Accelerated biological vascular ageing is still a major driver of the increasing burden of cardiovascular disease and mortality. Exercise training delays this process, known as early vascular ageing, but often lacks effectiveness due to a lack of understanding of molecular and clinical adaptations to specific stimuli.
- exercise
- hypertension
- blood pressure
- cardiovascular disease
- microvascular function
1. Background
32. Chronic Adaptations of Blood Vessels to Exercise
3.1. Long-Term Structural and Functional Vascular Adaptations in Response to Regular Exercise Training
2.1. Long-Term Structural and Functional Vascular Adaptations in Response to Regular Exercise Training
It is well established that regular exercise training improves vascular function in both health and disease. Chronic training-related adaptations of the cardiovascular system improve tissue perfusion and nutrient exchange at rest and result in a greater capacity to increase them during exercise. In this context, both structural and functional adaptations of the blood vessels have been reported (Figure 2).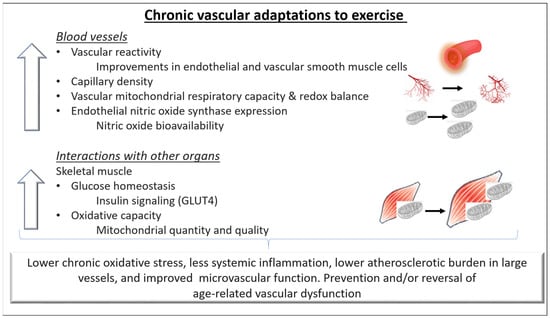
3.2. The Role of Mitochondria in Exercise-Induced Vascular Benefits
2.2. The Role of Mitochondria in Exercise-Induced Vascular Benefits
43. Clinical Vascular Effects of Exercise
4.1. Effects of Exercise on Vascular Health
3.1. Effects of Exercise on Vascular Health
Regular exercise reduces the risk of cardiovascular morbidity and mortality by up to 44% [36][22], delays all-cause mortality [37][23], and increases health span [38][24]. Surprisingly, less than 50% of this effect is explained by reduced oxidative stress and subclinical inflammation due to modifications in cardiovascular risk factors, such as blood pressure, insulin sensitivity, blood lipids, and body composition [39][25]. The remaining gap in explaining vascular benefits of exercise is likely to be filled by direct effects of exercise on the vascular wall that translate into higher nitric oxide availability and favorable structural remodeling [18][26]. The result is a delayed progression of endothelial dysfunction and arterial stiffening with ageing. This assumption is supported by a considerable body of evidence indicating a positive association of cardiorespiratory fitness with endothelial function [40,41][27][28] and a negative association of time spent exercising with arterial stiffness [42][29] as well as with wall thickness [43][30]4.2. Clinical Vascular Effects of Short-Versus Long-Term Exercise
3.2. Clinical Vascular Effects of Short-Versus Long-Term Exercise
The extent and clinical relevance of vascular effects induced by single bouts of exercise and short-term interventions are idiosyncratic in a way. Although endothelial function appears to be modifiable within a few weeks of regular exercise [45][31], arterial stiffness and structural integrity of the vascular wall improve either slowly or not at all [46,47][32][33]. This is not in contrast to the consistent observations about beneficial vascular effects induced by long-term exposure to regular exercise but rather indicates the complexity of the underlying mechanisms.43.2.1. Influence of Age
Cardiovascular effects of chronic regular exercise are independent of sex and age [4,40][4][27] and are already apparent in minors and young adults [48][34], as demonstrated by the European Youth Heart Study [49][35] and the KiGGS study [50][36]. Considering the increasing prevalence of obesity and inactivity among children and adolescents [51][37], preventive efforts involving regular exercise should include the youngest individuals within a population.43.2.2. Influence of Cardiovascular Risk Factors and Diseases
