Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Paula Tilley and Version 2 by Lindsay Dong.
Decision making consists of gathering quality data in order to correctly assess a situation and determine the best course of action. This process is a fundamental part of medicine and is what enables practitioners to accurately diagnose diseases and select appropriate treatment protocols. Despite severe equine asthma (SEA) being a highly prevalent lower respiratory disease amongst equids, clinicians still struggle with the optimization of routine diagnostic procedures. The use of several ancillary diagnostic tests has been reported for disease identification and monitoring, but many are only suitable for research purposes or lack practicality for everyday use.
- equine
- severe equine asthma
- diagnosis
- clinical history
1. Introduction
Severe equine asthma (SEA) is a chronic insidious respiratory disease which commonly affects mature adult horses [1][2][1,2]. Its estimated prevalence in the northern hemisphere is 20%, but the number of affected individuals continues to rise [3][4][5][3,4,5].
The precise immunological pathways of this multifactorial disease are complex and not yet fully understood [6][7][8][9][10][11][12][6,7,8,9,10,11,12], but it is known that when susceptible individuals are exposed to high concentrations of respirable particles they develop inflammation, bronchospasm and airway hyperreactivity [13][14][15][16][13,14,15,16]. Consequently these animals develop increased respiratory effort at rest, cough and nasal discharge which, depending on inflammation severity, may impact athletic performance and the horse’s well-being [17][18][17,18].
According to the type of inflammatory triggers associated with SEA exacerbation, two major disease phenotypes have been described [1]. The stable-associated SEA mainly involves exposure to organic respirable particles found indoors during the colder months, such as in bedding materials, hay and straw [19][20][21][19,20,21], whilst the pasture-associated SEA occurs in animals kept at pasture during the warmer season due to exposure to pollen [22][23][24][22,23,24].
However, inflammation can be triggered by a large number of molecules with a synergistic effect, such as LPS, pollen, mites, fungi spores, or even plastic particles, which can be found in the horses’ habitat [19][20][21][25][26][27][28][19,20,21,25,26,27,28]. Because antigen avoidance can be extremely difficult to achieve, affected animals tend to present recurrent episodes of disease exacerbation [29].
2. Diagnosis
In evidence-based medicine, reaching a correct diagnosis is paramount to produce individualized patient care and optimize clinical outcome [30][31]. Every patient is unique, as their medical conditions can vary in severity, underlying causes, and treatment response. Thus, by accurately identifying the patient’s condition, veterinarians can tailor their treatment plans to address the specific needs of the animal and their owner, taking into account risks and potential benefits, ultimately maximizing the chances of therapeutic success and animal well-being [29][31][29,32]. Therefore, diagnosis must be sought using the most up-to-date research and clinical guidelines in the decision-making process. This approach ensures that patients are subjected to the most relevant clinical interventions and receive treatments that have been proven effective [30][32][30,31]. Also, regarding the practitioner, evidence-based medicine is also the best way to efficiently allocate resources and contribute to continuous learning and improvement in healthcare practice.2.1. History, Clinical Signs and Clinical Scores
