Since the COVID-19 occurrence in late 2019, intense research efforts on an unprecedented scale have focused on the study of SARS-CoV-2 entry mechanisms and clinical presentations.
2. Prevalence of Gastrointestinal Symptoms
Several studies reported gastrointestinal symptoms in patients affected by COVID-19. Their prevalence in adults is high, with diarrhea, nausea, and abdominal pain being the most frequent ones (16.5%, 9.7%, 4.5%, respectively)
[8]. Anorexia or loss of appetite (1.6%), vomiting (1.5%), and loss of taste (1.3%) are less common. Increased liver enzymes are not rare (5.6%) (
Table 1)
[8]. Prevalences, however, are hardly comparable as different series do not report all main gastrointestinal symptoms. This likely results from the different weight attributed by authors to mild and/or infrequent symptoms, which were not invariably reported.
Table 1. Gastrointestinal symptoms in adult and pediatric patients.
In the pediatric population, the incidence of gastrointestinal symptoms is higher compared to adults
[9]. A recent meta-analysis reported a higher prevalence of nausea/vomiting (19.7%) and abdominal pain (20.3%) but not diarrhea (19.08%)
[9]. However, wide variations have been described in different series
[10].
The relationship between gastrointestinal symptoms, mortality, and more severe systemic disease presentation is debatable. Available evidence suggests that the overall presence of gastrointestinal symptoms is not associated with increased mortality rates (OR = 0.88; 95% CI 0.71–1.09;
p = 0.23). The same applies to individual symptoms, such as diarrhea (
p = 0.96), nausea/vomiting (
p = 0.46), and abdominal pain (
p = 0.3)
[11].
A recent meta-analysis correlating the incidence of gastrointestinal symptoms with severe presentation in adults showed that abdominal pain (OR = 2.70, 95% CI 1.17–6.27,
p = 0.02), but not diarrhea, nausea, or vomiting, is associated with aggressive disease
[12].
In the pediatric population, the presence of diarrhea significantly correlates with more severe clinical course (OR 3.9, 95% CI: 1.80–8.73;
p < 0.01). This is not the case for nausea/vomiting and abdominal pain
[9].
The persistence of gastrointestinal symptoms for more than two weeks after discharge is also high, as 3.23% of patients reported nausea, 3.19% vomiting, and 4.12% prolonged diarrhea, while the persistence of abdominal pain was 1.68%
[13].
Gastrointestinal bleeding (GIB) was reported in 2% of COVID-19 patients, respectively, 1% for upper GI and 1% for lower GI
[14]. The most common causes were ulcers (25.3%), erosive/ulcerative diffuse damage (16.1%), and petechial/hemorrhagic gastropathy (9.2%) in upper gastrointestinal bleeding. Ischemic colitis was reported in one-third of patients with lower gastrointestinal bleeding
[15]. Again, some differences have been reported in different cohorts
[4]. The presentation with GIB however represents a negative prognostic factor, as reported by a recent systematic review comparing the outcomes of 808 COVID-19 patients with GIB and 18,179 non-GIB COVID-19 patients. The overall incidence of GIB was 0.06%, with GIB patients showing a higher death rate than non-GIB patients (25.4% vs. 16.4%,
p < 0.001)
[4].
3. Gastrointestinal Infection
Respiratory droplets are the main route of transmission of SARS-CoV-2
[16], but SARS-CoV-2 RNA was also detected in fecal samples
[17][18][19][20][17,18,19,20].
Direct evidence of fecal–oral transmission is still lacking, but emerging evidence supports the hypothesis
[21][22][21,22]. SARS-CoV-2 RNA has indeed been detected in anal swabs and stool samples in over 50% of infected patients
[23][24][25][23,24,25]. RNA levels in the stools ranged from 102 to 105 copies/mL, but in several reports fecal shedding exceeded 107 copies/mL
[23][26][27][28][23,26,27,28]. This is in line with nasopharyngeal fluids concentration (105–1011 copies/mL)
[27][28][27,28]. SARS-CoV-2 concentration in stool samples peaks 2 to 3 weeks after symptom onset
[25][29][25,29], and, as reported in a small German cohort, the RNA load in fecal specimens reflects what is found in sputum in 86% of cases (6 of 7 patients)
[23]. Live SARS-CoV-2 was also observed in the feces of COVID-19 patients, confirming potential fecal–oral transmission
[30]. However, despite being easily detected by electron microscopy
[31], SARS-CoV-2 isolation from stools is difficult
[32].
