Proteins and peptides are potential therapeutic agents, but their physiochemical properties make their use as drug substances challenging. Hydrogels are hydrophilic polymeric networks that can swell and retain high amounts of water or biological fluids without being dissolved. Due to their biocompatibility, their porous structure, which enables the transport of various peptides and proteins, and their protective effect against degradation, hydrogels have gained prominence as ideal carriers for these molecules’ delivery. Particularly, stimuli-responsive hydrogels exhibit physicochemical transitions in response to subtle modifications in the surrounding environment, leading to the controlled release of entrapped proteins or peptides.
- stimuli-responsive hydrogels
- proteins
- peptides
- protein delivery
1. Introduction
2. Therapeutic Proteins
2.1. Characteristics
Peptides and proteins are essential biological macromolecules that have a central role inside cells during enzyme catalysis, transportation, signal transduction, gene regulation, and immunity-related functions [10]. These compounds are also involved in several pathological conditions, including cancer, diabetes, and hypertension. Therefore, considering their diversity of functions and participation in the control of various diseases, proteins and peptides are promising therapeutic agents [11][12]. Since the approval of the first protein used as an active substance—human recombinant insulin, Humulin®—in 1982 by the U.S. Food and Drug Administration (FDA), several therapeutic proteins have been approved for clinical usage, and others are in the process of development [1][2]. Therapeutic proteins can be used as drugs to (i) substitute a protein that is abnormal or deficient, (ii) increase an existing pathway, (iii) provide a new function or activity, and (iv) interfere with a molecule or organism [13]. Peptides and proteins consist of amino acid units joined together by peptide bonds. Whereas peptides contain two to fifty amino acids, macromolecules with more than fifty amino acids are known as proteins. The sequence of amino acids in their structure is designated as the primary structure [14]. Following the interaction and folding of amino acid chains, higher levels of organization arise, namely secondary, tertiary, and quaternary structures [15]. The functional characteristics of proteins rely on their three-dimensional (3D) conformation. As the 3D structure depends on the primary structure, any difference in the latter may produce a protein that is unable to perform its function [10]. Therapeutic proteins include molecules ranging in size from 1 to 50 kDa to much larger proteins like monoclonal antibodies (mAbs) with around 150 kDa; thus, even the smallest of these molecules exceed in size the so-called conventional drugs, such as aspirin (Figure 1) [16][17][18].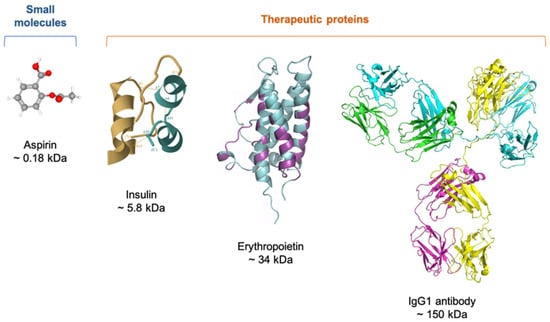
2.2. Delivery of Therapeutic Proteins
2.2.1. Parenteral Route
Therapeutic peptides and proteins are mostly administered by intravenous (IV), subcutaneous (SC), and intramuscular (IM) routes [21][22]. Although medicines can be given intravenously as a bolus, proteins are frequently administered as an infusion [23]. With the IV route, it is possible to achieve an immediate physiological response due to the complete delivery of the administrated proteins to the systemic circulation, avoiding the first-pass metabolism [24]. Notwithstanding its high bioavailability, IV administration is invasive and often painful. Moreover, treatment with high doses, as in the case of antibodies, requires infusion and, thus, visits to the hospital, which increases the overall cost of intravenously given drugs [23]. For some polypeptides and proteins, SC administration poses an alternative to the IV route while also bypassing the first-pass metabolism. Furthermore, as the SC approach could allow patients to self-administer proteins [23], patient preference and adherence are improved, resulting in overall cost savings. Regardless of the benefits of SC-administrated proteins, it still represents an invasive route and demands patients know how to take their medication safely. Additionally, SC injection is restricted to the maximum volume of 2.0 mL because higher volumes would cause rapid changes in the hydrostatic pressure that are perceived as painful [25]. Although such a volume is usually adequate for administering peptides due to their potency, high concentrations are often necessary if proteins are the case. For instance, some antibody solutions at higher concentrations exhibit high viscosity, which might increase injection time and discomfort at the site of injection, with a negative impact on patient compliance [26].2.2.2. Oral Route
