Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Lorcán Mason and Version 2 by Rita Xu.
Sleep is viewed as essential to the recuperation process and is distinguished as an active participant in recovery through its involvement in growth, repair, regeneration, and immunity. Furthermore, the literature has shown that the sleep of athletes impacts elements of athletic performance including both physical and cognitive performance, recovery, injury risk, and mental well-being. For sleep to have a restorative effect on the body, it must meet an individual’s sleep needs whilst also lasting for an adequate duration and being of adequate quality, which is age-dependent.
- adolescent
- athletes
- sleep
- nutrition
1. Introduction
Sleep can be defined as a reversible behavioural state of impaired consciousness through a reduction in sensory and motor activity [1][2][3][4][5][1,2,3,4,5]. Sleep is regarded as an active regulatory process [6] and facilitates the proper functioning of the brain and cognitive performance while also regulating physiological functions including substrate and energy metabolism [7][8][9][7,8,9], cardiovascular function [10][11][10,11], appetite [12], endocrine function [13][14][13,14], and immune function [15]. Several facilitating theories for sleep have been hypothesised [5][16][5,16], including the regeneration of immune and endocrine function, the nervous system, and metabolic cost of living, and aids in cognitive development and synaptic plasticity [17]. As such, sleep is viewed as essential to the recuperation process [3][18][3,18] and is distinguished as an active participant in recovery through its involvement in growth, repair, regeneration, and immunity [5]. Furthermore, the literature has shown that the sleep of athletes impacts elements of athletic performance including both physical and cognitive performance, recovery, injury risk, and mental well-being [4][19][20][21][22][23][4,19,20,21,22,23].
The architecture of sleep is organised into multiple 90-min series of one rapid-eye-movement (REM) and three non-REM sleep phases (N1, N2, and N3) [24][25][26][24,25,26]. Non-REM and REM sleep are distinct in nature and are characterised by brainwave activity, eye movement, cardiac rhythm, muscle tone, breath rate, and arousal thresholds [27][28][27,28]. REM sleep facilitates neurological regeneration, learning, memory, and emotional regulation [27][29][30][27,29,30]. Non-REM sleep is a three-phased process whereby the propensity to wake (the arousal threshold) is lowest during the first phase and progressively increases through to the highest point in the final phase (N3) [27][28][27,28] and can be characterised by the wave activity of the brain [27][31][27,31]. Non-REM sleep functions to support the regeneration of the nervous system, conserve energy, release anabolic hormones that augment protein synthesis to facilitate muscle recovery [32][33][32,33], and mobilise free fatty acids for ATP production [34]. For a detailed breakdown of the brainwave characteristics of the sleep cycle, readers should refer to the AASM manual for the scoring of sleep and associated events [25], and the principles and practices of sleep medicine [27].
2. Importance of Sleep Health
Sleep health is defined as an individualised and context-specific multidimensional pattern of sleep and wakefulness that supports physical and mental well-being [35] and is an integral component of not only living a healthy lifestyle [36][37][36,37] but also of adaptation and recovery [3][27][32][38][39][3,27,32,38,39]. The relationship between sleep and recovery in athletes can be viewed in terms of three key factors that affect restoration processes: 1. sleep duration (total sleep requirements including napping); 2. sleep quality (total sleep absent of sleep disorders, environmental disturbances, or sleep fragmentation); 3. sleep phase (circadian timing of sleep during the light–dark cycle) [39][40][39,40]. During adolescence, the psychosocial and societal pressures experienced may result in adverse sleep health and reduced recovery capacity [41][42][41,42]. This is due to sleep deficiencies, which have a negative impact on health and are