Recent evidence suggests that viral variants show different gastrointestinal infectivity. Reduced viral replication of Omicron BA.1 and BA.2 variants compared with the B.1.617.2/Delta variant was reported in studies carried out in organoids
[33].
The persistence of the virus in stools is significantly longer (median 22 days, interquartile range 17–31 days) than in respiratory (18 days, 13–29 days;
p = 0.02) and serum samples (16 days, 11–21 days;
p < 0.001)
[25]. Polymerase chain reaction detected viral RNA in fecal samples of patients with no detectable virus in respiratory tract specimens
[19][25][34][19,25,34].
Several studies have shown the presence of SARS-CoV-2 in epithelial cells of both the small and large intestines, as demonstrated by intestinal biopsies
[17][35][36][17,35,36]. Additionally, the transcription of subgenomic SARS-CoV-2 mRNA (sgmRNA) indicates active viral replication in the intestine, as sgmRNA is only transcribed in infected cells and not packaged into virions
[23]. Intestinal organoids primarily secrete SARS-CoV-2 apically
[37], which may explain viral excretion in feces.
Although evidence suggests that the gut is an active site of SARS-CoV-2 replication, it is still unclear whether the virus present in feces is directly infectious. While viral RNA may be shed in fecal specimens, the presence of viral ribonucleic acid does not necessarily imply the presence of live transmissible virus
[38]. Therefore, while direct and indirect data support the hypothesis that SARS-CoV-2 actively infects human intestinal epithelial cells, further research is needed to determine whether the virus in feces is directly infectious.
4. SARS-CoV-2 Structure and Interaction with the Host
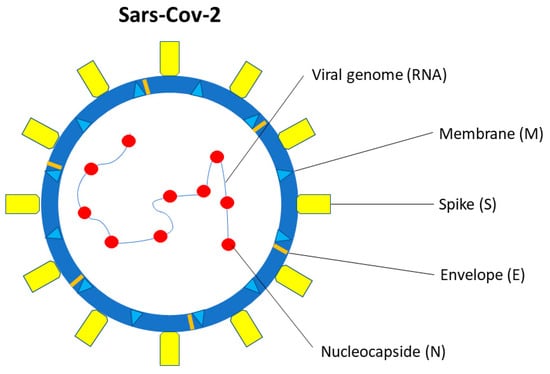
SARS-CoV-2 is a single-stranded β-coronavirus, with 29.9 kb RNA genome and an envelope with spikes on the surface (
Figure 1)
[39]. It shares up to 80% of the gene sequence with other pathogenic members of the coronavirus family, such as SARS-CoV-1 and Middle East Respiratory Syndrome coronavirus (MERS-CoV)
[40].
Figure 1. SARS-CoV-2 structure. SARS-CoV-2 is a single-stranded β-coronavirus. Two-thirds of viral RNA, in the first open reading frame (ORF 1a/b), encodes for 16 non-structural proteins (NSP). The remaining viral genome expresses accessory proteins, interfering with the host innate immune response, and four structural proteins (S, E, N, M).
Two-thirds of viral RNA, in the first open reading frame (ORF 1a/b), translates two polyproteins, encoding for 16 non-structural proteins (NSP). The remaining viral genome expresses accessory proteins, interfering with the host innate immune response, and structural proteins. The four essential structural proteins include the spike (S) glycoprotein, small envelope (E) protein, nucleocapsid (N) protein, and matrix (M) protein
[41]. Proteins M, E, and S form the viral envelope
[42]. The N protein is structurally bound to the viral RNA and is involved in viral replication
[43], while the M protein plays a role in determining the shape of the viral envelope
[43].