Similar observations regarding clinical vascular effects of exercise have been made for both healthy individuals and patients with comorbidities, such as metabolic syndrome [40][27], arterial hypertension [53][38], and heart failure [40,54][27][39]. In contrast, exercise studies in animals provided evidence indicating an impaired mechanical transduction of elevated shear stress [55][40] and an attenuated increase in nitric oxide release [56][41] in the presence of cardiovascular risk factors such as arterial hypertension.43.2.3. Influence of Training Status and Physical Fitness Level
It is an appealing thought that cardiorespiratory fitness or previous training level influence the vascular adaptability to an exercise stimulus. It seems only logical that a highly trained organism does not have much room for further optimizations. Studies about endothelial adaptations to exercise in highly trained athletes support this in part, as some of them report better endothelial function than in untrained individuals [60,61[42][43][44],62], whereas many others report no differences or even lower function [63,64,65][45][46][47].54. Exercise Training to Improve Vascular Fitness
5.1. General Aspects of Exercise Training to Improve Vascular Health
4.1. General Aspects of Exercise Training to Improve Vascular Health
The World Health Organization recommends at least 75 min per week of vigorous physical activity or 150 min of moderate intensity [68][48]. The relationship between exercise and cardiovascular risk has been described in a curvilinear dose–response pattern [69][49], and numerous studies have consistently reported beneficial vascular effects of exercise training [5,42,43,44,59,70][5][29][30][50][51][52]. However, these effects depend on frequency, intensity, volume, and modality of the training, and are subject to considerable individual variation [71][53]. The F(requency)-I(ntensity)-T(ime)-T(ype) principle provides a practical approach to structure and adapt the training program according to the individual’s vascular responses.5.2. F-I-T-T Principle: F(requency)
4.2. F-I-T-T Principle: F(requency)
Longitudinal shear stress is a major stimulus for adaptive endothelial responses to exercise. Therefore, the total load of shear stimulus rather than the peak itself seems to be the critical determinant [72][54]. An animal study demonstrated that high frequencies of repeatedly elevated shear stress induce adaptive mechanisms within the endothelial cells [73][55]. Repeated elevations in shear stress could therefore explain some of the direct vascular effects of exercise. Aerobic exercise training: A meta-analysis of randomized controlled exercise interventions in humans found no association between the frequency of sessions and improvement of endothelial function with aerobic exercise training [71][53]. Frequently repeated shorter bouts of exercise training might still be a considerable option, especially in individuals in whom the risk of injuries limits the application of high intensities or loads. Resistance exercise training: A positive association between the frequency of resistance training sessions and improvement of endothelial function has been shown [71][53]. As with aerobic exercise training, frequently repeated shorter bouts of exercise training might be a considerable option in resistance training as well to minimize injury risk. However, the optimal frequency of training stimuli is still unclear in both aerobic and resistance exercise training.5.3. F-I-T-T Principle: I(ntensity)
4.3. F-I-T-T Principle: I(ntensity)
Aerobic exercise training: One study conducted a 12-week aerobic, ergometer-based training intervention at mild, moderate, and high exercise intensity [74][56]. Interestingly, only moderate but not high intensity led to improvements of nitric oxide-dependent endothelial function and less oxidative stress. The authors concluded that high intensities of aerobic exercise might induce massive acute oxidative and inflammatory stress, potentially attenuating favorable effects of elevated shear stress. Consistently, the short-term decrease in vascular function immediately after an exercise bout becomes larger with increasing exercise intensities [75][57].