The preference for the oral route for drug delivery can be attributed to its ease of administration and noninvasive nature [27]. Nevertheless, delivering peptides and proteins by the oral route is very challenging. The GIT contains large quantities of several enzymes, such as pepsin, trypsin, and chymotrypsin, and bile salts, which may elicit premature leakage and degradation of therapeutic proteins [28]. Moreover, the pH values in the GIT vary considerably from highly acidic (pH 2.0–4.0) in the stomach to pH ~5.5 in the duodenum, ~6.0 in the jejunum, 7.2–8.0 in the ileum, and ~6.5 in the colon, also adding difficulty for oral delivery [29]. Besides lubricating and protecting the cell layer, the thick mucus layer covering the intestinal epithelium acts as a physical barrier to the absorption of drugs, hindering contact with epithelial cells and, thus, drug transport [30]. Molecules can be electrostatically trapped in mucus by virtue of its mucin proteins and proteolytic enzymes in abundance [31]. In addition to the mucus layer, the intestinal epithelium represents a second physical barrier, consisting of a continuous monolayer of epithelial cells, such as enterocytes, goblet cells, Paneth cells, and microfold cells [28][31]. This cellular barrier regulates the transport of nutrients and proteins across the gut lumen and the bloodstream or lymphatic system [31]. The permeation of proteins and peptides between adjacent intestinal cells, designated paracellular transport, is prevented by tight junctions, having an estimated average pore radius of 8–13 Å [31][32]. There are only a few commercially available therapeutic proteins for administration via oral route. One of the first peptide drugs approved by FDA for oral delivery is linaclotide (Linzess®), approved in 2012, which is both acid- and pepsin-resistant and used to treat patients with irritable bowel syndrome and chronic constipation. In 2017, semaglutide (Rybelsus®) was the first oral glucagon-like peptide-1 (GLP-1) approved for type 2 diabetes treatment [30].2.2.3. Nasal Route
In general, the nasal route is best suited for drug delivery as it is noninvasive and the nasal mucosa is easily accessible, considering that the epithelial barrier is thin, porous, and highly vascularized [1]. Since the nasal venous system provides direct access to the systemic circulation, the loss of drug by the hepatic first-pass metabolism can be prevented [33]. Like the intestinal epithelium, the nasal epithelium is the main physical obstacle to the passage of proteins and peptides due to their low membrane permeability [34]. It is noteworthy that nasal mucociliary clearance is a primary defense mechanism of the lungs, in which mucus and its foreign, potentially harmful substances are removed from the respiratory tract. Knowing that the mucus layer is renewed every 15–30 min, the contact time between the protein or peptide and the nasal epithelium is thus limited [35].2.2.4. Pulmonary Route
In addition to noninvasiveness and hepatic first-pass metabolism avoidance, other advantages of the pulmonary route for drug delivery that merit attention and intensive research include (i) the large surface area of lungs, (ii) a very thin alveolar epithelium, and (iii) a rich vascular supply, allowing for rapid systemic absorption [1][34]. However, some factors affect the delivery efficacy of inhaled proteins and peptides, with the primary barrier for inhaled particle deposition being the highly branching structure of the lung [16]. The rate and extent of this process depend significantly on the physicochemical properties of aerosol particles, especially the diameter of a particle in airflow, referred to as aerodynamic diameter [34][36]. Whereas particles with aerodynamic diameters ranging from 1 to 5 μm are deposited in the lower respiratory tract, those with diameters greater than 10 μm are deposited in the oropharyngeal region [16]. Particles exhaled during tidal breathing are under 1 μm [37]. After their deposition in the lungs, therapeutic proteins can be removed by either mucociliary clearance or alveolar macrophage uptake via pinocytosis [16][38]. The latter is size-dependent and becomes more relevant to large proteins (≥40 kDa) owing to their slower transport and absorption across the alveolo-capillary barrier. Alveolar macrophage uptake may not have such an impact on small proteins and peptides (≤25 kDa) as they are readily absorbed from airspaces [38]. Therapeutic proteins also encounter enzymes in the lungs but undergo less degradation compared to the GIT [39]. It is established that proteins and peptides with molecular weights around 6–50 kDa have good bioavailability following inhalation [1][16][40].2.2.5. Ocular Route