Open reading frames encoding nine accessory proteins (3a, 3b, 6, 7a, 7b, 8, 9b, 9c, and 10) and two polyproteins (pp1a and pp1ab) are also present in the genome
[44].
Polyproteins pp1a and pp1ab, but not accessory proteins, are involved in viral replication
[44].
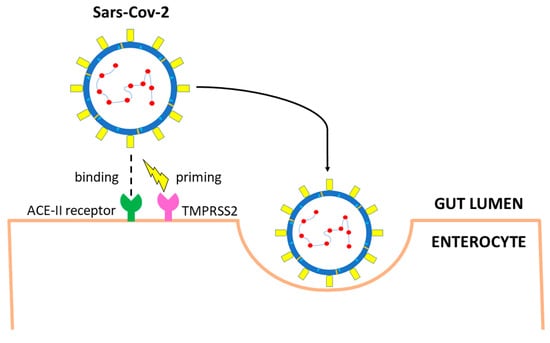
SARS-CoV-2 interacts with target cells through envelope spike glycoprotein which binds the angiotensin-converting enzyme 2 (ACE2) receptor of the host (
Figure 2)
[41]. The binding affinity for the human ACE2 receptor is 10–20 times stronger for SARS-CoV-2 than for its predecessor SARS-CoV-1
[45]. After binding ACE2 receptors, the transmembrane serine protease 2 (TMPRSS2) mediates the cleavage of the spike glycoprotein, regulating the internalization of the virus into target cells
[46]. The two subunits, S1 and S2, favor the binding of the virus to the cell and the fusion between the two cellular membranes
[46].
Figure 2. Main entry route of SARS-CoV-2 in gastrointestinal tract. The spike protein of SARS-CoV-2 binds angiotensin-converting enzyme 2 (ACE2) receptors. Priming by TMPRSS2, TMPRSS4 (or other proteases such as FURIN) leads to endocytosis. The virus is uncoated, genomic RNA is released, and viral proteins are synthesized using the host replication system.
Two proteolytic events are however needed to activate SARS-CoV-2. The first is the cut in the specific cleavage site between the S1 and S2 domains, which is recognized by various proteases, including TMPRSS2
[46] and furin
[47][48][47,48]. The second cleavage site is within the S2 domain and allows the exposition of the fusion peptide, which enables membrane fusion. This second cleavage can be either performed by TMPRSS2 on the surface of the host cell or by lysosomal proteases, such as cathepsin L in the endolysosomes
[49]. Following the entry into the cell, the virus is uncoated and replicates using the host replication system
[42].
5. Route of Gastrointestinal Infection
The exact route of infection is still undefined, but the virus likely reaches the gut after being swallowed.
In vitro studies show that SARS-CoV-2, like other enveloped viruses, loses infectivity after 10 min incubation in gastric fluid
[50]. Nonetheless, this route of transmission is possible as other viruses, such as influenza virus, despite being vulnerable to digestive juices, retain infectivity when protected by highly viscous mucus
[51].
The glycosylation of the S protein is a further mechanism by which other coronaviruses survive the adverse milieu of the stomach and bile-salt-containing duodenal juice
[52]. The mechanism may be shared by SARS-CoV-2.
Indirect evidence deriving from in vitro models of other coronaviruses suggests that fasting or fed state modulate infectivity. Indeed, MERS rapidly loses infectivity in simulated fasting state, low pH gastric fluid, but not after 2 h of exposure to fed-state condition
[53].
It has also been hypothesized that chronic H. pylori infection leading to atrophic gastritis and intestinal metaplasia could facilitate SARS-CoV-2 intestinal infection by reducing stomach acidity
[54][55][54,55]. H. pylori also increases the expression of ACE-2 receptors in the GI tract
[56]. Clinically, a strong correlation between the occurrence of abdominal pain (19.4% vs. 2.6%,
p = 0.007) or diarrhea (32.3% vs. 9.1%,
p = 0.006) and H. pylori infection has been reported in COVID-19 patients
[57].
