1. Introduction
Hypertension represents a massive global health issue and is one of the most important cardiovascular risk factors. Hypertension-mediated organ damage (HMOD) is common in patients with severe or long-standing hypertension and is also prevalent in less severe hypertension, even in asymptomatic individuals with elevated blood pressure
[1]. It is important to note that at any given blood pressure category above the normal or optimal, the presence of HMOD is associated with a 2- to 3-fold increase in the cardiovascular risk
[2]. Up to 40% of newly diagnosed hypertensive patients already have HMOD, predominantly functional and structural alterations of heart, kidneys, eyes, brain, and peripheral arteries
[3].
Hypertension is a well-established risk factor for the development of coronary microvascular dysfunction (CMD)
[4]. The constant high pressure within the larger arteries can lead to damage and remodeling of the smallest arteries and arterioles in the microcirculation, capillaries, and venules, affecting their ability to regulate blood flow
[5]. This leads to structural and functional remodeling of the coronary microcirculation, in which endothelial dysfunction is one of the most important pathogenetic mechanisms
[6]. The endothelium plays a crucial role in regulating blood vessel tone and controlling blood flow. In hypertensive individuals, endothelial dysfunction significantly contributes to the development of CMD, which progressively leads to increased resistance in coronary microcirculation and limited blood flow, causing a reduced oxygen supply to the myocardium
[7]. This is why the finding of myocardial ischemia as a result of CMD is relatively common in patients with hypertension, especially in patients with hypertensive heart disease (HHD). Many additional risk factors also contribute to the development of CMD in hypertensive patients, including metabolic syndrome, diabetes mellitus, hyperlipidemia, smoking, and others
[8][9][10][8,9,10]. As the development of hypertensive heart disease progresses, left ventricular hypertrophy is more pronounced, consequently leading to more severe impairment of coronary microcirculation. These changes, accompanied by myocardial fibrosis, lead to an increased risk of heart failure with both preserved (HFpEF) and reduced ejection fraction (HFrEF)
[11][12][11,12]. This is why coronary microvascular dysfunction significantly affects the morbidity and mortality of patients, demanding more purposeful diagnostic and therapeutic algorithms.
2. Diagnostics for Coronary Microvascular Dysfunction in Patients with Hypertension
In recent years, several important diagnostic algorithms have been presented regarding CMD that aim to integrate both non-invasive and invasive modalities
[13][61]. The diagnostic algorithm in patients with suspected CMD starts with the exclusion of significant epicardial coronary artery disease. Although CMD can be present in patients with obstructive CAD, the presence of CMD in the absence of obstructive CAD is extremely important to diagnose, especially in patients with additional risk factors for the development of adverse cardiovascular events, primarily heart failure
[14][62]. In patients with microvascular angina, non-invasive diagnostic imaging modalities, primarily echocardiography and cardiac magnetic resonance (CMR), are important for the evaluation of alternative causes of chest pain, including structural and inflammatory conditions
[15][63]. Patients with a negative coronary angiogram, a positive stress test for myocardial ischemia, and additional risk factors for the development of CMD (especially those with hypertensive heart disease) should be considered for non-invasive and invasive investigation of CMD.
2.1. Non-Invasive Diagnostics
2.1.1. Echocardiography
Conventional echocardiographic stress tests have limited utility in the diagnosis of CMD, as significant inter-observer variability is present in cases with low to moderate ischemia burden, resulting in hypokinesia
[16][64]. The use of echocardiography in detecting coronary microvascular dysfunction mainly relies on myocardial contrast echocardiography and the estimation of myocardial blood flow (MBF) or coronary flow velocity reserve using pulsed-wave Doppler sampling of the proximal left anterior descending coronary artery. Nowadays, CFVR has higher diagnostic accuracy and better correlation with intracoronary Doppler wire-based techniques, especially in patients with HFpEF, as demonstrated in the PROMIS-HFpEF trial
[17][65]. Numerous studies have investigated the prognostic significance of CFVR in patients with hypertension, demonstrating an impairment in microvascular vasodilatation capacity even in the early stages of the disease
[18][19][66,67]. The study by Volz et al. showed that CFVR was significantly lower in patients with resistant hypertension than in individuals with non-resistant hypertension, indicating a more severe impairment of coronary microvascular function that could account for the increased risk of adverse outcomes
[18][66]. The main disadvantages of MBF assessment of CFVR are the presence of artifacts and high inter-observer variability, especially in obese patients and patients with lung disease. However, these methods can be helpful as inexpensive methods in the initial assessment of patients with CMD. In addition to its significant role in the diagnosis of obstructive coronary artery disease, strain assessment is becoming equally important in patients with CMD
[20][68]. Aside from CFRV, novel protocols of stress echocardiography incorporate the estimation of global longitudinal strain in rest and peak stress to increase sensitivity and specificity of this estimation
[21][69]. A study by Jovanovic et al. demonstrated that resting, peak, and ΔLVGLS were all significantly impaired in female patients with coronary microvascular dysfunction and slow coronary flow
[22][70].