It is the route of choice to deliver drugs directly to the ocular tissue [23]. Bearing in mind how accessible the front of the eye is, it comes as no surprise that topical instillation of eyedrops is often selected to treat diseases affecting the anterior segment of the eye, including the cornea, conjunctiva, aqueous humor, iris, ciliary body, and lens [41]. Nevertheless, less than 5% of a topically applied drug reaches deeper ocular tissues because reflex blinking and increased tear turnover collectively lead to poor drug retention and permeation [42][43]. The nasolacrimal duct drains the excess volume into the systemic circulation [42]. The rest of the protein or peptide faces the corneal epithelial barrier, formed by five to seven cell layers, also limiting its penetration [44].2.2.6. Transdermal Route
Skin delivery of proteins and peptides may be efficient since it bypasses the liver, allows for sustained-release effect, and has less proteolytic activity than other mucosal routes [45]. Sustained release may overcome the need for frequent injections if the protein or peptide has a short in vivo half-life [46]. Seeing that the primary function of the skin is to protect the body against exogenous substances, achieving the permeation of protein molecules through the skin is undoubtedly a challenge [34]. Acting as the first and principal barrier to the transdermal route, the topmost layer of the skin, designated stratum corneum, consists of keratinocytes embedded in a lipid matrix, highly organized in a “brick-and-mortar” formation [1][45].3. Hydrogels
3.1. Definition
Hydrogels are 3D, hydrophilic polymeric networks that can swell and retain significant amounts of water or biological fluids without being dissolved [47]. Over the last few decades, hydrogels have been widely used as tissue engineering scaffolds, wound dressings, medical adhesives, and contact lenses. Additionally, hydrogels are becoming increasingly attractive as vehicles for protein delivery due to their desirable properties. Hydrogels are similar in structure to the natural extracellular matrix and enable the physical incorporation of peptides and proteins [8][48]. The crosslinked nature of hydrogels is beneficial for transporting peptides and proteins, as it prevents large foreign molecules from interacting with the encapsulated proteins, thus promoting their retention in circulation without immune rejection.3.2. Stimuli-Responsive Polymers
Stimuli-responsive hydrogels exhibit rapid physicochemical transitions in response to subtle variations in the surrounding environment, leading to the release of the entrapped molecules in a controlled manner [49]. Also termed “smart” polymers, stimuli-responsive polymers respond to external stimuli with reversible changes as they return to their original state after the stimulus is removed [50]. As illustrated in Figure 2, their macroscopic response can be a change in solubility, swelling/shrinking, or switching between hydrophilic/lipophilic, depending on whether the “smart” polymer chains are dissolved in an aqueous solvent (sol state), crosslinked forming a hydrogel, or grafted onto/bound to a surface [51].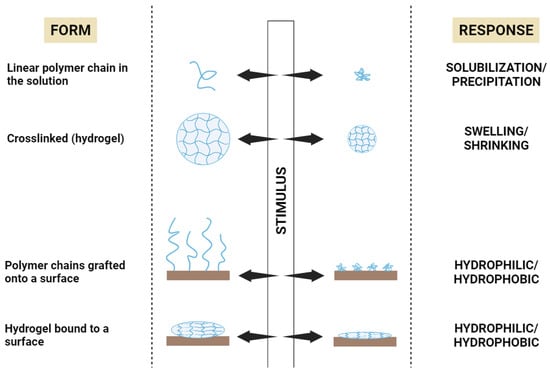
3.2.1. Temperature-Responsive Polymers
3.2.2. pH-Responsive Polymers
The use of pH-responsive polymers in drug delivery systems takes into consideration that pH differences exist in the human body under normal or pathological conditions. For instance, as previously mentioned, the pH of the GIT varies greatly, with the stomach being strongly acidic and the intestine alkaline. Therefore, some pH-responsive polymers can be used to prevent gastric degradation and premature release in the stomach upon reaching the intestine3.2.3. Ionic Strength-Responsive Polymers
Gelation can occur as a response to alterations in the ionic content of the surrounding medium if ionic strength-responsive polymers are involved3.2.4. Biomolecule-Responsive Polymers
Biomolecule-responsive hydrogels can undergo structural transition in response to specific target biomolecules, such as glucose, proteins, nucleic acids, and polypeptides3.2.5. Enzyme-Responsive Polymers
Enzymes are increasingly used as stimuli to trigger structural transformations in hydrogels. To understand this, one should acknowledge that many medical conditions are associated with altered expression of proteins, more precisely overexpressed enzymes in diseased tissues3.2.6. Dual and Multiple Stimuli-Responsive Polymers
On some occasions, polymer materials with a single responsiveness may not fully serve the therapeutic purpose in a complex physiological or pathological microenvironment4. Stimuli-Responsive Hydrogels for Protein Delivery
In a strategy to deal with the problems of protein delivery in the stomach, Lima et al.