Resistance exercise training: For resistance training, little evidence exists about the relationship between intensity and vascular adaptations, and it does not suggest a dose–response relationship between resistance exercise intensity and improvements in vascular function [71][53].5.4. F-I-T-T Principle: T(ime)
4.4. F-I-T-T Principle: T(ime)
Aerobic exercise training: The relationship of aerobic exercise with functional and structural vascular adaptations has been described in a dose–response pattern, with higher volumes of at least moderate-intensity exercise inducing higher functional vascular improvements [81][58]. However, the nature of this relationship is unclear, and no data exist about a minimum necessary time of training or a ceiling effect. To date, no conclusion can be drawn on the appropriate duration of a single session and, therefore, the appropriate volume of elevated shear stress that would provide the optimal stimulus for endothelial adaptation. Resistance training: Very limited data exist on the relationship of resistance exercise duration with functional and structural vascular adaptations. Therefore, no conclusions can be drawn to date.5.5. F-I-T-T Principle: T(ype)
4.5. F-I-T-T Principle: T(ype)
Continuous versus interval aerobic exercise training: High-intensity interval training (HIIT) is a frequently used method of improving fitness. A meta-analysis examining the effects of HIIT relative to moderate-intensity continuous training (MICT) on vascular function reported that HIIT was more effective at improving macrovascular (brachial artery) function than MICT. However, the authors reported that the variability in secondary outcome measures and the small sample sizes in the studies included limits this finding. Aerobic, resistance (dynamic/isometric), and combined exercise training: Both aerobic and resistance exercise seem to be associated with idiosyncratic patterns of blood flow and shear stress, which lead to distinct effects on arterial function and remodeling [20][59]. Isometric exercise training has also been suggested as an effective intervention for inducing favorable vascular adaptations.5.6. Individualization
4.6. Individualization
Despite considerable scientific efforts, the mechanisms by which protective effects of exercise contribute to the maintenance and improvement of vascular health are still not fully understood. In consequence, evidence is lacking when it comes to the choice of optimal training programs for the individual [20,92][59][60]. Furthermore, patients’ adherence to exercise-based therapies is often undermined by the high efforts regular exercise requires [93,94][61][62]. Individuals with the poorest functional capacity who carry the highest risk of early frailty and disability, especially, do not seem reachable in many multifactorial risk-based studies [95][63]. Furthermore, sex differences in the training adaptations of the vessels have been reported [98,99][64][65]. Specifically, although in healthy, exercise-trained adults, large-elastic-artery-stiffening progression was attenuated, and exercise interventions were shown to improve arterial stiffness in sedentary middle-aged and older men and postmenopausal women; regular aerobic exercise was reported to improve endothelial function in men (by reducing oxidative stress and preserving NO bioavailability) but not to do so consistently in estrogen-deficient postmenopausal women. Thus, potential sex differences should also be taken into account when designing an exercise program.References
- Widlansky, M.E.; Gokce, N.; Keaney, J.F.; Vita, J.A., Jr. The clinical implications of endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1149–1160.
- Danninger, K.; Hafez, A.; Binder, R.K.; Aichberger, M.; Hametner, B.; Wassertheurer, S.; Weber, T. High prevalence of hypertension and early vascular aging: A screening program in pharmacies in Upper Austria. J. Hum. Hypertens. 2020, 34, 326–334.
- Nilsson, P.M.; Boutouyrie, P.; Cunha, P.; Kotsis, V.; Narkiewicz, K.; Parati, G.; Rietzschel, E.; Scuteri, A.; Laurent, S. Early vascular ageing in translation: From laboratory investigations to clinical applications in cardiovascular prevention. J. Hypertens. 2013, 31, 1517–1526.
- Vaitkevicius, P.V.; Fleg, J.L.; Engel, J.H.; O’Connor, F.C.; Wright, J.G.; Lakatta, L.E.; Yin, F.C.; Lakatta, E.G. Effects of age and aerobic capacity on arterial stiffness in healthy adults. Circulation 1993, 88, 1456–1462.
- Konigstein, K.; Wagner, J.; Infanger, D.; Knaier, R.; Nève, G.; Klenk, C.; Carrard, J.; Hinrichs, T.; Schmidt-Trucksäss, A. Cardiorespiratory Fitness and Endothelial Function in Aging Healthy Subjects and Patients With Cardiovascular Disease. Front. Cardiovasc. Med. 2022, 9, 870847.
- Pinto, R.; Melo, X.; Angarten, V.; Pires, M.L.; Borges, M.; Santos, V.; Abreu, A.; Santa-Clara, H. The effects of 12-months supervised periodized training on health-related physical fitness in coronary artery disease: A randomized controlled trial. J. Sports Sci. 2021, 39, 1893–1902.
- Königstein, K.; Meier, J.; Angst, T.; Maurer, D.J.; Kröpfl, J.M.; Carrard, J.; Infanger, D.; Baumann, S.; Bischofsberger, I.; Harder, M.; et al. VascuFit: Vascular Effects of Non-linear Periodized Exercise Training in Sedentary Adults with Elevated Cardiovascular Risk—Protocol for a Randomized Controlled Trial. BMC Cardiovasc. Disord. 2022, 27, 449.