2.1.2. Computerized Tomography (CT)
The role of CT coronary angiography is to primarily exclude the existence of significant epicardial coronary artery disease. Recent technical and software advancements provide the possibility to follow the first pass of contrast through the myocardium at frequent intervals and estimate the absolute myocardial flow. Two types of CT myocardial perfusion protocols can be performed, static and dynamic. Static CT myocardial perfusion requires a lower amount of radiation and prospective ECG gating. However, only qualitative and semiquantitative evaluation is possible with this technique. Dynamic CT perfusion allows the estimation of myocardial perfusion in different layers of the myocardium and a complete quantitative myocardial blood flow evaluation, providing evidence of reduced subendocardial perfusion in patients with CMD
[23][71]. Novel techniques combining CTA-derived FFR and estimation of myocardial perfusion can provide an accurate anatomical and functional assessment of both the myocardium and the coronary circulation within one examination, which can be significant, especially in patients with hypertensive heart disease
[24][72]. Studies that investigated myocardial perfusion and coronary-volume-to-left-ventricular-mass ratio showed promising results in diagnosing patients with CMD
[25][73]. However, the results in patients with hypertension are controversial. The study by van Rosendal and colleagues demonstrated that patients with hypertension and increased left ventricular (LV) mass did not have reduced coronary vascular volume that could be associated with the presence of abnormal perfusion reserve
[26][74]. This can also be a result of predominantly functional impairment of coronary microcirculation, as well as a lack of the estimation of coronary vasodilator reserve.
2.1.3. Single-Photon Emission Computed Tomography (SPECT)
With recent advancements in high-sensitivity cardiac cameras and radiotracers, dynamic SPECT found its place in the quantification of myocardial blood flow and the assessment of CMD. Nowadays, iodinated rotenone compounds and solid-state, high-sensitivity cadmium–zinc–telluride detectors can detect the first-pass blood perfusion of a tracer and its extraction into the myocardium. This allows the quantification of myocardial blood flow and myocardial perfusion reserve with better accuracy and fewer artifacts.
[27][75]. This protocol results in better spatial resolution and higher sensitivity, resulting in shorter acquisition time and lower radiation exposure. Zhang et al. demonstrated that quantitative SPECT analysis of myocardial blood flow provides prognostic value in patients with ischemia and no obstructive coronary artery disease (INOCA)
[28][76]. However, as the diagnostic and prognostic significance of SPECT is still under PET and CMR, it can allow clinically useful measurements in the absence of previously mentioned modalities.
2.1.4. Positron Emission Tomography (PET)
The main advantages of PET in the estimation of CMD are global and regional measurements of perfusion, quantitative MBF, and function, both under stress and at rest. By estimating myocardial perfusion during rest and stress, it can accurately estimate myocardial perfusion reserve (MPR), a value that has an excellent correlation with invasive modalities and also with adverse outcomes
[29][77]. As it can estimate both epicardial and microvascular coronary distribution, PET can improve risk stratification for patients being investigated for ischemia. Studies of patients with hypertension revealed that the “endogen” type of CMD, predominantly related to alterations in resting myocardial blood flow, is more prevalent in these patients
[30][78]. High radiation exposure and cost are the main disadvantages of this method. In comparison to cardiac magnetic resonance, PET lacks the possibility to additionally provide a sophisticated myocardial tissue characterization.