[78]
chose alginate as the hydrogel matrix and bovine serum albumin (BSA) as a model protein. The resulting hydrogel showed biocompatibility and pH-dependent BSA release and swelling profile, reaching the highest value of swelling at pH 7.4. The overall results suggested that the performance of this alginate-based hydrogel as an oral drug delivery system would be excellent.
Knowing that keratinocyte growth factor (KGF) repairs potently epithelial tissue, Xu et al.References
- Bajracharya, R.; Song, J.G.; Back, S.Y.; Han, H.K. Recent Advancements in Non-Invasive Formulations for Protein Drug Delivery. Comput. Struct. Biotechnol. J. 2019, 17, 1290–1308.
- Walsh, G. Biopharmaceutical benchmarks 2018. Nat. Biotechnol. 2018, 36, 1136–1145.
- Asfour, M.H. Advanced trends in protein and peptide drug delivery: A special emphasis on aquasomes and microneedles techniques. Drug Deliv. Transl. Res. 2021, 11, 1–23.
- Florence, A.T.; Attwood, D. Physicochemical Principles of Pharmacy: In Manufacture, Formulation and Clinical Use, 6th ed.; Pharmaceutical Press: London, UK, 2015.
- Lin, J.H. Pharmacokinetics of biotech drugs: Peptides, proteins and monoclonal antibodies. Curr. Drug Metab. 2009, 10, 661–691.
- Irianti, M.K.; Rahmasari, R.; Arifianti, A.E.; Iswandana, R. Non-invasive strategies for protein drug delivery: Oral, transdermal, and pulmonary. J. Appl. Pharm. Sci. 2020, 10, 166–179.
- Vermonden, T.; Censi, R.; Hennink, W.E. Hydrogels for protein delivery. Chem. Rev. 2012, 112, 2853–2888.
- Bae, K.H.; Kurisawa, M. Emerging hydrogel designs for controlled protein delivery. Biomater. Sci. 2016, 4, 1184–1192.
- Narayanaswamy, R.; Torchilin, V.P. Hydrogels and Their Applications in Targeted Drug Delivery. Molecules 2019, 24, 603.
- Vasudevan, D.; Sreekumari, S.; Vaidyanathan, K. Proteins: Structure and Function. In Textbook of Biochemistry for Medical Students; Jaypee Brothers Medical Publishers: New Delhi, India, 2017; pp. 36–51.
- Jain, A.; Jain, A.; Gulbake, A.; Shilpi, S.; Hurkat, P.; Jain, S.K. Peptide and protein delivery using new drug delivery systems. Crit. Rev. Ther. Drug Carrier Syst. 2013, 30, 293–329.
- Deb, P.K.; Al-Attraqchi, O.; Chandrasekaran, B.; Paradkar, A.; Tekade, R.K. Protein/Peptide Drug Delivery Systems: Practical Considerations in Pharmaceutical Product Development. In Basic Fundamentals of Drug Delivery; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 651–684.
- Leader, B.; Baca, Q.J.; Golan, D.E. Protein therapeutics: A summary and pharmacological classification. Nat. Rev. Drug Discov. 2008, 7, 21–39.
- Timofeev, V.; Samygina, V. Protein Crystallography: Achievements and Challenges. Crystals 2023, 13, 71.
- Voet, D.; Voet, J.G. Amino acids. In Biochemistry, 4th ed.; John Wiley & Sons: New York, NY, USA, 2010; pp. 67–78.
- Liang, W.; Pan, H.W.; Vllasaliu, D.; Lam, J.K.W. Pulmonary Delivery of Biological Drugs. Pharmaceutics 2020, 12, 1025.
- Awwad, S.; Angkawinitwong, U. Overview of antibody drug delivery. Pharmaceutics 2018, 10, 83.
- Datta-Mannan, A. Mechanisms Influencing the Pharmacokinetics and Disposition of Monoclonal Antibodies and Peptides. Drug Metab. Dispos. 2019, 47, 1100–1110.
- Joseph, M.; Trinh, H.M.; Mitra, A.K. Peptide and Protein-Based Therapeutic Agents. In Emerging Nanotechnologies for Diagnostics, Drug Delivery and Medical Devices; Mitra, A.K., Cholkar, K., Mandal, A., Eds.; Elsevier: Boston, MA, USA, 2017; pp. 145–167.