linked to increases in all-cause mortality and disease risk [43]. Sleep deprivation (an insufficient sleep duration compared to the basal level) and disturbances (the inability to initiate and/or maintain the sleep–cycle) are also risk factors for adverse health, recovery, and injury risk in athletic populations [39][40][44][45][46][47][48][39,40,44,45,46,47,48]. For sleep to have a restorative effect on the body, it must meet an individual’s sleep needs whilst also lasting for an adequate duration and being of adequate quality, which is age-dependent [46]. Sleep needs can be defined as the optimum quantity of sleep required to maintain alertness and function throughout daily living [5]. Sleep duration can be influenced by exogenous and endogenous environmental characteristics, which adds complexity to defining an “optimal” sleep pattern due to high inter-individual differences [49][50][51][49,50,51]. Peripheral tissues contain molecular clocks within each cell that dictate the expression of clock-controlled genes in a period (the required time for a cortical neuron oscillation) or phase (waking time in relation to the light cycle) [49][52][49,52]. Processes controlled by circadian rhythms also influence sleep duration; thus, the time at which sleep occurs in the light cycle also has an integral role in sleep duration [50][53][54][50,53,54]. The difference between sleep needs and actual sleep duration is known as sleep debt [5].3. Sleep Adaptations during Adolescence
The chronotype that defines the expression of individual circadian rhythmicity [55] may similarly shift during adolescence [56][57][58][59][60][56,57,58,59,60] due to the greater robustness to increased sleep pressure [61] and environmental factors that increase evening alertness [42]. An individual’s chronotype is mainly dictated by their genetic makeup; however, environmental and societal factors also affect the chronotype [55][62][55,62]. Cross-sectional research has evidenced that during adolescence, the distribution of the chronotype shifts toward the evening chronotype, reverting back to the earlier chronotypes post-maturation [56][57][58][59][60][56,57,58,59,60]. As sleep needs change over the lifespan, The National Sleep Foundation has published guidelines for age-dependent sleep durations, which includes recommendations for the following: adolescents (8–10 h), adults (7–9 h), and older adults (7–8 h) [46]. The literature has suggested that athletes have increased sleep needs, and thus the general recommendations may not be sufficient for athletic populations [23][63][23,63]. Therefore, a more individualised approach accounting for overall sleep health may be more appropriate for addressing sleep needs in individuals including athletes [23][35][63][23,35,63]. To feel rested, the literature has demonstrated that elite athletes need ~8.3 h of sleep [64][65][64,65]. Moreover, adolescent athletes achieve, on average, ~6.3 h [47][66][67][47,66,67] of sleep, demonstrating a discrepancy between sleep recommendations and actual sleep achieved [42][68][69][42,68,69]. Sleep–wake cycles also undergo development during adolescence whereby adaptation occurs in sleep regulation during this phase [68]. These adaptations to sleep regulation increase sleep pressure tolerance (reduced adenosine accumulation) [70][71][72][70,71,72] and are driven by the maturation of physiological, psychological, and cognitive functioning along with delays in circadian rhythmicity [73], thus creating an environment for inadequate sleep influenced by external factors associated with adolescence (Figure 1) [41][42][73][74][41,42,73,74]. This results in ever-decreasing time spent asleep during the ages of 15–18 years, with research reporting a decrease of ~1.5–3 h during this period [70][75][76][70,75,76]. Despite this, an adolescents sleep needs (pressure dissipation) under free living conditions does not appear to alter from the recommended ~9.25 h [42], irrespective of maturation status [77][78][79][77,78,79], thus attributing the decline to environmental factors as opposed to biological factors [73][80][73,80].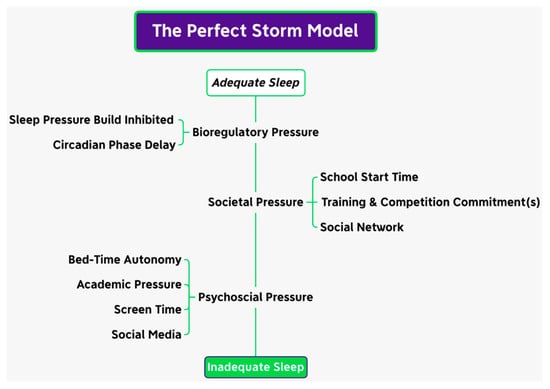
Figure 1. The perfect storm model.