- Kojda, G.; Hambrecht, R. Molecular mechanisms of vascular adaptations to exercise. Physical activity as an effective antioxidant therapy? Cardiovasc. Res. 2005, 67, 187–197.
- Harrison, D.G.; Cai, H. Endothelial control of vasomotion and nitric oxide production. Cardiol. Clin. 2003, 21, 289–302.
- Vasiliadis, A.V.; Zafeiridis, A.; Dipla, K.; Galanis, N.; Chatzidimitriou, D.; Kyparos, A.; Nikolaidis, M.G.; Vrabas, I.S. Circulating angiogenic biomolecules at rest and in response to upper-limb exercise in individuals with spinal cord injury. J. Spinal Cord. Med. 2014, 37, 226–232.
- Pugh, C.W.; Ratcliffe, P.J. Regulation of angiogenesis by hypoxia: Role of the HIF system. Nat. Med. 2003, 9, 677–684.
- Tomanek, R.J.; Schatteman, G.C. Angiogenesis: New insights and therapeutic potential. Anat. Rec. 2000, 261, 126–135.
- Brodal, P.; Ingjer, F.; Hermansen, L. Capillary supply of skeletal muscle fibers in untrained and endurance-trained men. Am. J. Physiol. 1977, 232, H705–H712.
- Gute, D.; Laughlin, M.H.; Amann, J.F. Regional changes in capillary supply in skeletal muscle of interval-sprint and low-intensity, endurance-trained rats. Microcirculation 1994, 1, 183–193.
- Taylor, J.L.; Keating, S.E.; Holland, D.J.; Green, D.J.; Coombes, J.S.; Bailey, T.G. Comparison of high intensity interval training with standard cardiac rehabilitation on vascular function. Scand. J. Med. Sci. Sports 2022, 32, 512–520.
- Thomas, H.J.; Marsh, C.E.; Naylor, L.H.; Ainslie, P.N.; Smith, K.J.; Carter, H.H.; Green, D.J. Resistance, but not endurance exercise training, induces changes in cerebrovascular function in healthy young subjects. Am. J. Physiol. Heart Circ. Physiol. 2021, 321, H881–H892.
- Hood, D.A.; Uguccioni, G.; Vainshtein, A.; D’Souza, D. Mechanisms of exercise-induced mitochondrial biogenesis in skeletal muscle: Implications for health and disease. Compr. Physiol. 2011, 1, 1119–1134.
- Zhang, Y.; Oliveira, A.N.; Hood, D.A. The intersection of exercise and aging on mitochondrial protein quality control. Exp. Gerontol. 2020, 131, 110824.
- Guan, Y.; Drake, J.C.; Yan, Z. Exercise-Induced Mitophagy in Skeletal Muscle and Heart. Exerc. Sport. Sci. Rev. 2019, 47, 151–156.
- Lundby, C.; Jacobs, R.A. Adaptations of skeletal muscle mitochondria to exercise training. Exp. Physiol. 2016, 101, 17–22.
- Bravo-San Pedro, J.M.; Kroemer, G.; Galluzzi, L. Autophagy and Mitophagy in Cardiovascular Disease. Circ. Res. 2017, 120, 1812–1824.
- Lee, D.C.; Sui, X.; Artero, E.G.; Lee, I.-M.; Church, T.S.; McAuley, P.A.; Stanford, F.C.; Kohl, H.W.; Blair, S.N. Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: The Aerobics Center Longitudinal Study. Circulation 2011, 124, 2483–2490.
- Paffenbarger, R.S.; Kampert, J.B., Jr.; Lee, I.M.; Hyde, R.T.; Leung, R.W.; Wing, A.L. Changes in physical activity and other lifeway patterns influencing longevity. Med. Sci. Sports Exerc. 1994, 26, 857–865.
- Wagner, J.; Knaier, R.; Konigstein, K.; Klenk, C.; Carrard, J.; Lichtenstein, E.; Scharnagl, H.; März, W.; Hanssen, H.; Hinrichs, T.; et al. Composite Measures of Physical Fitness to Discriminate Between Healthy Aging and Heart Failure: The COmPLETE Study. Front. Physiol. 2020, 11, 596240.
