Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Everton Freitas de Morais and Version 2 by Jessie Wu.
Adenoid cystic carcinoma (ACC) is a rare salivary gland tumor that accounts for approximately 1% of all head and neck cancers. Despite its initial indolent behavior, long-term survival is poor due to locoregional recurrence in approximately 40% and distant metastasis in up to 60% of patients who undergo radical treatment. The histological parameters of ACC and the combination of these parameters in histopathological grading systems provide valuable prognostic information about the clinical course of the disease.
- malignant salivary gland tumors
- prognosis
- histopathological features
- histopathological grading systems
1. Histopathological Pattern and Adenoid Cystic CarcinomaC Prognosis
Adenoid cystic carcinoma (ACC) is characterized by a dual cell population consisting of basaloid cells with myoepithelial/basal differentiation and luminal/epithelial cells, which may histologically acquire specific architectural patterns that determine three pathological subtypes [1][2][13,21]. The cribriform pattern is characterized by islands of small or cuboidal basaloid epithelial cells that contain a basophilic nucleus and scarce cytoplasm with multiple pseudocystic spaces filled with basophilic material compatible with glycosaminoglycans (Figure 1A,B). In the tubular pattern, the ductal structures are lined with a single layer of epithelial cells or one or more layers of basaloid cells. An amorphous eosinophilic material may be present in the center of the tubules and the stroma in this pattern is often hyalinized (Figure 1C,D). In the solid pattern, tumor islands are filled with luminal and non-luminal cells dispersed in a dense fibrous connective stroma; areas with ductal or pseudocystic spaces are rare [3][4][5][10,19,22] (Figure 1E,F). Most cases of ACC exhibit more than one pathological pattern [6][7][23,24].
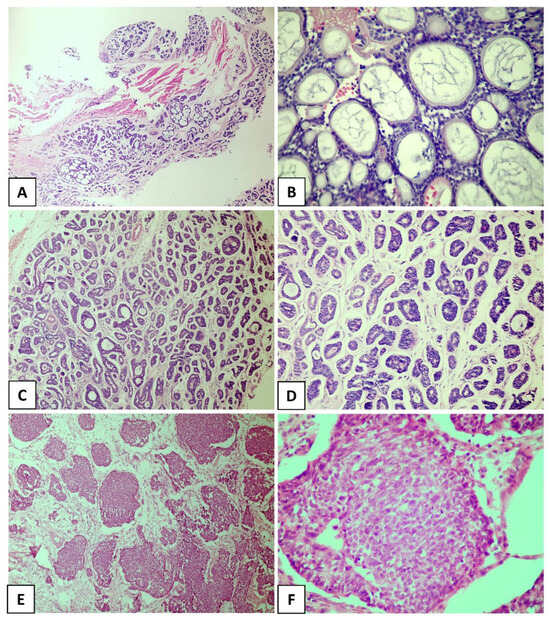
Figure 1. Histological subtypes of the salivary gland adenoid cystic carcinoma. (A,B) Cribriform pattern, (C,D) tubular pattern, and (E,F) solid pattern. ((A) In original magnification of 40×, (C–E) in original magnification of 100×, and (B,F) in original magnification of 200×).
For decades, studies have tried to identify histopathological factors that correlate with the prognosis of ACC [8][9][10][11][12][14,15,16,17,18]. The solid proliferation of tumor cells (predominance of solid areas) was notoriously one of the first proposed prognostic factors and has been considered a useful histological parameter for assessing survival rates in patients with ACC [8][14]. Indeed, the solid subtype is considered the most aggressive variant of ACC, which has a poor prognosis [8][13][14][15][14,25,26,27]. This importance has been confirmed by all histological grading systems for ACC available so far, which are based on the presence and/or proportion of the solid component in the tumor [8][9][10][11][12][14,15,16,17,18]. Furthermore, according to the current WHO classification for salivary gland tumors, ACC in which the solid component accounts for more than one-third of the tumor exhibits a poor clinical course [16][2].
Compared to the cribriform and tubular subtypes, the solid pattern is characterized by high loss of heterozygosity, a larger number of chromosomal and somatic mutations, and high expression of p53 [17][18][19][20][21][28,29,30,31,32]. Clinicopathological studies indicate a higher risk of lymph node metastases in solid ACC [8][14] and a direct association of this pattern with poor overall survival [22][33]. In addition to these results, de Morais et al. [15][27] found that the presence of the solid pattern contributed to the negative impact on long-term disease-specific survival (10 years) of cases evaluated in both univariate and multivariate analyses, corroborating the importance of the solid pattern for the prognostic evaluation of ACC.