Severely asthmatic horses will have a history of recurrent respiratory disease with clinical signs being triggered by exposure to specific environmental factors [1]. Often these signs will be seasonal with coughing or labored breathing occurring during spring or autumn. Some horses will also develop clinical signs when performing physical exercise in dusty arenas or when moved to stables with poor air quality [33][34][33,34] which is frequently associated with dusty bedding materials, hay or straw and poor ventilation [35][36][37][35,36,37]. Thus, it is important to carefully examine the horses’ environment but also to inquire about any recently made changes, since some owners may have decided to alter the animals’ environment but have forgotten to report it during the initial consultation. Most commonly, owners will report that in response to being fed poor quality hay the horse will exhibit bouts of cough [38][39][38,39]. Two different phenotypes have been reported in SEA which means that asthmatic horses can develop clinical signs when exposed to stable environmental conditions (fungal spores, organic dust, mites, endotoxins, among others) or when exposed to a pasture environment (pollen and fungal spores) [4][19][40][41][4,19,40,41]. Identifying the horses’ phenotype will determine the best treatment protocol for these animals, and intradermal testing can be useful for constructing an individualized allergen eviction protocol [42][43][42,43]. The clinical signs associated with SEA are quite distinctive [39][44][39,44], which can lead to the temptation of making a presumptive diagnosis based only on the patient’s clinical history and physical examination. Nonetheless, this should be discouraged since it can lead to an erroneous diagnosis especially in horses examined during disease remission or with low grade airway hyperreactivity. Severely asthmatic horses have a history of chronic and persistent cough, which can be seasonal, associated with stabling and hay feeding or pasture [45]. Close inspection of the affected horses’ living quarters and feed will normally reveal the triggering factor. Airway inflammation, hyperreactivity and obstruction result in cough, exercise intolerance, increased respiratory effort at rest and nasal discharge [17][43][46][17,43,46], and the severity of the exhibited clinical signs tend to correlate with the degree and persistence of the inflammatory process [18][47][48][18,47,48]. Cough is usually the first clinical sign reported by owners and although the onset of exercise intolerance precedes it [49], the latter is not always reported early on. This could be related to the expected athletic level of the affected horse, since low grade inflammation may not impair the performance of less strenuous physical activities [50]. With disease progression the severity of cough increases and paroxysmal bouts of cough are typically observed [39][51][39,51]. The associated airway obstruction results in overt respiratory distress with consequent modification of the respiratory pattern, characterized by a short inspiration followed by prolonged exhalation and abdominal lift [52]. Affected animals present increased abdominal effort, with consequent hypertrophy of the external oblique muscles (‘heave line’) and nasal flaring as an attempt to reduce upper airway resistance [17][18][47][53][17,18,47,53]. Changes in mucus rheology along with its decreased clearance result in the accumulation of secretions in the tracheobronchial tree [54][55][54,55]. However, due to the regular swallowing of these secretions, horses only exhibit nasal discharge occasionally [56]. Thoracic auscultation of affected animals will reveal increased bronchovesicular sounds, end-expiratory wheezes due to airway narrowing, and inspiratory crackles caused by the opening of collapsed airways. An expanded pulmonary field can also be auscultated due to lung hyperinflation, secondary to air entrapment in the alveoli [1][2][57][1,2,60]. In some cases, lung auscultation will be unusually silent despite the horse exhibiting substantial respiratory effort due to a remarkable compromise of airflow associated with significant airway obstruction [57][60]. Loss of body mass and cachexia can also occur in horses with extreme respiratory distress due to a combination of reduced food intake and increased energy expenditure to overcome the expiratory obstruction [50][58][59][50,61,62]. However, these scores alone can be insufficient, since mild or subclinical cases of severe equine asthma have little or no clinical signs despite maintaining some degree of airway inflammation and hyperreactivity [39][44][45][60][39,44,45,64]. Although scores based on nasal flaring and abdominal effort correlate with airway dysfunction, exercise intolerance does not, and cough may not occur during