- Green, D.J.; O’Driscoll, G.; Joyner, M.J.; Cable, N.T. Exercise and cardiovascular risk reduction: Time to update the rationale for exercise? J. Appl. Physiol. (1985) 2008, 105, 766–768.
- Miyachi, M.; Tanaka, H.; Yamamoto, K.; Yoshioka, A.; Takahashi, K.; Onodera, S. Effects of one-legged endurance training on fem oral arterial and venous size in healthy humans. J. Appl. Physiol. 2001, 90, 2439–2444.
- Montero, D. The association of cardiorespiratory fitness with endothelial or smooth muscle vasodilator function. Eur. J. Prev. Cardiol. 2015, 22, 1200–1211.
- Braun, G.; Hafner, B.; Konigstein, K.; Infanger, D.; Klenk, C.; Rossmeissl, A.; Schmidt-Trucksäss, A.; Hanssen, H. Association of cardiorespiratory fitness with retinal vessel diameters as a biomarker of cardiovascular risk. Microvasc. Res. 2018, 120, 36–40.
- Germano-Soares, A.H.; Andrade-Lima, A.; Meneses, A.L.; Correia, M.A.; Parmenter, B.J.; Tassitano, R.M.; Cucato, G.G.; Ritti-Dias, R.M. Association of time spent in physical activities and sedentary behaviors with carotid-femoral pulse wave velocity: A systematic review and meta-analysis. Atheroscler 2018, 269, 211–218.
- Garcia-Hermoso, A.; Gonzalez-Ruiz, K.; Triana-Reina, H.R.; Olloquequi, J.; Ramirez-Velez, R. Effects of Exercise on Carotid Arterial Wall Thickness in Obese Pediatric Populations: A Meta-Analysis of Randomized Controlled Trials. Child. Obes. 2017, 13, 138–145.
- Dawson, E.A.; Cable, N.T.; Green, D.J.; Thijssen, D.H.J. Do acute effects of exercise on vascular function predict adaptation to training? Eur. J. Appl. Physiol. 2018, 118, 523–530.
- Oudegeest-Sander, M.H.; Olde Rikkert, M.G.; Smits, P.; Thijssen, D.H.; van Dijk, A.P.; Levine, B.D.; Hopman, M.T. The effect of an advanced glycation end-product crosslink breaker and exercise training on vascular function in older individuals: A randomized factorial design trial. Exp. Gerontol. 2013, 48, 1509–1517.
- Rauramaa, R.; Halonen, P.; Vaisanen, S.B.; Lakka, T.A.; Schmidt-Trucksäss, A.; Berg, A.; Penttilä, I.M.; Rankinen, T.; Bouchard, C. Effects of aerobic physical exercise on inflammation and atherosclerosis in men: The DNASCO Study: A six-year randomized, controlled trial. Ann. Intern. Med. 2004, 140, 1007–1014.
- Cayres, S.U.; Agostinete, R.R.; de Moura Mello Antunes, B.; Lira, F.S.; Fernandes, R.A. Impact of physical exercise/activity on vascular structure and inflammation in pediatric populations: A literature review. J. Spec. Pediatr. Nurs. 2016, 21, 99–108.
- Ried-Larsen, M.; Grontved, A.; Kristensen, P.L.; Froberg, K.; Andersen, L.B. Moderate-and-vigorous physical activity from adolescence to adulthood and subclinical atherosclerosis in adulthood: Prospective observations from the European Youth Heart Study. Br. J. Sports Med. 2015, 49, 107–112.
- Konigstein, K.; Buschges, J.C.; Sarganas, G.; Krug, S.; Neuhauser, H.; Schmidt-Trucksass, A. Exercise and Carotid Properties in the Young-The KiGGS-2 Study. Front. Cardiovasc. Med. 2021, 8, 767025.
- Spinelli, A.; Buoncristiano, M.; Nardone, P.; Starc, G.; Hejgaard, T.; Júlíusson, P.B.; Fismen, A.; Weghuber, D.; Milanović, S.M.; García-Solano, M.; et al. Thinness, overweight, and obesity in 6- to 9-year-old children from 36 countries: The World Health Organization European Childhood Obesity Surveillance Initiative-COSI 2015–2017. Obes. Rev. 2021, 22 (Suppl. S6), e13214.