Some findings that have been described as markers of poor prognosis (Figure 2A,D) are more common in the solid pattern of ACC compared to the cribriform and tubular subtypes, particularly tumor necrosis and high-grade transformation [4][23][24][25][19,34,35,36]. Xu et al. [4][19] explored the presence of necrosis as a prognostic factor for ACC in a large retrospective cohort of 135 patients and found that its presence is a predictor of poor recurrence-free survival and disease-free survival. In that study, the presence of necrosis was associated with a high mitotic index and severe nuclear atypia [4][19]. High-grade transformation, i.e., the presence of a distinct population of anaplastic cells [24][35], has been histologically defined when the tumor exhibits intense nuclear atypia, a high mitotic index, prominent necrosis, and loss of biphasic ductal-myoepithelial differentiation, features indicative of a poor prognosis [4][23][25][19,34,36]. In a recent study conducted by Zhu et al. [26][37], high-grade transformation was the only histological parameter associated with shortened overall survival and disease-specific survival in multivariate analysis. It is important to highlight that numerous studies have identified particular mutations in solid tumors. Ferrarotto et al. [27][38] detected a high frequency of NOTCH1 mutations among solid ACCs with liver and bone metastasis, as well as a poorer prognosis in these cases. Liu et al. [28][39] reported that loss of PTEN expression was more frequently seen in ACC compared to other salivary gland malignancies, especially in the poorly differentiated, high-grade subtype of solid ACC.
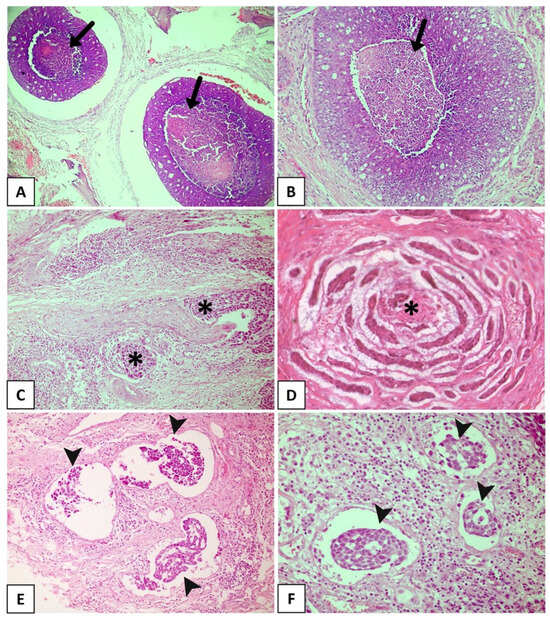
Figure 2. Histopathological features with promising prognostic potential for adenoid cystic carcinoma. (A,B) The black arrow showing extensive areas of necrosis. Solid subtype with perineural invasion in cords (C) and small islands (D) (asterisks). (E,F) Solid tumor with vascular invasion (arrowhead). (Figure (A) in original magnification of 40×, (B,C,E,F) in original magnification of 100×, and (D) in original magnification of 200×).
2. Individual Histological Features and Adenoid Cystic CarcinomaCC Prognosis
Several morphological characteristics were identified as potential prognostic markers for patients with ACC.
PNI, which is nowadays considered a consequence of interactions among tumor cells, neural cells, and the perineural niche [15][27], is found in 48–82% of head and neck ACCs (Figure 2C). It has been widely accepted as the fourth metastatic pathway in ACC, together with the other three well-known routes: direct invasion of surrounding tissues, lymphatic metastasis, and hematogenous metastasis [29][30][31][32][5,46,47,48]. PNI has been widely reported as an independent negative prognostic factor in head and neck ACC and is significantly associated with decreased overall survival, disease-specific survival, locoregional control, and distant metastasis [33][34][35][36][20,44,49,50]. Fang et al. [29][5] reinforced the importance of a careful assessment of PNI in ACC, considering the degree of impairment (invaded layers of the nerve sheath), number of neural invasions, margins of involved nerves (compromised neural circumference), and sites of tumor dissemination (large or small nerves). A meta-analysis conducted by Ju et al. [37][51] indicated that PNI is strongly associated with poor overall and disease-free survival in ACC. Fordice [38][52] showed that survival significantly decreases when a large nerve is involved. Invasion involving the perineurium or endoneurium increases the risk of recurrence when compared to tumors whose growth occurs only adjacent to the nerves [39][53]. In a multicenter cohort of 239 patients with ACC and neural invasion, Amit et al. [40][54] found intraneural invasion to be an independent negative prognostic marker for overall survival and disease-specific survival. Thus, considering these findings, intraneural invasion is more strongly correlated with a poor prognosis than PNI and is a reliable prognostic predictor of ACC. Considering the association between PNI and ACC prognosis, a comprehensive investigation into the underlying mechanisms related to this process is crucial. This exploration is essential to determine potential predictors of this condition and to identify specific markers that can accurately predict tumor prognosis. Such discoveries could facilitate the development of targeted drugs and effectively reduce the risk of ACC recurrence. However, several studies have highlighted the close correlation between distinct PNI characteristics and factors such as ACC metastasis, locoregional recurrence of the tumor, and overall quality of life of patients [41][55].