- Goldberg, M.; Gomez-Orellana, I. Challenges for the oral delivery of macromolecules. Nat. Rev. Drug Discov. 2003, 2, 289–295.
- Vugmeyster, Y.; Xu, X.; Theil, F.P.; Khawli, L.A.; Leach, M.W. Pharmacokinetics and toxicology of therapeutic proteins: Advances and challenges. World J. Biol. Chem. 2012, 3, 73–92.
- Jain, D.; Mahammad, S.S.; Singh, P.P.; Kodipyaka, R. A review on parenteral delivery of peptides and proteins. Drug Dev. Ind. Pharm. 2019, 45, 1403–1420.
- Ibeanu, N.; Egbu, R.; Onyekuru, L.; Javaheri, H.; Khaw, P.T.; Williams, G.R.; Brocchini, S.; Awwad, S. Injectables and Depots to Prolong Drug Action of Proteins and Peptides. Pharmaceutics 2020, 12, 999.
- Usach, I.; Martinez, R.; Festini, T.; Peris, J.E. Subcutaneous Injection of Drugs: Literature Review of Factors Influencing Pain Sensation at the Injection Site. Adv. Ther. 2019, 36, 2986–2996.
- Jackisch, C.; Müller, V.; Maintz, C.; Hell, S.; Ataseven, B. Subcutaneous Administration of Monoclonal Antibodies in Oncology. Geburtshilfe Frauenheilkd 2014, 74, 343–349.
- Tomar, D.S.; Kumar, S.; Singh, S.K.; Goswami, S.; Li, L. Molecular basis of high viscosity in concentrated antibody solutions: Strategies for high concentration drug product development. MAbs 2016, 8, 216–228.
- Devadasu, V.R.; Deb, P.K.; Maheshwari, R.; Sharma, P.; Tekade, R.K. Physicochemical, Pharmaceutical, and Biological Considerations in GIT Absorption of Drugs. In Dosage Form Design Consideration; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2018; pp. 149–178.
- Han, Y.; Gao, Z.; Chen, L.; Kang, L.; Huang, W.; Jin, M.; Wang, Q.; Bae, Y.H. Multifunctional oral delivery systems for enhanced bioavailability of therapeutic peptides/proteins. Acta Pharm. Sin. B 2019, 9, 902–922.
- Abuhelwa, A.Y.; Williams, D.B.; Upton, R.N.; Foster, D.J. Food, gastrointestinal pH, and models of oral drug absorption. Eur. J. Pharm. Biopharm. 2017, 112, 234–248.
- Wright, L.; Barnes, T.J.; Prestidge, C.A. Oral delivery of protein-based therapeutics: Gastroprotective strategies, physiological barriers and in vitro permeability prediction. Int. J. Pharm. 2020, 585, 119488.
- Brown, T.D.; Whitehead, K.A.; Mitragotri, S. Materials for oral delivery of proteins and peptides. Nat. Rev. Mater. 2020, 5, 127–148.
- Linnankoski, J.; Mäkelä, J.; Palmgren, J.; Mauriala, T.; Vedin, C.; Ungell, A.L.; Lazorova, L.; Artursson, P.; Urtti, A.; Yliperttula, M. Paracellular porosity and pore size of the human intestinal epithelium in tissue and cell culture models. J. Pharm. Sci. 2010, 99, 2166–2175.
- Thwala, L.N.; Préat, V.; Csaba, N.S. Emerging delivery platforms for mucosal administration of biopharmaceuticals: A critical update on nasal, pulmonary and oral routes. Expert Opin. Drug Deliv. 2017, 14, 23–36.
- Anselmo, A.C.; Gokarn, Y.; Mitragotri, S. Non-invasive delivery strategies for biologics. Nat. Rev. Drug Discov. 2019, 18, 19–40.
- Balcão, V.; Moutinho, C. Proteins and Peptides: Non-Invasive Delivery. In Encyclopedia of Pharmaceutical Science and Technology; Informa Healthcare: London, UK, 2013; pp. 2555–2578.
- Yoshida, H.; Usui, A.; Abe, Y.; Goda, Y.; Izutsu, K.-I. Relationship Between Geometric and Aerodynamic Particle Size Distributions in the Formulation of Solution and Suspension Metered-Dose Inhalers. AAPS PharmSciTech 2020, 21, 158.