- Collier, S.R.; Kanaley, J.A.; Carhart, R., Jr.; Frechette, V.; Tobin, M.M.; Hall, A.K.; Luckenbaugh, A.N.; Fernhall, B. Effect of 4 weeks of aerobic or resistance exercise training on arterial stiffness, blood flow and blood pressure in pre- and stage-1 hypertensives. J. Hum. Hypertens. 2008, 22, 678–686.
- Pearson, M.J.; Smart, N.A. Effect of exercise training on endothelial function in heart failure patients: A systematic review meta-analysis. Int. J. Cardiol. 2017, 231, 234–243.
- Zhang, X.; Cheng, R.; Rowe, D.; Sethu, P.; Daugherty, A.; Yu, G.; Shin, H.Y. Shear-sensitive regulation of neutrophil flow behavior and its potential impact on microvascular blood flow dysregulation in hypercholesterolemia. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 587–593.
- Sun, D.; Huang, A.; Yan, E.H.; Wu, Z.; Yan, C.; Kaminski, P.M.; Oury, T.D.; Wolin, M.S.; Kaley, G.; Csiszar, A.; et al. Reduced release of nitric oxide to shear stress in mesenteric arteries of aged rats. Am. J. Physiol. Heart Circ. Physiol. 2004, 286, H2249–H2256.
- Kasikcioglu, E.; Oflaz, H.; Kasikcioglu, H.A.; Kayserilioglu, A.; Umman, S.; Meric, M. Endothelial flow-mediated dilatation and exercise capacity in highly trained endurance athletes. Tohoku J. Exp. Med. 2005, 205, 45–51.
- Tanriverdi, H.; Evrengul, H.; Tanriverdi, S.; Turgut, S.; Akdag, B.; Kaftan, H.A.; Semiz, E. Improved endothelium dependent vasodilation in endurance athletes and its relation with ACE I/D polymorphism. Circ. J. 2005, 69, 1105–1110.
- Walther, G.; Nottin, S.; Karpoff, L.; Perez-Martin, A.; Dauzat, M.; Obert, P. Flow-mediated dilation and exercise-induced hyperaemia in highly trained athletes: Comparison of the upper and lower limb vasculature. Acta Physiol. 2008, 193, 139–150.
- Rognmo, O.; Bjornstad, T.H.; Kahrs, C.; Tjønna, A.E.; Bye, A.; Haram, P.M.; Stølen, T.; Slørdahl, S.A.; Wisløff, U. Endothelial function in highly endurance-trained men: Effects of acute exercise. J. Strength. Cond. Res. 2008, 22, 535–542.
- Petersen, S.E.; Wiesmann, F.; Hudsmith, L.E.; Robson, M.D.; Francis, J.M.; Selvanayagam, J.B.; Neubauer, S.; Channon, K.M. Functional and structural vascular remodeling in elite rowers assessed by cardiovascular magnetic resonance. J. Am. Coll. Cardiol. 2006, 48, 790–797.
- Green, D.J.; Rowley, N.; Spence, A.; Carter, H.; Whyte, G.; George, K.; Naylor, L.H.; Cable, N.T.; Dawson, E.A.; Thijssen, D.H. Why isn’t flow-mediated dilation enhanced in athletes? Med. Sci. Sports Exerc. 2013, 45, 75–82.
- WHO. WHO Global Recommendations on Physical Activity for Health. 2010. WHO Guidelines Approved by the Guidelines Review Committee; WHO: Geneva, Switzerland, 2010.
- Williams, P.T.; Thompson, P.D. Walking versus running for hypertension, cholesterol, and diabetes mellitus risk reduction. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1085–1091.
- Campbell, A.; Grace, F.; Ritchie, L.; Beaumont, A.; Sculthorpe, N. Long-Term Aerobic Exercise Improves Vascular Function into Old Age: A Systematic Review, Meta-Analysis and Meta Regression of Observational and Interventional Studies. Front. Physiol. 2019, 10, 31.