LVI is another histological finding associated with poor clinical behavior in different malignant neoplasms [34][42][43][44][45][46][47][48][42,43,44,56,57,58,59,60]. In ACC (Figure 2E,F), LVI is reported in a large number of cases, ranging from 5% to 70%, and is a known indicator of high recurrence risk and poor prognosis [49][50][61,62]. Tang et al. [51][63] revealed LVI to be an independent prognostic determinant, whereas Oplatek et al. [44][56] found a significant association with recurrences. In a systematic review and meta-analysis, Martins-Andrade et al. [33][20] found LVI to be a significant prognostic parameter for head and neck ACC, which was associated with lower overall survival rates and a higher risk of lymph node metastases. The prognostic relevance of LVI as a risk factor for recurrence has been documented in the literature [44][51][56,63]. Jeong et al. [48][60] identified the presence of LVI in surgical pathology specimens to be associated with a reduction in 5-year overall survival in recurrent and metastatic ACC, with multivariate analysis confirming its role as an independent risk factor. Although these results indicate an aggressive evolution associated with LVI, most published studies only described its presence or absence and considered LVI to be a secondary finding. Indeed, few studies investigated the true importance of LVI and its impact on survival in ACC as a primary endpoint. Furthermore, the profile of tumor emboli is not well described, with the types of vessels that are being invaded, whether blood or lymphatic, and the morphological characteristics of the invaded vessel being unknown [33][52][9,20]. Therefore, large studies investigating the prognostic potential of LVI in ACC are necessary.
The presence of positive surgical margins has also been proposed as a prognostic factor for ACC [33][20]. Amit et al. [53][64] analyzed the role of surgical margins in 507 cases of head and neck ACC in an international multicenter study and found a high rate of positive surgical margins (50% of the analyzed cases). The authors concluded that positive margins are predictors of poor survival in head and neck ACC, while negative margins, corresponding to tumor-free margins <5 mm, are associated with a favorable outcome. Although de Morais et al. [15][27] found a statistically significant association between positive margins and a poor prognosis at 5 and 10 years in univariate analysis, in multivariate analysis, the status of the surgical margin itself did not have an independent prognostic value. Furthermore, there are no data in the literature that confirm the prognostic role of positive surgical margins in recurrent and metastatic ACC [22][50][33,62]. It is worthwhile noting that the ability to achieve large tumor-free margins depends on a number of factors, including tumor location and size, histopathological pattern, and previous treatment [29][5]. In many cases, surgery is limited by the proximity of vital structures [15][27], as occurs in some cases of head and neck ACC that have an anatomical propensity for intracranial extension involving vital structures, posing a challenge to achieve negative surgical margins [29][5]. Studies have shown that patients with ACC arising at sites close to the base of the skull (nasopharynx, nasal cavity, and paranasal sinuses) have a significantly higher risk of local recurrence [53][54][64,65].
In a recent study, Xuan et al. [55][66] proposed an evaluation based on the dominant cell type. The authors applied immunohistochemistry against p63 and CD117 and classified ACCs into epithelial (E-ACC), myoepithelial (M-ACC), and conventional (C-ACC) subtypes. The results showed that the E-ACC subtype was an independent negative prognostic factor for overall survival and recurrence-free survival. According to the authors, the main advantages of this analysis for ACC prognostic prediction are the reduction in subjectivity associated with traditional histological grading, as well as the practicality and simplicity of the method [55][66].
With respect to prognostic studies, reswearchers must consider the inconsistencies of the results reported in the literature, which may be due to many factors such as differences in patient treatment protocols among cohorts, the duration of postoperative follow-up, and the differences in the proportion of patients in different stages of the disease [55][56][66,67]. However, despite all these drawbacks, the findings highlight the importance of extensive histological evaluation of the primary tumor to identify the elements that imply greater tumor aggressiveness [50][62], without disregarding the fact that the intrinsic characteristics of the primary tumor may also influence the outcome of recurrent and metastatic disease [57][68].