Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Xianyi Sha and Version 4 by Fanny Huang.
Airway mucus is a complex viscoelastic gel mainly composed of water, glycoproteins, lipids, enzymes, minerals, etc. Among them, glycoprotein is the main factor determining mucus-gel-like rheology. Airway mucus forms a protective barrier by secreting mucin, which represents the absorption barrier, especially for more lipophilic drugs. It rapidly clears the drug from the airways through physiological mucus clearance mechanisms, so the drug does not remain in the lungs or reach the airway epithelial tissue for a long time.
- airway mucus
- nanoparticles
1. Introduction
The mucus layer plays a vital role in human health, as it is the front line of the body's defense system [1], capable of selectively penetrating foreign bodies and pathogens, thereby protecting the normal functioning of the organism [2]. Lung mucus consists of two layers: the fluid layer on the airway surface and the layer around the eyelashes. The former consists of gel-forming mucus and is responsible for adsorbing and encapsulating inhalation particles. The latter is where surface cells beat and relax, efficiently transporting the mucus layer to the outside of the lungs [3][4][3,4]. The composition and thickness of the mucus layer is not constant; It is a dynamic system whose composition and thickness are caused by the continuous secretion and clearance of mucus [5].
In addition to water, the main component of mucus is mucin, which can be divided into two subtypes according to its glycosylation variability: secreted mucin and membrane-bound mucin. Membrane-binding proteins bind mainly to the surface of the mucosal epithelium, while the disulfide bonds between them link the secreted mucins to form a continuous gel state [6][6]. Given the importance of lung mucus to the bioavailability of pulmonary drugs, studying the important components and tissues of lung mucus [5] is critical to understanding its barrier function. Drugs delivered directly to the airways or inhalation therapy [7][7] are commonly used to treat lung disease. Among them, inhalation therapy makes it easier to deliver therapeutic drugs to the pulmonary mucosa, so it is possible to significantly reduce the dose of the drug and further reduce its side effects. However, due to the inherent clearance mechanism of the pulmonary mucosa, the drug is less bioavailable in the lungs, and most of the drug is cleared in the pulmonary mucosa [8][9][8,9].
Over the past few decades, convincing data have confirmed that nanodelivery systems can be promising carriers for delivering drugs through the mucus layer, including polymer nanoparticles, liposomes, polymer micelles, and nanoparticles [10][11][12][13][14][15][10,11,12,13,14,15]. After inhalation delivery to the airway, these nanoparticles can penetrate or remain in the airway mucus layer by osmosis-mediated, adhesion-mediated, and biomimetic-mediated, respectively [16][17][18][16,17,18]. The benefits of utilizing nanocarriers are increased bioavailability of the drug and reduced unwanted toxicity due to its surface modification, suitable nanometer size, and blood stability [19][20][19,20].
2. Pathophysiology of Aairway Mmucus
According to statistics, a typical adult breaths about 16-20 times per minute in a calm state. The amount of gas inhaled or exhaled is approximately 500 mL, or tidal volume [21]. As a result, the surface of the human airways constantly interacts with the external environment, including inhaled particles and pathogens. The mucociliary clearance mechanism is an important defense mechanism for maintaining a normal physiological state of the human airway [22]. The mucocilia removal system avoids the retention of pathogenic bacteria by constantly renewing the mucus blanket while removing pathogenic microorganisms and inhaled particles. The mucosal cilia clearance system [23] has three main components: the surface fluid layer in contact with the airway lumen, the periciliary fluid layer that supports cilia beating, and the respiratory epithelium composed of secretory cells [24] [24] (Figure 1).
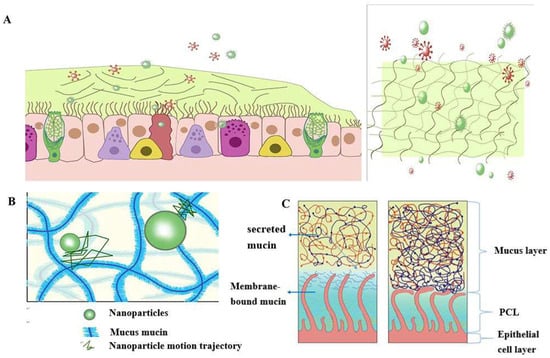
Figure 1Schematic diagram of the structure and function of the mucus barrier: (A) The mucosal cilia removal system has three main components: the surface fluid layer in contact with the airway lumen, the periciliary fluid layer that supports cilia beating, and the respiratory epithelium composed of secretory cells. Constant renewal of the mucus blanket avoids the retention of pathogenic bacteria, while removing pathogenic microorganisms (red spheres) and inhaled particulate matter (green spheres); (B) Schematic diagram of the nanoparticle structure through the mucin network. Small molecules can cross the mucus barrier by diffusion freely, but most large molecules do not easily cross the mucus barrier; (C) Schematic diagram of PCL collapse under normal conditions due to mucus and PCL layers and airway dehydration.
