Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Wojciech Kazimierczak and Version 2 by Wendy Huang.
Artificial intelligence (AI) describes the ability of machines to perform tasks that are classified as intelligent. AI can be classified into two main categories: symbolic AI and machine learning (ML). Symbolic AI involves structuring an algorithm in a way that is easily understandable to humans. Machine learning (ML) is the predominant paradigm in the field of AI. The advent of artificial intelligence (AI) in medicine has transformed various medical specialties, including orthodontics. AI has shown promising results in enhancing the accuracy of diagnoses, treatment planning, and predicting treatment outcomes. Its usage in orthodontic practices worldwide has increased with the availability of various AI applications and tools.
- AI
- cephalometric analysis
- orthodontic
- dental diagnostics
- CBCT
1. Introduction
Artificial intelligence (AI), a term first introduced in 1955 by John McCarthy, describes the ability of machines to perform tasks that are classified as intelligent [1]. During these 70 years, there have been cycles of significant optimism associated with the development of AI, alternating with periods of failure, reductions in research funding, and pessimism [2]. The 2015 victory of AlphaGo, a Google-developed AI application, over the “GO” world champion represented a breakthrough [2]. This AI success over a human player sparked further development and interest, which was raised by the introduction of the Chat-GPT in 2022. These events served as precursors to the remarkable growth of AI applications in various fields, including everyday life and medicine [2].
AI algorithms have already proven effective in various medical specialties, surpassing the capabilities of experienced clinicians [3][4][5][6][7][3,4,5,6,7]. These algorithms enable the analysis, organization, visualization, and classification of healthcare data. The development of AI algorithms in medicine has gained momentum in recent years, particularly in radiology, where medical imaging accounts for approximately 85% of FDA-approved AI programs (data for 2023) [8].
In the field of diagnostic imaging, AI can be categorized into three main domains: operational AI, which enhances healthcare delivery; diagnostic AI, which aids in the interpretation of clinical images; and predictive AI, which forecasts future outcomes [9]. Currently, the primary goals of AI in diagnostic imaging are to detect and segment structures and classify pathologies [10]. AI tools can analyze images obtained from various imaging modalities, ranging from X-ray to MRI [11][12][13][14][15][11,12,13,14,15].
Orthodontics, with its emphasis on cephalometric analysis and pretreatment imaging, is particularly well suited for the implementation of AI. However, AI is also being utilized in orthodontics for applications beyond cephalometric analysis. The literature on the use of AI in orthodontics can be divided into five main areas: diagnosis and treatment planning, automated landmark detection and cephalometric analysis, assessment of growth and development, treatment outcome evaluation, and miscellaneous applications [16].
The number of AI companies in the healthcare industry has experienced a remarkable increase, indicating significant growth in commercial prospects for AI [9]. AI tools are no longer limited to researchers and scientists involved in research and development projects. They are now accessible through commercially available web-based products as well. In orthodontics, the adoption of AI has led to the creation of various AI-based programs, such as WeDoCeph (Audax, Ljubljana, Slovenia), WebCeph (Assemble Circle, Seoul, Republic of Korea), and CephX (ORCA Dental AI, Las Vegas, NV, USA). These systems can automatically identify cephalometric landmarks, compute angles and distances, and generate cephalometric reports with significant findings. AI programs are now easily accessible on mobile devices, making AI tools widely available and promoting equal access for all interested users. As a result, orthodontic practices and scientific researchers utilizing AI applications have notably increased. However, this accessibility has also sparked concerns about patient safety, especially when AI is used for diagnosis and treatment.
2. Dental Diagnostics
The use of medical imaging methods is essential in dental patient care because they aid in the clinical diagnosis of pathologies related to teeth and their surrounding structures [17][18][19][30,31,32]. Radiological methods, such as orthopantomograms (OPGs) and cone-beam computed tomography (CBCT), play crucial roles in orthodontic diagnosis, treatment planning, and monitoring [20][21][22][33,34,35]. However, with the increasing number of radiological examinations being performed [23][36], there is a need for a comprehensive tool to support the process of radiological diagnosis. In response to this demand, multimodular diagnostic systems based on AI have emerged. One such AI-based system, developed by Diagnocat Ltd. (San Francisco, CA, USA), utilizes CNNs and provides precise and comprehensive dental diagnostics. The system enables tooth segmentation and enumeration, oral pathology diagnosis (including periapical lesions and caries), and volumetric assessment. Several scientific papers have validated the diagnostic performance of this program, demonstrating its high efficacy and accuracy [24][25][26][27][28][37,38,39,40,41]. A study by Orhan et al. [24][37] reported that the AI system achieved 92.8% accuracy in the detection of