Similarly, proton pump inhibitor-induced hypochloridria could favor SARS-CoV-2 intestinal infection
[58], but available data are conflicting. Patients on PPI had significantly higher requirement for oxygen therapy, intensive care unit admission, and invasive ventilation than patients not taking PPI (fully adjusted OR (aOR): 2.39; 95% CI: 1.08–5.10) in a post hoc analysis from a nationwide Korean cohort
[5]. Conversely, several meta-analyses did not confirm these early reports
[59][60][59,60].
6. Gastrointestinal Tract–Virus Interaction
Lungs are the primary route of SARS-CoV-2 infection, but ACE2 receptors, an 805 amino acids-, type I cell-surface glycoprotein
[61], are highly expressed also on the brush border of the enterocytes
[62][63][62,63]. The ACE2 receptor is detected by immunofluorescent staining also in the glandular cells of the stomach and colon
[17]. Viral RNA has been detected also in the esophageal mucosa, but the lack of viral nucleocapsid protein staining suggests a low viral load
[17]. This is in keeping with low ACE2 expression in squamous esophageal epithelial cells. ACE2 receptors are minimally expressed by enteroendocrine cells, Paneth cells, and goblet cells
[61][64][65][66][61,64,65,66].
Under physiological conditions, ACE2 receptors in the gastrointestinal tract are associated with the amino acid carrier B0AT1, which regulates the homeostasis of tryptophan, and thus stimulates the production of mechanistic target of rapamycin (mTOR)-dependent antimicrobial peptides from Paneth cells
[67][68][67,68].
Besides ACE2 receptors, other molecules may play a role in SARS-CoV-2 infection. It has been demonstrated that TMPRSS2 is highly expressed in the gastrointestinal tract
[50], not only in enterocytes
[50] but also in intestinal goblet
[69] and Paneth cells (
Figure 2)
[70][71][70,71]. Other serine proteases of the same family, such as TMPRSS4, are also highly expressed in mature enterocytes and potentially favor SARS-CoV-2 infection
[50]. An additive effect of the two enzymes has been documented, suggesting synergic effect resulting from distinct cellular and subcellular localization of the two proteases
[50].
The protease furin, widely present in the stomach, small bowel, and colon
[72], also enables the S protein to separate into two pinching structures
[73]. Although furin significantly increases the cleavage of the S protein, promoting SARS-CoV-2 infectivity and spread, its presence is not essential
[74].
In addition to proteases, other alternative entry molecules, such as neuropilin-1 (NRP1), have been identified
[75]. The expression of NRP1 in the small bowel has been reported on both human biopsies and organoids
[76][77][76,77]. Following protease cleavage of the S protein into S1 and S2, a polybasic Arg-Arg-Ala-Arg carboxyl-terminal sequence on S1 binds NRP1
[75][78][75,78]. The role of NRP1 is less clear than ACE2 receptors, but the protein might mediate SARS-CoV-2 infection in ACE2-negative cells
[77] and possibly explain different disease behavior in adults and children
[76].
Recent studies suggest a possible interaction between the SARS-CoV-2 S protein and the cluster of differentiation (CD) 147 binding site
[79], possibly through cyclophilin A-mediated regulation of ACE2 receptors
[80], but conflicting results have also been published
[81].
A small Italian case series
[82] suggested that VEGF through CD147 may trigger gastrointestinal ischemia in SARS-CoV-2, as reported in other conditions
[83]. However, validation in larger series is needed.
Protease-mediated membrane fusion represents the usual SARS-CoV-2 entry route in the host cell. An alternative option has recently been advocated, consisting of endocytosis resulting from SARS-CoV-2 binding to ACE2 receptors followed by S protein cleavage by cathepsin L
[49] expressed in a variety of tissues including the gastrointestinal tract
[84][85][84,85].