disease remission [47][53][61][47,53,65]. The main limitation of clinical sign scores is therefore the correct diagnosis of severely asthmatic horses when in disease remission, making other ancillary diagnostic tests crucial for accurate disease characterization and exclusion of other alternative diagnoses [44][46][53][44,46,53]. Nonetheless, they can be useful in the initial triage and for the continuous assessment of treatment response, without resorting to more invasive diagnostic methods. Furthermore, methods like the Horse Owner Assessed Respiratory Signs Index (HOARSI) [39][46][39,46], and the Visual Analog Scale (VAS) [62][70], can be particularly useful for triage since they rely on information reported by horse owners to help identify the presence of respiratory disease. The HOARSI questionnaire scoring system is based on clinical history and on cough frequency, nasal discharge, breathing at rest and the horse’s performance [15].2.2. Diagnostic Imaging
Radiography and ultrasonography are routinely used ancillary diagnostic tests in equine ambulatory practice, since both are non-invasive and well accepted by horses [63][64][71,72]. In SEA, the radiographic findings have been found to correlate with the clinical signs and disease severity [17]. SEA-affected horses exhibit lung pattern changes, such as increased bronchovascular, interstitial and bronchial interstitial lung patterns, along with thickening of tracheal and bronchial walls [17][65][17,73]. In extreme cases, when disease progression results in lung remodeling, interstitial infiltration, increased lung radiopacity and bronchiectasis can also be observed [66][67][74,75]. Ultrasound examination allows the clinician to attain more detailed information about the surface of the lung, including the assessment of effusion and its characteristics. However the most common ultrasonographic finding in severely asthmatic horses is the presence of comet tails which are non-specific artifacts associated with inflammation [68][69][70][79,80,81].2.3. Endoscopy
Respiratory endoscopy alone or when combined with other sampling techniques can provide insight about the equine upper and lower airways [54][71][72][54,84,85]. Thus it can contribute to the characterization of SEA and to the exclusion of other differentials [1][17][55][72][1,17,55,85]. Endoscopic examination of severely asthmatic horses will reveal the presence of mucus in the trachea and bronchi and thickening of the carina (tracheal septum). The presence of bronchospasm and mucosal hyperemia associated with inflammation can also be assessed [17][55][73][74][75][76][77][17,55,86,87,88,89,90]. Tracheal secretions will usually form a small pool at the lowest point of the trachea. However, decreased mucus clearance and altered rheology increases the amount of mucus observed and mucus strings can be observed in the lateral and dorsal aspects of the trachea [55][78][55,91]. Most endoscopic scoring systems assess the quantity and quality of tracheal mucus [17][73][74][75][77][17,86,87,88,90], and mucus accumulation was found to correlate with clinical scores [79][92], cough frequency [51] and cytological indicators of airway inflammation [55].2.4. Lung Function Tests
Pulmonary function testing has become an important tool in the evaluation of the respiratory system since it provides information about ventilation and the dynamics of this system [63][80][71,93]. They are considered the gold standard for the diagnosis of asthma both in human and equine medicine [81][94]. In SEA they contribute to disease diagnosis and assessment of disease severity as well as treatment response. Nevertheless, no single test can be considered perfect, as they all have their strengths and weaknesses, and their selection will be determined by the clinician’s needs, their practicality and availability. Arterial blood gas analysis assesses lung gas exchange and can be used in an ambulatory setting [82][95]. Severely asthmatic horses commonly present only hypoxemia, but lower values of pH and increased values of PaCO2 have also been reported [18][83][84][85][86][18,96,97,98,99]. Its main disadvantage is that it lacks sensitivity for recognizing animals in remission [86][99]. The change in pleural pressure (ΔPpl), assessed by an oesophageal balloon catheter, is considered the gold standard for the diagnosis of SEA. The measured values can be interpreted on their own, with ΔPpl > 15 cm H2O being considered the cut off value for disease diagnosis [1][46][1,46]. This method can easily be used in an ambulatory setting, but in the authors’ experience some owners may be reticent to allow this test to be performed on their horses due to its invasive nature. When combined with a pneumotachograph, standard lung mechanics can be assessed, namely dynamic compliance (Cdyn), pulmonary resistance (RL), and work of breathing (W). Airway obstruction results in increased RL, W and ΔPpl, and decreased Cdyn [1][53][87][1,53,100]. Flowmetrics is based in boxless plethysmography and it combines respiratory inductance plethysmography (RIP) with pneumotachography [88][103]. This system, which has been specifically developed for equines and was suited for field testing [89][104], is no longer commercially available. It had a sensitivity similar to that of pleural pressure but, when combined with histamine bronchoprovocation, allowed the detection of horses in disease remission [18][46][90][91][18,46,105,106]. Lung function testing can be associated with either a histamine or bronchodilator challenge [80][93]. Airway hyperreactivity, the reversible narrowing of airways in response to a bronchoconstrictor stimulus, such as histamine, occurs in all asthmatic horses, especially during disease exacerbation but is also present in cases of mild obstruction without apparent clinical signs [1][18][46][89][90][92][93][94][1,18,46,104,105,107,108,109]. When asthmatic horses present with a severe compromise of baseline pulmonary function, it is recommended to perform a bronchodilator challenge instead [2][59][2,62]. A bronchodilator is administered (e.g., albuterol 450–900 μg) after a base-line reading and 15 min later pulmonary function is re-assessed [1][80][1,93]. Within 10 min, a 50% improvement of airway resistance should occur in SEA-affected horses in exacerbation [80][93]. Furthermore, both the maximum value and the magnitude of the observed bronchodilation can also predict, to some degree, the future therapeutic response. The use of spirometry [44][95][96][97][44,110,111,112], electrical impedance tomography [98][113], and impulse oscillation system (IOS) for assessing the dynamics of equine lower airways have shown promising results, particularly IOS, which has been reported to differentiate severely asthmatic horses in remission from healthy controls [99][100][101][102][114,115,116,117].2.5. Cytology
In equine ambulatory medicine, airway cytology remains a fundamental technique for diagnosing and monitoring SEA. It provides insight into the inflammatory status of airways and although it is not considered the gold standard for the diagnosis of this disease, its practicality in an ambulatory context has rendered this ancillary diagnostic test popular. Cytological samples can be collected using a wide variety of methods, including brush cytology, tracheal wash (TW), bronchoalveolar lavage fluid (BALF) or even bronchial biopsies [103][104][105][106][118,119,120,121]. Of these methods, BALF cytology is considered to be the one which most accurately reflects the cellular populations of the bronchi and alveoli and the consequent degree of inflammation found in the horses’ lungs [105][107][108][120,122,123]. Sampling can easily be performed transendoscopicaly or ‘blindly’, via a balloon catheter, by instilling a volume of 250 to 500 mL of saline and a minimum of 400 cells should be counted [2][18][105][109][110][2,18,120,124,125]. BALF samples of healthy animals have <400 cells/μL and a superficial foam layer, indicating the presence of pulmonary surfactant. Alveolar macrophages (40–70%) and lymphocytes (30–60%) are the most commonly observed immune cells followed by neutrophils (<5%), mast cells (<2%) and eosinophils (<1%) [1]. The cytological profile of the severely asthmatic horse is usually characterized by neutrophilia (>20% neutrophils) and a reduction in macrophage and lymphocyte percentages [1][17][18][111][112][113][1,17,18,126,127,128]. An increased amount of mucus is also observed which can form