periapical lesions in CBCT images and showed no statistically significant difference in volumetric measurements compared to manual methods. Similarly, a study evaluating the diagnostic accuracy of the program for periapical lesion detection on periapical radiographs (PRs) yielded comparable results [25][38]. However, conflicting results have also been reported, particularly regarding the accuracy of AI in the assessment of periapical lesions in OPGs [29][42]. In a recent study by Ezhov (2021) [30][43], the overall diagnostic performance of two groups, one aided by AI and the other unaided, was compared in oral CBCT evaluation. The AI system used in this researchtudy included modules for tooth and jaw segmentation, tooth localization and enumeration, periodontitis, caries, and periapical lesion detection. The results showed that the AI system significantly improved the diagnostic capabilities of dentists, with higher sensitivity and specificity values observed in the AI-aided group than in the unaided group (sensitivity: 0.8537 vs. 0.7672; specificity: 0.9672 vs. 0.9616). Several systematic reviews and meta-analyses have been conducted on the utilization of AI for identifying caries and periapical lucencies [31][32][33][34][35][36][37][38][39][40][41][42][44,45,46,47,48,49,50,51,52,53,54,55]. In a recent comprehensive study by Rahimi [41][54], the accuracy of classification models for caries detection was evaluated across 48 studies. The reported diagnostic accuracy varied significantly based on the imaging modality, ranging from 68% to 99.2%. The diagnostic odds ratio, which indicates the effectiveness of the test, also varied greatly from 2.27 to 32,767 across studies. The study concluded that deep learning models show promise for caries detection and may aid clinical workflows. One of the earliest meta-analyses conducted in 2019 on the computer-aided detection of radiolucent lesions in the maxillofacial region [33][46] yielded a pooled accuracy estimate of 88.75% (95% CI = 85.19–92.30); however, only four studies were included. A more recent meta-analysis by Sadr [39][52] included 18 studies and revealed that the pooled sensitivity and specificity were 0.925 (95% CI, 0.862–0.960) and 0.852 (95% CI, 0.810–0.885), respectively. The researcheuthors concluded that deep learning showed highly accurate results in detecting periapical radiolucent lesions in dental radiographs. These findings suggest that multimodal AI programs may serve as first-line diagnostic aids and decision support systems, improving patient care at multiple levels. Figure 1 shows a sample of the Diagnocat report.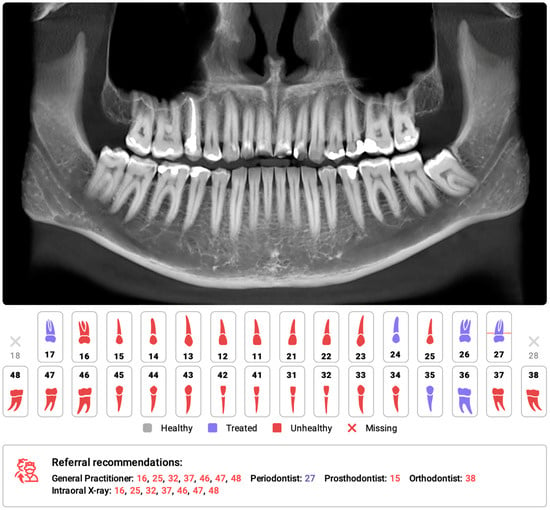
Figure 1. Part of the automatic diagnostic report from a CBCT scan was obtained prior to orthodontic treatment on a 24-year-old male. The software automatically identified the absence of teeth 18 and 28, as well as changes in the remaining teeth, primarily consisting of attrition and the presence of dental fillings. The program has recommended further consultations as necessary.
3. Cephalometric Analysis
Cephalometric analysis (CA) is an important diagnostic tool in orthodontics that has been in use since 1931 [43][56]. Over the years, advancements in technology have revolutionized CA by replacing manual assessments with digital software. This approach simplifies the measurement process and provides an automatic display of the analysis results. Automated CA has been shown to be more stable and repeatable than manual analyses, which rely heavily on operator-dependent landmark identification and often exhibit significant variability [44][45][46][47][57,58,59,60]. Accurate and repeatable landmark identification is crucial for reliable CA outcomes. Several studies have demonstrated the effectiveness of AI in identifying cephalometric landmarks. Although lateral radiography remains the most commonly used method in CA, recent AI advancements have sparked renewed interest in the use of cone-beam computed tomography (CBCT) [48][61]. The effectiveness of AI in identifying cephalometric landmarks has been studied since 1998 [49][62]. Numerous studies have used various automated methods and have consistently achieved high accuracy in landmark identification [46][47][50][51][52][53][54][55][56][57][58][59][59,60,63,64,65,66,67,68,69,70,71,72]. A recent study by Hwang et al. (2020) [47][60] concluded that automated cephalometric landmark identification can be as reliable as an experienced human reader. Similarly, Kim et al. [52][65], Lee et al. [58][71], and Dobratulin et al. [50][63] achieved landmark definition accuracies between 88% and 92% using AI. These researcheuthors also found that, compared with manual methods, AI methods demonstrated greater accuracy in landmark identification and reduced the time and human labor required. In other studies conducted by Hwang et al. [46][59] and Yu et al. [57][70], the researcheuthors found no statistically significant differences between the results of automated cephalometric analysis and those calculated via manually identified landmarks. Additionally, AI has been shown to significantly improve the workflow of practices, reducing analysis time by up to 80 times compared to manual analysis [59][72]. Figure 2 shows the definitions of the sampled cephalometric landmarks.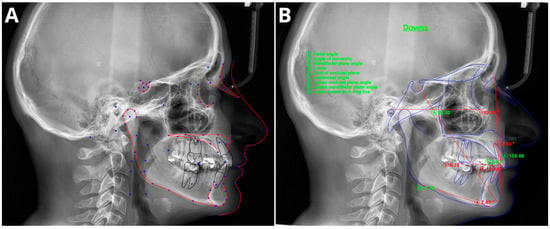
Figure 2. Sample of automatic cephalometric landmark tracings performed using CephX (A) and WebCeph (B) on an 18-year-old male. The results of Downs cephalometric analysis superimposed on tracings (B). Measurements outside the standard range marked in red and with asterix *.