The mucus layer is one of the key components of the mucocilia removal system, which acts as both a physical and a chemical barrier. The mucus layer consists of hundreds of substances and contains 98% water and 2% solids [25]. The main macromolecule of this 2% solid substance is mucin, a macromolecule formed from a family of glycoproteins that are highly glycosylated [26][27][28][26,27,28]. The main secreted mucins in the airways are MUC5B and MUC5AC [29][30][29,30], which have characteristic domains formed by repeated tandem associations of abundant proline, serine, serine, and threonine. The repeat sequence undergoes O-glycosylation to harden the mucin backbone and increase the stiffness of the mucin chain, thus maintaining the gel morphology of the mucus. Mucin itself can bind to therapeutic drugs in a non-specific way. Pavan G. Bhat and colleagues studied the permeability of porcine gastric mucus to five substances: isoniazid [31], pentamidine [32], rifampicin [33], p-aminosalicylic acid [34], and pyrazinamide [35], all of which can be delivered to lung targets using inhalation therapy. The permeability of all two agents was significantly reduced in the presence of mucus compared with the permeability of the blank buffer [2]. The above results show that all compounds bind specifically to mucin molecules before passing through the mucus layer, resulting in reduced penetration through the mucus layer. The pore size of the mucus layer also plays a crucial role in the penetration of the drug. Anionic and nonionic surfactants have a more significant effect on the mucus permeability of nanoparticles and their mucus barrier modulation ability, which also depends on the type of surfactant. Sodium lauryl sulfate (SDS) increased the composite viscosity and viscoelasticity of mucus, but poloxamer showed a downward trend. Tween 80 largely retains its original mucus rheological and morphological properties and may be a promising candidate for promoting the penetration of nanoparticles into the mucus barrier with good safety. Studies have shown that some small molecules can cross the mucus barrier through free diffusion, but most large molecules do not easily cross the mucus barrier [27]. Therefore, we can infer that the permeability of the mucus layer may be limited by its pore size can be infered [36][<>].
The periciliated liquid layer (PCL) is ideal for cilia flow and is approximately 5-10 μm thick,[4] [4] corresponding to the length of the cilia. If the layer is too thick, cilia cannot reach the upper mucus layer and therefore cannot perform their clearing defense function. At the same time, if this layer is too thin, the upper mucus layer adheres to the cilia and blocks their movement [23]. Hydration of airway surface fluids is critical to achieving mean mucus clearance [25]; In the normal airway [37], water is distributed between the mucus layer and the periciliary fluid layer, and the layer with low osmotic pressure changes its concentration more easily than the layer with high osmotic pressure. Button et al. propose a brush gel model that shows that when the mucus layer is heavily hydrated [4][4], its osmotic pressure drops sharply, so that the liquid from the airway surface enters the mucus layer first, while the PCL remains unchanged. Conversely, when airway dehydration occurs, the mucus layer is dehydrated first, increasing its concentration, increasing the osmotic pressure of the mucus layer, and the PCL layer is compressed under high pressure, causing the PCL to collapse. PCL is a network structure composed of various macromolecular substances, the size of which is not constant between grids, related to the height of the PCL layer [38]. When the airway surface fluid is overhydrated, resulting in the collapse of the PCL layer, the mesh size of the PCL layer is subsequently reduced; Assuming that the drug particles reach the mucus layer, the penetration of the drug particles in the lung mucosa is significantly reduced due to the reduction of the pores in the PCL grid. In addition, a series of changes in the composition and structure of the mucus layer in the pathological state, such as an imbalance in ion transport in the lung airways in patients with cystic fibrosis (CF), leads to a decrease in the volume of fluid on the surface of the airway, a significant increase in the viscoelasticity of the mucus, and impaired clearance of mucocilia [39][40][41][42][39,40,41,42].]。 In addition, under pathological conditions, the concentration of mucin, DNA, and actin increased significantly, significantly reducing the average size and size distribution of the mesh spacing, thereby severely hindering the transport of nanoparticles. Therefore, there is an urgent need for nanodelivery carriers capable of carrying drugs through dense mucus layers.
3. Nanoparticle-Mmediated Eeffective Eenhancement of Drug Rdrug retention and Ppenetration in the Aairway Mmucosa
Based on the barrier properties of airway mucus described earlier, rwesearchers can design different strategies to enhance the penetration of drugs in the pulmonary mucosa according to their characteristics. Among them, nanoparticle formulations have significant advantages in improving cell penetration and therefore may be a promising approach to treating lung diseases [43]. However, when used as a transport carrier, it faces a double barrier of size filtration of the mucus layer and interaction filtration. Since the barrier properties of mucus change its behavior, it is necessary to design nanoparticles appropriately, such as changing the surface properties of nanoparticles (including particle surface functional groups and charge density, etc.), changing their particle size [44][44], etc. In addition, enlarging mucosal lattice voids by disrupting specific non-covalent interactions of mucogel is also an effective way to promote mucosal drug penetration. Table 1 summarizes the various types of nanoparticles that enhance mucus penetration and retention.
Table 1. Summary of nanoparticles for enhanced mucus penetration and retention.
Summary of nanoparticles for enhanced mucus penetration and retention.
| Nanoparticle type | Recipe details | outcome | reference |
|---|---|---|---|
|
|
|
[45] |
|
|
[46] | |
|
|
[47] | |
|
|
|
[48] |
|
|
[1] | |
|
|
|
[49] |
|
|
[50] | |
|
|
[51] | |
|
|
|
[52] |
|
|
[53] | |
|
|
|
[54] |
|
|
[55] | |
|
|
[56] | |
|
|
|
[57] |
|
|
[58] | |
|
|
|
[59] |
| Nanoparticle type | Recipe details | outcome | reference |
|---|---|---|---|
|
|
|
[45] |
|
|
[46] | |
|
|
[47] | |
|
|
|
[48] |
|
|
[1] | |
|
|
|
[49] |
|
|
[50] | |
|
|
[51] | |
|
|
|
[52] |
|
|
[53] | |
|
|
|
[54] |
|
|
[55] | |
|
|
[56] | |
|
|
|
[57] |
|
|
[58] | |
|
|
|
[59] |