Glioblastoma (GBM) is the most aggressive and common form of primary brain cancer with a dismal prognosis. Current GBM treatments have not improved patient survival, due to the propensity for tumor cell adaptation and immune evasion, leading to a persistent progression of the disease. In recent years, the tumor microenvironment (TME) has been identified as a critical regulator of these pro-tumorigenic changes, providing a complex array of biomolecular and biophysical signals that facilitate evasion strategies by modulating tumor cells, stromal cells, and immune populations. Efforts to unravel these complex TME interactions are necessary to improve GBM therapy. Immunotherapy is a promising treatment strategy that utilizes a patient’s own immune system for tumor eradication and has exhibited exciting results in many cancer types; however, the highly immunosuppressive interactions between the immune cell populations and the GBM TME continue to present challenges.
- glioblastoma
- immunotherapy
- tumor microenvironment
- biophysics
1. Introduction
2. Biophysical Aspects of the TME
2.1. ECM Composition
Solid tumors comprise a wide range of highly expressed ECM proteins that include laminins, fibronectin, elastin, and fibrillar collagen [48][63]. These proteins provide functionality and stability to the tumor environment for disease progression and accounts for up to 60% of the tumor mass [49][64]. Indeed, the presence of these proteins plays a key role in regulating the pro-invasion and therapeutic resistance within the tumor that help to direct cell migration, adhesion, and proliferation similar to that seen in early development [50][65]. Several ECM proteins of interest in GBM have been identified over the last several years including osteopontin, hyaluronic acid (HA), and laminin and are known to increase invasion potential through mechanotransduction signals transmitted throughout the cytoskeleton [51][52][53][66,67,68]. Further, HA is the primary ECM component in the brain, and it has been strongly implicated in GBM tumor development and depends on the HA molecular weight—high-molecular-weight HA has an anti-tumor effect and low-molecular-weight HA has a pro-tumor effect [52][54][55][56][57][67,69,70,71,72].2.2. ECM Mechanics
Besides ECM composition, the mechanics of the ECM can direct cell behavior [58][73] and tumor malignancy. Increased substrate stiffness has been shown to increase proliferation and single-cell migration in GBM. ECM stiffness can also increase cell adhesiveness, which interestingly reduces collective migration due to dense networks of cell–substrate adhesions [59][60][74,75]. These stiffnesses also affect the density of the matrix and can facilitate primary tumor escape during metastasis [61][76] by providing permissive porous environments to increase cell escape from the tumor or inhibitory dense environments that would confine the cell to the tumor.2.3. Interstitial Fluid Flow
The increased mechanics of the intratumoral space caused by the high stiffness and density can also affect the flow of interstitial fluid throughout the tumor. The flow of interstitial fluid through the tumor exposes the cells to fluid pressure and soluble cues such as pro-angiogenic factors and anti-inflammatory TGF-β1 signals [62][79]. These factors function to inhibit anti-tumor immune cells and promote pro-tumor immune cells by maintaining the inflammation of the tumor to a sustainable level.3. Biophysical TME-Immune Cell Interactions
It has been established that the biophysics of the TME and ECM can regulate cell behavior in a pro-tumorigenic capacity. However, besides cancer cells, other types of cells including the immune cell populations are regulated by the biophysical TME (Figure 1).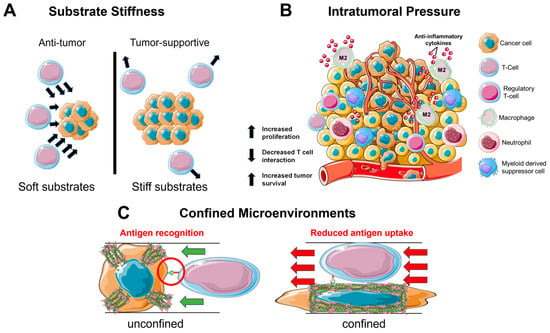
3.1. Substrate Stiffness
3.2. Intratumoral Pressure
In a similar manner to the stiff tumor, an interstitial fluid flow induces pro-tumorigenic effects on the immune cells in the TME (Figure 1B). Tumors often utilize the lymphatic system to invade and metastasize [68][99]. This system specializes in fluid drainage and, therefore, it is not uncommon to find heightened pressure gradients at the junction of tumor and lymphatics. These junctions experience an increased flow and mechanical stress, which serves to cause DNA damage and increase the production of cytokines such as TGF-β1 to reduce inflammation [68][69][70][99,100,101]. Furthermore, the interstitial pressure is sufficient to induce a pro-tumorigenic macrophage phenotype as seen by the upregulation of M2 macrophage markers ArgI, TGM2, and CD206 [71][102]. This development of M2 macrophages further works to inhibit T cell function via the additional TGF-β1 production and expression of immune checkpoint ligands that inactivate infiltrating T cells [72][73][103,104].3.3. Confined Migration