- Patton, J.S.; Brain, J.D.; Davies, L.A.; Fiegel, J.; Gumbleton, M.; Kim, K.J.; Sakagami, M.; Vanbever, R.; Ehrhardt, C. The particle has landed—Characterizing the fate of inhaled pharmaceuticals. J. Aerosol. Med. Pulm. Drug Deliv. 2010, 23, 71–87.
- Matthews, A.A.; Ee, P.L.R.; Ge, R. Developing inhaled protein therapeutics for lung diseases. Mol. Biomed. 2020, 1, 11.
- Jin, L.; Zhou, Q.T.; Chan, H.K.; Larson, I.C.; Pennington, M.W.; Morales, R.A.V.; Boyd, B.J.; Norton, R.S.; Nicolazzo, J.A. Pulmonary Delivery of the Kv1.3-Blocking Peptide HsTX1 for the Treatment of Autoimmune Diseases. J. Pharm. Sci. 2016, 105, 650–656.
- Patton, J.S.; Fishburn, C.S.; Weers, J.G. The lungs as a portal of entry for systemic drug delivery. Proc. Am. Thorac. Soc. 2004, 1, 338–344.
- Meng, T.; Kulkarni, V.; Simmers, R.; Brar, V.; Xu, Q. Therapeutic implications of nanomedicine for ocular drug delivery. Drug Discov. Today 2019, 24, 1524–1538.
- Bachu, R.D.; Chowdhury, P.; Al-Saedi, Z.H.F.; Karla, P.K.; Boddu, S.H.S. Ocular Drug Delivery Barriers-Role of Nanocarriers in the Treatment of Anterior Segment Ocular Diseases. Pharmaceutics 2018, 10, 28.
- Patel, A.; Cholkar, K.; Agrahari, V.; Mitra, A.K. Ocular drug delivery systems: An overview. World J. Pharmacol. 2013, 2, 47–64.
- Sridhar, M.S. Anatomy of cornea and ocular surface. Indian J. Ophthalmol. 2018, 66, 190–194.
- Chaulagain, B.; Jain, A.; Tiwari, A.; Verma, A.; Jain, S.K. Passive delivery of protein drugs through transdermal route. Artif. Cells Nanomed. Biotechnol. 2018, 46, 472–487.
- Katikaneni, S. Transdermal delivery of biopharmaceuticals: Dream or reality? Ther. Deliv. 2015, 6, 1109–1116.
- Chatterjee, S.; Hui, P.C.-l. Stimuli-Responsive Hydrogels: An Interdisciplinary Overview. In Hydrogels; Lăcrămioara, P., Mihaela Violeta, G., Cristina-Elena, D.-P., Eds.; IntechOpen: Rijeka, Croatia, 2018; Chapter 2.
- Raza, F.; Zafar, H.; Zhu, Y.; Ren, Y.; Ullah, A.; Khan, A.U.; He, X.; Han, H.; Aquib, M.; Boakye-Yiadom, K.O.; et al. A Review on Recent Advances in Stabilizing Peptides/Proteins upon Fabrication in Hydrogels from Biodegradable Polymers. Pharmaceutics 2018, 10, 16.
- Mahlumba, P.; Choonara, Y.E.; Kumar, P.; du Toit, L.C.; Pillay, V. Stimuli-Responsive Polymeric Systems for Controlled Protein and Peptide Delivery: Future Implications for Ocular Delivery. Molecules 2016, 21, 1002.
- Chatterjee, S.; Chi-Leung Hui, P. Review of Stimuli-Responsive Polymers in Drug Delivery and Textile Application. Molecules 2019, 24, 2547.
- Jocic, D.; Tourrette, A.; Lavric, P.K. Biopolymer-based Stimuli-Responsive Polymeric Systems for Functional Finishing of Textiles. In Biopolymers; Elnashar, M., Ed.; IntechOpen: Rijeka, Croatia, 2010; Chapter 3.
- Sarwan, T.; Kumar, P.; Choonara, Y.E.; Pillay, V. Hybrid Thermo-Responsive Polymer Systems and Their Biomedical Applications. Front. Mater. 2020, 7, 73.
- Matanović, M.R.; Kristl, J.; Grabnar, P.A. Thermoresponsive polymers: Insights into decisive hydrogel characteristics, mechanisms of gelation, and promising biomedical applications. Int. J. Pharm. 2014, 472, 262–275.
