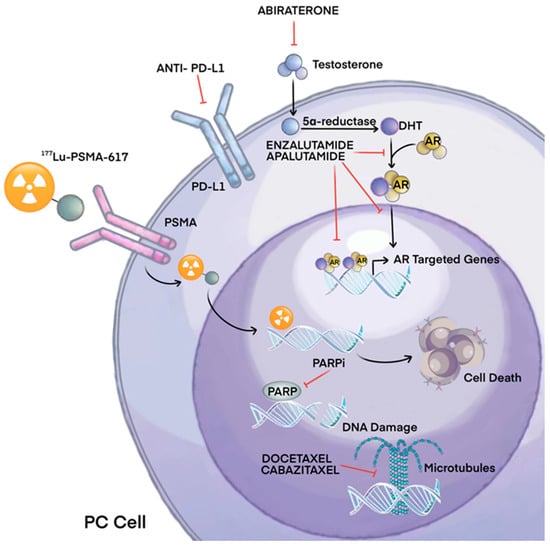
Figure 1.
Main mechanisms of therapeutic agents for prostate cancer.
Table 1.
Drugs and their mechanisms of actions against prostate cancer.
| Drug | Action | Mechanism |
|---|---|---|
| Abiraterone | Inhibition of androgen synthesis | Inhibits CYP17, reduces androgen production |
| Enzalutamide | Antagonization of androgen action | Androgen receptor inhibitor, blocks testosterone effects |
| Bicalutamide | Blockade of the AR | |
| Apalutamide | Prevent AR translocation, DNA binding, and AR–mediated transcription | |
| Docetaxel Cabazitaxel |
Inhibition of mitosis | Tubulin inhibition |
| Radium-223 | Alpha radiation, gamma rays | Targets bone metastases, emits alpha particles |
| 177Lu-PSMA-617 MEDI3726 |
Inhibition of growth signals | Binding and internalization of the PSMA ligands triggers cell death |
| Ipilimumab | Checkpoint (CTLA-4) inhibitor | Increases antitumor T-cell responses |
| Olaparib Rucaparib |
PARP inhibitor | Inhibition of DNA repair |
| Pembrolizumab | PD-1 inhibitor | Regulates T cell activation |
| Sipuleucel-T | Immunotherapy | Autologous vaccine |
| CAR-T | Targeted PSMA |
2. Hormonal Therapy
Enzalutamide is a second-generation androgen receptor antagonist and was initially reported in 2009 [7]. In men with metastatic hormone-sensitive prostate cancer (mHSPC), the ARCHES study demonstrated that enzalutamide exhibited a significant reduction in the risk of mortality when compared to placebo (HR: 0.39, 95% CI 0.30–0.50; p < 0.001). Additionally, enzalutamide was found to be effective in reducing the occurrence of the first symptomatic skeletal events, castration resistance, and pain progression [8]. A post hoc analysis of the ARCHES study provided additional clarification on the effects of enzalutamide in reducing the risk of radiographic progression of bone metastases (HR: 0.33, 95% CI 0.22–0.49) and the risk of bone metastases with lymph node metastases (HR: 0.31, 95% CI 0.21–0.47) when compared to placebo. Still, there was no significant reduction in the risk of lymph node metastasis [9]. PREVAIL, a double-blind, phase III study [10], met its primary endpoint, radiographic progression-free survival, with a significant advantage in the enzalutamide arm (65% versus 14%, p < 0.001). The occurrence of SREs, which was assessed as a secondary endpoint, demonstrated improvement in the enzalutamide group (32% vs. 37%, p < 0.001). Additionally, enzalutamide has shown efficacy in patients with low baseline PSA levels (i.e., <10 ng/mL), including those with ≥4 bone metastases and/or visceral disease and <4 bone metastases without visceral disease [11].
Abiraterone, a CYP17 inhibitor that targets a crucial enzyme involved in androgen synthesis, was assessed in the LATITUDE trial [12]. In this phase III trial, a total of 1199 mCSPC patients were randomly assigned in a 1:1 ratio to receive ADT + abiraterone acetate + prednisone versus ADT + dual placebo. Treatment with abiraterone was associated with a statistically significant survival advantage (not reached vs. 34.7 months), and the median length of radiographic progression-free survival was 33.0 months in the abiraterone group and 14.8 months in the placebo group. A post hoc analysis revealed that abiraterone acetate led to improvements in bone pain, fatigue symptoms, and overall health-related quality of life. Patients in the abiraterone group had a longer median time to worst pain intensity, worst fatigue intensity, and functional deterioration condition [13]. The STAMPEDE trial examined the efficacy of abiraterone acetate in combination with prednisolone and ADT versus ADT alone in patients with locally advanced or metastatic PC. After 3 years of treatment, survival improved (83% versus 76%, HR 0.63; p < 0.001) and the risk of SREs decreased (12% versus 22%, HR 0.46, p < 0.001) in the combination group [14]. Abiraterone was assessed in the COU-AA-302 trial, which examined the efficacy of abiraterone acetate in combination with prednisone compared to placebo and prednisone in mCRPC patients who had not previously received chemotherapy. The pain progression was 26.7 months in the abiraterone group and 18.4 months in the prednisone group (HR, 0.82; 95% CI, 0.67 to 1.00; p < 0.05), and the advantage in radiographic progression-free survival reached statistical significance (16.5 months versus 8.3 months; p < 0.001) [15].