Considering the density of the brain parenchyma, it is unsurprising that GBM is an innately aggressive cancer. For many cell types, migration in a confined environment can lead to DNA damage via nuclear rupture [73][104], which serves as the basis for the development of metastatic cancer [74][111]. During infiltration of the TME, the immune cells will enter a state of confined migration (Figure 1C). Macrophages have been observed to form a protective actin cortex that shields against compressive forces that can damage the nucleus and lead to cell death [75][112]. This enables a more efficient and safe form of migration necessary for patrolling throughout the confined environments. Likewise, T cells navigate a variety of confined spaces as they patrol throughout the body; however, while patrolling, the T cells also interact with antigen-presenting cells. This presents a balance that must be maintained between migrating quickly through an environment and spending enough time in the same location as the antigen-presenting cell to become activated against an antigen [76][113].4. Bioengineering Systems
4.1. Biomaterial Systems
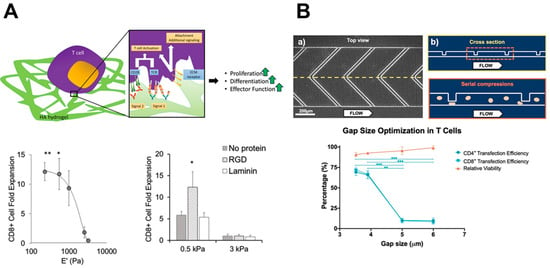
Biomaterials are synthetic or natural materials that can be engineered to mimic physiological and pathological environments and are foundational to investigate cell-ECM interactions. Among the most common biomaterials are hydrogel-culture-based systems due to their versatility in controlling factors such as stiffness, ECM composition, and other biomolecules such as growth factors [77][122]. In the context of solid tumors such as GBM, the most important immune cell functions to consider are tumor infiltration and tumor cell elimination. Hydrogel-based platforms have proven vital in dissecting the interplay between immune cells and the tumor ECM. The mechanosensing capacity of T cells has been interrogated via TCR-mediated activation through the introduction of HA binding [78][123] and the tuning of the stiffness to biomimetic levels [78][79][123,124].4.2. Microfabrication
Microfabrication approaches such as 3D printing and microfluidics represent important tools for studying the contribution of geometric cues as well as observing cell phenomena in a single-cell context. Many studies leverage these tools to decipher the migration mechanisms of immune cells. In the 3D context, CD8+ T cell amoeboid migration operates through a contractility driven mechanism via RhoA activation that is unique to the 2D environment [80][81][82][129,130,131]. Additionally, the T cell transfection efficiency can be modified on microfluidic systems through mechanoporation via stretching to engineer T cells with greater motility, antigen recognition, and antigen elimination [83][84][132,133].4.3. Advanced In Vitro Systems
Creating more complex, biologically relevant in vitro systems serves as an intermediate step before reaching in vivo models. Co-culture models combine multiple cell types into a single culture environment to analyze real-time interactions between the cells, and lab-on-a-chip technology is useful for combining multiple physiological systems to determine how cell processes differ between the environmental changes. Macrophages and microglia are normally susceptible to reprogramming via GBM cues that promote tumor development; yet, when cultured separately, these changes cannot be observed. Therefore, co-culture systems allow for the necessary paracrine and juxtacrine interactions (ephs/ephrins [85][137] or P-selectin/PSGL-1 [86][138]) involved in the bidirectional communication between the tumor and immune cells to occur and be observed. These interactions are intended to help recognize the cancer cells for immune-cell-mediated elimination but are often dysregulated to instead promote tumor survival and development.5. Immunotherapy Applications
From the mechanistic insights gained through bioengineering systems, researchers can leverage these interactions to optimize immunotherapy protocols to increase efficacy and improve patient survival. By engineering the culture expansion platforms of immune cells and the activities of immune cells, efforts to increase the tumoricidal capacity of immune cells are growing. In recent years, many types of cancers have seen significant improvement due to the development of novel immunotherapies, their developments in treating GBM, and the biophysical design of the therapies (Figure 2).