- Marques, A.C.; Costa, P.C.; Velho, S.; Amaral, M.H. Injectable Poloxamer Hydrogels for Local Cancer Therapy. Gels 2023, 9, 593.
- Chatterjee, S.; Hui, P.C. Review of Applications and Future Prospects of Stimuli-Responsive Hydrogel Based on Thermo-Responsive Biopolymers in Drug Delivery Systems. Polymers 2021, 13, 86.
- Altomare, L.; Bonetti, L.; Campiglio, C.E.; De Nardo, L.; Draghi, L.; Tana, F.; Farè, S. Biopolymer-based strategies in the design of smart medical devices and artificial organs. Int. J. Artif. Organs 2018, 41, 337–359.
- Zhang, J.; Jiang, X.; Xiang, W.; Xu, Q.; Zeng, H.; Zhao, Y.; Liu, M.; Wang, Z.; Hu, X.; Wang, Y. Bio-responsive smart polymers and biomedical applications. J. Phys. Mater. 2019, 2, 032004.
- Zha, L.; Banik, B.; Alexis, F. Stimulus responsive nanogels for drug delivery. Soft Matter 2011, 7, 5908–5916.
- Andrade, F.; Roca-Melendres, M.M.; Durán-Lara, E.F.; Rafael, D.; Schwartz, S., Jr. Stimuli-Responsive Hydrogels for Cancer Treatment: The Role of pH, Light, Ionic Strength and Magnetic Field. Cancers 2021, 13, 1164.
- Rizwan, M.; Yahya, R.; Hassan, A.; Yar, M.; Azzahari, A.D.; Selvanathan, V.; Sonsudin, F.; Abouloula, C.N. pH Sensitive Hydrogels in Drug Delivery: Brief History, Properties, Swelling, and Release Mechanism, Material Selection and Applications. Polymers 2017, 9, 137.
- Lynch, C.R.; Kondiah, P.P.D.; Choonara, Y.E.; du Toit, L.C.; Ally, N.; Pillay, V. Hydrogel Biomaterials for Application in Ocular Drug Delivery. Front. Bioeng. Biotechnol. 2020, 8, 228.
- Ferreira, N.N.; Ferreira, L.M.B.; Cardoso, V.M.O.; Boni, F.I.; Souza, A.L.R.; Gremião, M.P.D. Recent advances in smart hydrogels for biomedical applications: From self-assembly to functional approaches. Eur. Polym. J. 2018, 99, 117–133.
- El-Husseiny, H.M.; Mady, E.A.; El-Dakroury, W.A.; Doghish, A.S.; Tanaka, R. Stimuli-responsive hydrogels: Smart state of-the-art platforms for cardiac tissue engineering. Front. Bioeng. Biotechnol. 2023, 11, 1174075.
- Feng, Y.; Taraban, M.; Yu, Y.B. The Effect of Ionic Strength on the Mechanical, Structural and Transport Properties of Peptide Hydrogels. Soft Matter 2012, 8, 11723–11731.
- Sharifzadeh, G.; Hosseinkhani, H. Biomolecule-Responsive Hydrogels in Medicine. Adv. Healthc. Mater. 2017, 6, 1700801.
- Cao, J.; Yuan, P.; Wu, B.; Liu, Y.; Hu, C. Advances in the Research and Application of Smart-Responsive Hydrogels in Disease Treatment. Gels 2023, 9, 662.
- Zhao, L.; Wang, L.; Zhang, Y.; Xiao, S.; Bi, F.; Zhao, J.; Gai, G.; Ding, J. Glucose Oxidase-Based Glucose-Sensitive Drug Delivery for Diabetes Treatment. Polymers 2017, 9, 255.
- Mantha, S.; Pillai, S.; Khayambashi, P.; Upadhyay, A.; Zhang, Y.; Tao, O.; Pham, H.M.; Tran, S.D. Smart Hydrogels in Tissue Engineering and Regenerative Medicine. Materials 2019, 12, 3323.
- Honey Priya, J.; Rijo, J.; Anju, A.; Anoop, K.R. Smart polymers for the controlled delivery of drugs—A concise overview. Acta Pharm. Sin. B 2014, 4, 120–127.
- Lim, S.L.; Ooi, C.-W.; Low, L.E.; Tan, W.S.; Chan, E.-S.; Ho, K.L.; Tey, B.T. Synthesis of poly(acrylamide)-based hydrogel for bio-sensing of hepatitis B core antigen. Mater. Chem. Phys. 2020, 243, 122578.