Apalutamide was first described in 2012 as a novel antiandrogen for prostate cancer [16]. The TITAN trial evaluated the therapeutic efficacy of adding oral apalutamide to ADT for the treatment of adult men with metastatic castration-sensitive prostate cancer (mCSPC). The 24-month OS rates were 82.4% in apalutamide plus ADT recipients and 73.5% in placebo plus ADT recipients (p = 0.005). There was no substantial difference between the two groups in the time to the skeletal-related events of prostate cancer [16]. The primary objective of the TITAN study was to assess the therapeutic effectiveness of combining oral apalutamide with ADT (not reached, HR 0.80) [17].
Approximately 8% of CRPC patients have the androgen receptor splice variant-7 (AR-V7) blood biomarker [18], which has been linked to resistance against enzalutamide and abiraterone [19]. Galeterone has been reported to inhibit AR signaling through multiple mechanisms: CYP17 inhibition, AR competitive antagonism, and induction of AR and AR-V7 protein degradation [20]. In a randomized phase III trial [21], CRPC patients with AR-V7 expression were randomly assigned to receive either galeterone or enzalutamide in an open-label manner. However, this trial did not achieve its primary objective due to a high number of patients discontinuing the study as a result of disease progression. Therefore, there is an urgent need for alternative treatments for circulating tumor cells expressing AR-V7 in mCRPC.
Bipolar androgen therapy (BAT) is an emerging treatment option for patients with CRPC. BAT has shown promise in restoring drug sensitivity in some patients, particularly to medications like Abiraterone and Enzalutamide. This therapy has demonstrated significant advantages in the treatment of CRPC patients [22]. The RESTORE trial was a single-arm, multicohort study, focused on CRPC patients. The results from this trial indicated that patients who had previously experienced progression on enzalutamide showed a 52% PSA50 response rate to enzalutamide after undergoing BAT. Similarly, patients who had previously progressed on abiraterone demonstrated a 16% PSA50 response to abiraterone after BAT. However, this study did not investigate the effects of BAT on SREs [23][24][23,24].
More than 50% of prostate cancer patients receiving long-term ADT have significant associated metabolic consequences, such as insulin resistance and metabolic syndrome [25][26][25,26]. A phase II trial observed that the use of high-dose metformin in mCRPC reduced PSA secretion and delayed the progression of prostate cancer [27].A cohort study based on a prostate cancer population showed that patients with hyperlipidemia may have prolonged survival with metformin and statins while undergoing radiotherapy [28]. Ongoing clinical trials will help elucidate the role of metformin in the treatment of locally advanced or metastatic prostate cancer [29][30][29,30].
3. Chemotherapy
In 2004, the United States Food and Drug Administration (FDA) approved the use of Docetaxel, a taxane drug that binds to tubulin, for the treatment of mCRPC [31]. Another taxane drug called cabazitaxel was also approved by the FDA in 2010 as a second-line salvage chemotherapy for prostate cancer [32]. A phase II trial found that a weekly treatment schedule of 10 mg/m2 of docetaxel resulted in a 34.9% prostate-specific antigen (PSA) response rate, with lower toxicity rates of 14.2% neutropenia and 35.7% diarrhea [33]. However, the GETUG-AFU 15 trial suggested that the addition of docetaxel to ADT should not be used as a first-line treatment for mCSPC as it did not improve overall survival [34]. On the other hand, the CHAARTED trial showed that adding docetaxel to ADT in early-stage prostate cancer improved overall survival, particularly in high-volume disease, but did not show a clear survival benefit in low-volume disease [35][36][35,36]. One potential reason for the discrepancy between the GETUG-AFU 15 and CHAARTED trials is the lack of statistical power in the former. The STAMPEDE trial reported a survival benefit with upfront docetaxel in patients with mCSPC, regardless of metastatic burden [37]. According to the National Comprehensive Cancer Network (NCCN) guidelines, patients with high-volume metastatic disease who are suitable for chemotherapy should receive ADT in combination with docetaxel, along with either abiraterone or darolutamide. The ARASENS trial found that adding darolutamide to ADT and docetaxel improved the overall survival of mHSPC patients with a similar rate of side effects compared to using a placebo with ADT and docetaxel [38]. The PEACE-1 trial demonstrated that using abiraterone in combination with ADT improved overall survival and progression-free survival in patients with de novo mCSPC, with only slight increases in treatment-related side effects [39]. Additionally, the findings from the ENZAMET trial suggested that adding enzalutamide should be considered for patients with mCSPC who are treated with docetaxel [40][41][40,41]. While studies have shown the benefits of doublet therapy with ADT plus androgen receptor signaling inhibitors (ARSIs), as well as the benefits of triplet therapy with ADT plus docetaxel and ARSIs, a direct comparison between doublet therapy and triplet therapy for mCSPC has not been conducted [38][39][38,39]. However, patients with low-volume disease appear to have increased treatment benefit from ARSI doublet therapy compared to docetaxel and ADT [42]. It is noteworthy that the overall survival (OS) rate is comparatively lower in African American individuals than in Caucasian individuals among patients diagnosed with prostate cancer. However, after administration of docetaxel, the OS rate in African American patients approached parity with that of Caucasian patients. This phenomenon may be attributed to racial disparities in drug responsiveness. The documented benefits of docetaxel or cabazitaxel in terms of OS are well established. However, there is currently no conclusive evidence regarding their impact on pain management and the potential delay or prevention of SREs in patients with mCRPC [43].