- Montero, D.; Roberts, C.K.; Vinet, A. Effect of aerobic exercise training on arterial stiffness in obese populations: A systematic review and meta-analysis. Sports Med. 2014, 44, 833–843.
- Konigstein, K.; Infanger, D.; Klenk, C.; Carrard, J.; Hinrichs, T.; Schmidt-Trucksass, A. Physical activity is favorably associated with arterial stiffness in patients with obesity and elevated metabolic risk. Int. J. Clin. Pract. 2020, 74, e13563.
- Ashor, A.W.; Lara, J.; Siervo, M.; Celis-Morales, C.; Oggioni, C.; Jakovljevic, D.G.; Mathers, J.C. Exercise modalities and endothelial function: A systematic review and dose-response meta-analysis of randomized controlled trials. Sports Med. 2015, 45, 279–296.
- Pyke, K.E.; Tschakovsky, M.E. Peak vs. total reactive hyperemia: Which determines the magnitude of flow-mediated dilation? J. Appl. Physiol. (1985) 2007, 102, 1510–1519.
- Zhang, J.; Friedman, M.H. Adaptive response of vascular endothelial cells to an acute increase in shear stress frequency. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H894–H902.
- Goto, C.; Higashi, Y.; Kimura, M.; Noma, K.; Hara, K.; Nakagawa, K.; Kawamura, M.; Chayama, K.; Yoshizumi, M.; Nara, I. Effect of different intensities of exercise on endothelium-dependent vasodilation in humans: Role of endothelium-dependent nitric oxide and oxidative stress. Circulation 2003, 108, 530–535.
- Dawson, E.A.; Green, D.J.; Cable, N.T.; Thijssen, D.H. Effects of acute exercise on flow-mediated dilatation in healthy humans. J. Appl. Physiol. (1985) 2013, 115, 1589–1598.
- Early, K.S.; Stewart, A.; Johannsen, N.; Lavie, C.J.; Thomas, J.R.; Welsch, M. The Effects of Exercise Training on Brachial Artery Flow-Mediated Dilation: A Meta-analysis. J. Cardiopulm. Rehabil. Prev. 2017, 37, 77–89.
- Rowley, N.J.; Dawson, E.A.; Birk, G.K.; Cable, N.T.; George, K.; Whyte, G.; Thijssen, D.H.; Green, D.J. Exercise and arterial adaptation in humans: Uncoupling localized and systemic effects. J. Appl. Physiol. 2011, 110, 1190–1195.
- Kozakova, M.; Palombo, C. Vascular Ageing and Aerobic Exercise. Int. J. Environ. Res. Public Health 2021, 18, 10666.
- Conraads, V.M.; Deaton, C.; Piotrowicz, E.; Santaularia, N.; Tierney, S.; Piepoli, M.F.; Pieske, B.; Schmid, J.-P.; Dickstein, K.; Ponikowski, P.; et al. Adherence of heart failure patients to exercise: Barriers and possible solutions: A position statement of the Study Group on Exercise Training in Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2012, 14, 451–458.
- Sallis, R.; Franklin, B.; Joy, L.; Ross, R.; Sabgir, D.; Stone, J. Strategies for promoting physical activity in clinical practice. Prog. Cardiovasc. Dis. 2015, 57, 375–386.
- Sjosten, N.M.; Salonoja, M.; Piirtola, M.; Vahlberg, T.J.; Isoaho, R.; Hyttinen, H.K.; Aarnio, P.T.; Kivelä, S.-L. A multifactorial fall prevention programme in the community-dwelling aged: Predictors of adherence. Eur. J. Public Health 2007, 17, 464–470.
- Santos-Parker, J.R.; Strahler, T.R.; Vorwald, V.M.; Pierce, G.L.; Seals, D.R. Habitual aerobic exercise does not protect against micro- or macrovascular endothelial dysfunction in healthy estrogen-deficient postmenopausal women. J. Appl. Physiol. 2017, 122, 11–19.
- Seals, D.R.; Nagy, E.E.; Moreau, K.L. Aerobic exercise training and vascular function with ageing in healthy men and women. J. Physiol. 2019, 597, 4901–4914.