Curschmann’s spirals [114][115][57,129]. BALF differential cell counts correlate well with airway obstruction and hyperresponsiveness, and a higher percentage of neutrophils is associated with greater disease severity, coughing and worse mucus scores [17][47][51][115][116][17,47,51,129,130]. During clinical remission, affected horses maintain a slightly elevated neutrophil percentage [117][63], and despite corticosteroid treatment, BALF neutrophilia can persist when severely asthmatic horses continue to be exposed to the offending respirable particles [40][118][119][120][40,131,132,133]. Furthermore, it has been reported that the percentage of neutrophils in BALF can be used to classify the severity of SEA, as it correlates well with the clinical signs exhibited by asthmatic horses, changes observed in thoracic x-rays, mucus scores determined through endoscopy and airway remodeling [17][112][17,127].2.6. SEA Staging
One of the main challenges of managing a severely asthmatic patient is continuously monitoring disease severity and response to treatment. An initial detailed characterization of the disease may help select the best therapeutic protocol and optimize environmental management catering to the horses’ and owners’ individualized needs [81][94]. Staging methods were developed to help clinicians gather information about disease severity by combining history, physical examination and a variety of ancillary diagnostic tests. A relatively complete SEA clinical staging method has been published, which encompasses clinical history reported by the owners and clinical signs observed during clinical examination, namely cough frequency, nasal flare and abdominal lift. It also uses ancillary diagnostic tests to quantify airway inflammation and remodeling, such as thoracic x-ray, endoscopy and BALF cytology [17]. This staging method has to be carried out in a hospital and only evaluates the present condition of the horse and does not take into account reported history An alternative staging system for ambulatory practice that included lung function assessment was later developed [18]. This method included data of the horses’ physical examination (clinical score), BALF cytology (neutrophil percentage), arterial blood oxygen pressure (PaO2), pleural pressure (ΔPpl) and histamine bronchoprovocation (maximum tolerated concentration). All the diagnostic procedures could easily be performed in the field, since all the equipment used was portable.2.7. SEA Characterization
Although the role of immunoglobulin E (IgE) in the pathophysiology of SEA remains controversial, differences in allergen-specific IgE concentrations in the sera and BALF between healthy and SEA-affected horses have been reported [26][121][122][123][124][26,140,141,142,143]. The measurement of allergen-specific IgE concentrations has helped ascertain the association between SEA and sensitization to fungi and mites [26][121][125][26,140,144]. Intradermal tests (IDT) are used to assess the patient’s reaction to an allergen. It requires the injection of specific allergens intradermally and if the horse is sensitized, a local allergic reaction occurs (papule). In SEA-affected horses the use of IDT allowed the identification of allergen sensitization [43][122][43,141]. Lo Feudo and colleagues reported that insects, the mite Dermatophagoides spp. and dog epithelium were the major allergen profiles associated with SEA [43].3. Diagnostic Flow-Chart
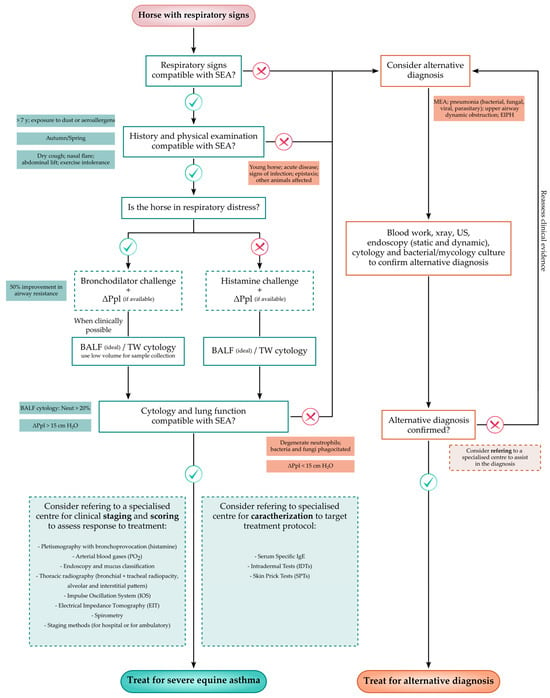
Because horses affected by severe equine asthma may not exhibit clinical signs during disease remission, disease diagnosis can be challenging, particularly to the less experienced practitioner. Thus, a flow-chart which aims to assist in the recognition of severely asthmatic horses by including the main steps required to correctly diagnose the disease, is proposed in Figure 1.Figure 1. Flow-chart proposal for the diagnosis of severe equine asthma to be used in everyday veterinary practice [17][18][42][43][55][63][102][17,18,42,43,55,71,117]. MEA—Mild/Moderate Equine Asthma; EIPH—Exercise Induced Pulmonary Hemorrhage; BALF—Bronchoalveolar Lavage Fluid; TW—Tracheal Wash; ΔPpl—Change in pleural Pressure (indirect); SEA—Severe Equine Asthma; and Neut—Neutrophils.