4. Bone-Modifying Agents
Osteoporosis is commonly observed in patients with prostate cancer. Studies have shown that a significant percentage of hormone-naïve PC patients (ranging from 3.9% to 37.8%) develop osteoporosis even before receiving any oncological treatment. This suggests that PC itself may be a risk factor for the loss of bone mineral density (BMD) due to its promotion of bone resorption [44][46]. ADT is designed to reduce testosterone by up to 95% and lower estrogen, but it also causes an increase in bone resorption to altering the balance between osteoblasts and osteoclasts and results in a rapid decline in BMD. The decline in BMD begins shortly after the initiation of ADT and continues throughout the treatment period [45][47]. The duration of ADT is directly proportional to the risk of osteoporotic fractures [46][48].
The efficacy of bone health agents, such as zoledronic acid and denosumab, in reducing the occurrence of SREs and delaying their onset in patients with bone metastases from prostate cancer has been extensively studied. The NCCN guidelines for the treatment of osteoporosis in prostate cancer patients receiving ADT recommend several strategies. They suggest calcium and vitamin D3 supplementation as a standard approach. Additionally, for men aged 50 years and older who have low bone mass in the femoral neck (with T values falling between −1.0 and −2.5), the NCCN advises considering further therapy options such as denosumab or zoledronic acid. Zoledronic acid is the most commonly used bisphosphonate for managing bone metastasis in prostate cancer patients due to its reported ability to prolong the time to SREs and alleviate bone pain [47][49]. Despite having similar rates of overall survival and SREs, zoledronic acid demonstrated superior efficacy in managing pain compared to clodronate [48][50] (Table S1). However, the effectiveness of zoledronic acid varies among studies, and some have yielded inconclusive results. For instance, a phase III clinical trial demonstrated that patients with mCSPC and bone metastases treated with zoledronic acid and ADT experienced a significantly shorter time to the first SRE (18.8 months) compared to those treated with ADT alone [49][51]. Conversely, the ALLIANCE 90202 trial found no association between zoledronic acid use and a reduced risk of SREs in men with mCSPC [50][52]. In TROG 03.04 RADAR trail [51][53], 18 months of androgen suppression plus radiotherapy is a more effective regimen for treating locally advanced prostate cancer, but the addition of zoledronic acid to this regimen does not significantly improve OS. Similarly, the TRAPEZE study reported that zoledronic acid did not prolong OS [52][54]. Moreover, in patients at high risk for localized PCa, zoledronic acid proved to be ineffective in preventing bone metastases [53][55]. Zoledronic acid has been shown to improve BMD when administered at various dosing intervals. In the United States, the approved use of zoledronic acid specifies that it should be used when prostate cancer has progressed despite hormone therapy. For patients with mCRPC and skeletal metastases, zoledronic acid has been utilized in accordance with the EAU guidelines to mitigate the occurrence of SREs [54][56]. The currently approved dose in most clinical trials is 4 mg intravenously every 3–4 weeks [55][56][57][57,58,59].
Numerous trials have examined the effectiveness of zoledronic acid in preventing BMD decline, but none of these trials were designed to detect a difference in fracture risk [58][60]. Denosumab, on the other hand, is a fully humanized monoclonal antibody that binds to and neutralizes RANKL, a protein involved in bone resorption. By inhibiting signaling through its target RANK, denosumab suppresses bone resorption by osteoclasts [59][61]. A post hoc analysis of three phase III trials compared denosumab to zoledronic acid in terms of reducing the risk of SREs, including both first-time and subsequent events [60][62]. The analysis found that denosumab was more effective than zoledronic acid in preventing SREs, regardless of factors such as Eastern Cooperative Oncology Group performance status, location and number of bone metastases, presence or absence of visceral metastases, and urinary N-telopeptide level. The standard dosage for denosumab is 120 mg administered subcutaneously every 4 weeks and there is evidence to suggest that administering bone-modifying agents every 12 weeks instead of every 4 weeks may be equally effective in preventing SREs [61][62][63,64]. Thus, prolonging the interval between doses of bone-modifying agents may help avoid the risk of adverse events such as osteonecrosis of the jaw (ONJ) without compromising SRE prevention.