2.1.5. Cardiac Magnetic Resonance (CMR)
Cardiac magnetic resonance has an important place in cardiac diagnostics, considering that it is a non-invasive method during which, with high specificity and sensitivity, the existence of both significant epicardial obstructive coronary disease and coronary microvascular dysfunction can be confirmed or excluded. Diagnostics of coronary microvascular dysfunction via CMR can be established by analyzing myocardial perfusion during the stress test in comparison with myocardial perfusion at rest, which actually evaluates the vasodilatory flow reserve
[31][79]. During the stress perfusion test, various vasodilator agents can be used, including adenosine, regadenoson, or dipyridamole. Stress CMR accurately assesses myocardial ischemia, myocardial viability, and cardiac function, all in one examination. Methods within cardiac magnetic resonance to evaluate the existence of coronary microvascular dysfunction can be qualitative and quantitative [
Figure 1]. A qualitative method of assessment includes visual evaluation of the perfusion during stress, whereby a characteristic diffuse subendocardial perfusion defect is observed. The drawback of the qualitative evaluation of the stress perfusion study is the extremely low sensitivity of only 41% and the inability to clearly differentiate between patients who have a pronounced degree of coronary microvascular dysfunction and patients who have multi-vessel CAD, which can also cause a diffuse subendocardial defect in perfusion
[32][80]. If coronary angiography was not performed before the stress perfusion test, in the differentiation of coronary microvascular dysfunction and obstructive coronary disease, late gadolinium enhancement (LGE) sequences can be helpful, on which the zones of the LGE phenomenon are not registered in patients with microvascular dysfunction. Novel CMR diagnostic modalities, myocardial tissue mapping, and extracellular volume fraction (ECV) are important in estimating the presence and degree of interstitial fibrosis, which can be significant in risk stratification, especially in patients with hypertension who have left ventricular hypertrophy, diastolic dysfunction, and consequently an increased risk of HFpEF
[33][81].
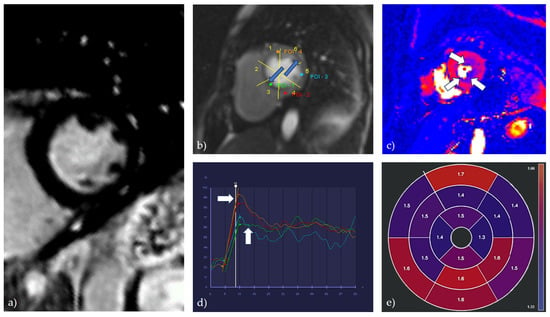
Figure 1. A combination of qualitative, semiquantitative, and quantitative methods for the evaluation of CMR stress perfusion study in a patient with coronary microvascular dysfunction. (a) LGE PSIR sequence, short axis view; showing the absence of LGE phenomenon; (b) qualitative analysis of stress perfusion; a global subendocardial perfusion defect is observed (marked by blue arrows); (c) perfusion map during stress perfusion study, short axis section, medial level; a global subendocardial perfusion defect is observed (marked by white arrows); (d) semiquantitative analysis (flow/time curve), short axis section, medial level; the perfusion curves indicate a global perfusion defect in the subendocardial layers of the myocardium (green and blue curves) in comparison to the subepicardial layers (red and orange curves) (marked by white arrows); (e) quantitative analysis of stress perfusion; diffusely reduced normalized values of myocardial perfusion reserve (MPRI) are observed.
Semiquantitative and, especially, quantitative methods of evaluation of stress perfusion are used for definitive assessment. Quantitative methods of assessing coronary microvascular dysfunction can, in addition to establishing a diagnosis, evaluate the severity of the disease, as well as monitor the effect of different therapeutic modalities. New sophisticated and fully automated CMR methods for the analysis of myocardial perfusion enable high diagnostic accuracy, strong prognostic significance, and complete independence from the level of staff training
[34][82]. The basic parameter for the analysis is the value of the blood flow through the myocardium (myocardial blood flow—MBF), which is analyzed both at rest (rest perfusion) and under stress (stress perfusion). Patients with global stress MBF below 2.25 mL/g/min without visual defects in perfusion are likely to have coronary microvascular dysfunction
[35][83]. The difference in myocardial blood flow at rest and under stress represents the myocardial perfusion reserve (MPR), whose indexed value (MPRI) is the most sensitive parameter in the diagnosis of coronary microvascular dysfunction
[36][84]. The accuracy of this method can be significantly increased by analyzing the myocardial perfusion reserve in the subendocardial layer (MPRendo), bearing in mind that the subendocardial layer of the myocardium is the most sensitive to the existence of ischemia
[37][85]. The values of these parameters can be fully evaluated and quantified using pixelated perfusion maps at the level of individual segments according to the 16-segment model of the left ventricle. This kind of analysis makes it possible to establish a diagnosis with high sensitivity and specificity and also to differentiate the existence of obstructive coronary disease from coronary microvascular dysfunction. Clinically relevant values of the above-mentioned parameters for the diagnosis of coronary microvascular dysfunction can be registered even in the absence of qualitative changes in perfusion. In studies that used a fully quantitative assessment of stress perfusion to diagnose CMD, an excellent correlation was shown with the values of invasively measured coronary flow parameters (dominantly with the value of the coronary flow reserve—CFR) and with the value of the index of microvascular resistance (IMR)
[38][39][86,87]. In terms of clinical outcomes, stress MBF and MPR/MPRI have been shown to be associated with serious adverse cardiovascular events and mortality
[40][88].