- Chang, D.; Ma, Y.; Xu, X.; Xie, J.; Ju, S. Stimuli-Responsive Polymeric Nanoplatforms for Cancer Therapy. Front. Bioeng. Biotechnol. 2021, 9, 707319.
- Zhao, Y.; Ran, B.; Xie, X.; Gu, W.; Ye, X.; Liao, J. Developments on the Smart Hydrogel-Based Drug Delivery System for Oral Tumor Therapy. Gels 2022, 8, 741.
- Chandrawati, R. Enzyme-responsive polymer hydrogels for therapeutic delivery. Exp. Biol. Med. 2016, 241, 972–979.
- Municoy, S.; Álvarez Echazú, M.I.; Antezana, P.E.; Galdopórpora, J.M.; Olivetti, C.; Mebert, A.M.; Foglia, M.L.; Tuttolomondo, M.V.; Alvarez, G.S.; Hardy, J.G.; et al. Stimuli-Responsive Materials for Tissue Engineering and Drug Delivery. Int. J. Mol. Sci. 2020, 21, 4724.
- Fu, X.; Hosta-Rigau, L.; Chandrawati, R.; Cui, J. Multi-Stimuli-Responsive Polymer Particles, Films, and Hydrogels for Drug Delivery. Chem 2018, 4, 2084–2107.
- Cheng, R.; Meng, F.; Deng, C.; Klok, H.A.; Zhong, Z. Dual and multi-stimuli responsive polymeric nanoparticles for programmed site-specific drug delivery. Biomaterials 2013, 34, 3647–3657.
- Pham, S.H.; Choi, Y.; Choi, J. Stimuli-Responsive Nanomaterials for Application in Antitumor Therapy and Drug Delivery. Pharmaceutics 2020, 12, 630.
- Lima, D.S.; Tenório-Neto, E.T.; Lima-Tenório, M.K.; Guilherme, M.R.; Scariot, D.B.; Nakamura, C.V.; Muniz, E.C.; Rubira, A.F. pH-responsive alginate-based hydrogels for protein delivery. J. Mol. Liq. 2018, 262, 29–36.
- Xu, H.L.; Xu, J.; Zhang, S.S.; Zhu, Q.Y.; Jin, B.H.; ZhuGe, D.L.; Shen, B.X.; Wu, X.Q.; Xiao, J.; Zhao, Y.Z. Temperature-sensitive heparin-modified poloxamer hydrogel with affinity to KGF facilitate the morphologic and functional recovery of the injured rat uterus. Drug Deliv. 2017, 24, 867–881.
- Dutta, K.; Das, R.; Ling, J.; Monibas, R.M.; Carballo-Jane, E.; Kekec, A.; Feng, D.D.; Lin, S.; Mu, J.; Saklatvala, R.; et al. In Situ Forming Injectable Thermoresponsive Hydrogels for Controlled Delivery of Biomacromolecules. ACS Omega 2020, 5, 17531–17542.
- Hu, D.-N.; Ju, X.-J.; Pu, X.-Q.; Xie, R.; Wang, W.; Liu, Z.; Chu, L.-Y. Injectable Temperature/Glucose Dual-Responsive Hydrogels for Controlled Release of Insulin. Ind. Eng. Chem. Res. 2021, 60, 8147–8158.
- Rahmanian, E.; Salari, N.; Mohammadi, M.; Jalali, R. Evaluation of sexual dysfunction and female sexual dysfunction indicators in women with type 2 diabetes: A systematic review and meta-analysis. Diabetol. Metab. Syndr. 2019, 11, 73.
- Lazzaro, B.P.; Zasloff, M.; Rolff, J. Antimicrobial peptides: Application informed by evolution. Science 2020, 368, eaau5480.
- Mahlapuu, M.; Håkansson, J.; Ringstad, L.; Björn, C. Antimicrobial Peptides: An Emerging Category of Therapeutic Agents. Front. Cell Infect. Microbiol. 2016, 6, 194.
- Rezaei, N.; Hamidabadi, H.G.; Khosravimelal, S.; Zahiri, M.; Ahovan, Z.A.; Bojnordi, M.N.; Eftekhari, B.S.; Hashemi, A.; Ganji, F.; Darabi, S.; et al. Antimicrobial peptides-loaded smart chitosan hydrogel: Release behavior and antibacterial potential against antibiotic resistant clinical isolates. Int. J. Biol. Macromol. 2020, 164, 855–862.