Non-contrast-based CMR techniques for perfusion estimation are the future of CMD diagnostics as they are more sensitive and have even higher diagnostic accuracy than today’s widely available techniques. They are based on the principle of estimating myocardial tissue oxygenation by specific protocols or comparing the changes in myocardial native T1 time during the rest and stress perfusion study
[41][89]. These techniques can overlook different limitations of conventional techniques, including imaging artifacts, long scan time, inter-observer variability, problems with the absolute quantitation of myocardial blood flow, and restricted use in patients with chronic kidney disease.
2.2. Invasive Diagnostics
The invasive modalities in the diagnostics of CMD are mainly based on the estimation of coronary blood flow. Coronary blood flow can be estimated by Doppler (measuring coronary flow velocity) or thermodilution (measuring cold bolus transit time), each with a different sensor-tipped intracoronary guidewire
[42][90]. In regard to the endothelium function, coronary blood flow can be estimated in response to adenosine (non-endothelium-dependent function) or in response to acetylcholine to evaluate the presence of vasospastic angina (endothelium-dependent function). CFR values (the ratio of the maximal or hyperemic flow to the resting flow) of less than 2.0–2.5 (thermodilution) or 2.5 (Doppler) in the absence of epicardial obstructive coronary artery disease indicate the presence of coronary microvascular dysfunction
[43][91]. The ratio between myocardial perfusion reserve and flow can be used to calculate coronary microvascular resistance (CMR). In the thermodilution-based method, the index of microvascular resistance (IMR) with a cut-off value of >25 is significant for confirming the presence of CMD, while in the Doppler-based technique, the resulting index is called hyperemic microvascular resistance (hMR), with the cut-off value of ≤2.5 mmHg/cm/s
[44][45][92,93]. Regarding endothelium-dependent microvascular dysfunction, the diagnosis can be made if there is an increase of less than 50% in coronary blood flow, accompanied by ischemic ECG changes and angina symptoms, and in the absence of epicardial vasoconstriction. It is important to have in mind that patients with CMD may have both endothelium-dependent and -independent types of microvascular dysfunction. Studies evaluating the invasive indices of CMD in patients with HFpEF revealed abnormalities in coronary flow and resistance
[46][94]. The study by Dryer et al. revealed that HFpEF patients had lower CFR and higher IMR values than the control group. These patients were also older and had higher values of NT-proBNP and higher left ventricular end-diastolic pressure, while 93% of them had hypertension as one of the comorbidities
[47][95].
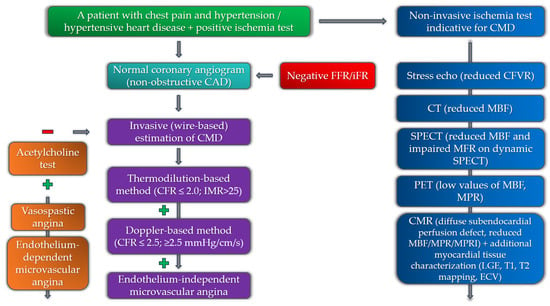
The diagnostic algorithm for the estimation of CMD among patients with chest pain and hypertension, involving both non-invasive and invasive modalities, is presented in Figure 2.
Figure 2. Diagnostic algorithm for the estimation of coronary microvascular dysfunction among hypertensive patients with chest pain (negative and positive symbols correspond to a negative or positive test in the diagnostic algorithm).
Considering the variety of imaging modalities in diagnostics for CMD, it is notable to mention that in patients with hypertension, the indices of arterial stiffness are independently related to microvascular dysfunction
[48][49][50][96,97,98]. A recent study by Aursulesei Onofrei et al. demonstrated a predictive value of the subendocardial viability ratio (SEVR), also known as the Buckberg index, in hypertensive patients with CMD. This parameter of arterial stiffness, which represents an index of myocardial oxygen supply and demand, is significant in the assessment of long-term cardiovascular risk and is independently associated with age, abdominal circumference, and Framingham risk score
[51][99].