Antimicrobial resistance is considered a “One-Health” problem, impacting humans, animals, and the environment. The problem of the rapid development and spread of bacteria resistant to multiple antibiotics is a rising global health threat affecting both rich and poor nations. Low- and middle-income countries are at highest risk, in part due to the lack of innovative research on the surveillance and discovery of novel therapeutic options. Fast and effective drug discovery is crucial towards combatting antimicrobial resistance and reducing the burden of infectious diseases. African medicinal plants have been used for millennia in folk medicine to cure many diseases and ailments. Over 10% of the Southern African vegetation is applied in traditional medicine, with over 15 species being partially or fully commercialized. These include the genera Euclea, Ficus, Aloe, Lippia. And Artemisia, amongst many others. Bioactive compounds from indigenous medicinal plants, alone or in combination with existing antimicrobials, offer promising solutions towards overcoming multi-drug resistance. Secondary metabolites have different mechanisms and modes of action against bacteria, such as the inhibition and disruption of cell wall synthesis; inhibition of DNA replication and ATP synthesis; inhibition of quorum sensing; inhibition of AHL or oligopeptide signal generation, broadcasting, and reception; inhibition of the formation of biofilm; disruption of pathogenicity activities; and generation of reactive oxygen species.
- antimicrobial resistance
- antibiotics
- bioactive compounds
- secondary metabolites
- indigenous plants
- Africa
1. Introduction
2. Clinically Important Multi-Drug-Resistant Bacteria and Modes of Antibiotic Resistance
Antibiotic resistance is found in both Gram-negative and Gram-positive strains of bacteria, which are leading causes of hospital- and community-acquired infections, ranging from common infections such as skin and soft tissue infections to life-threatening infections [4]. MDR bacterial infections account for millions of global deaths annually, with over 40% being neonatal deaths and with that percentage expected to increase in the absence of effective therapeutic drugs [4]. Gram-negative bacteria belonging to the order Enterobacteriales have since developed resistance mechanisms posing a serious threat to human health, especially in hospitals and nursing homes [4][7][16][4,7,16]. Enterobacter species are also Gram-negative and are characterized as facultatively anaerobic, rod-shaped bacteria of the Enterobacteriales family, which includes E. coli and K. pneumoniae [17]. This group of pathogens are a major cause of urinary and respiratory tract infections, causing bacteremia and pneumonia in the immunocompromised [17][18][17,18]. Acinetobacter species (e.g., A. baumannii) are Gram-negative, aerobic, non-fermenting, non-fastidious, ubiquitous coccobacillus, or pleomorphic bacteria, and are responsible for bloodstream infections and ventilator-associated pneumonia [17][18][17,18]. Acinetobacter species have the ability to resist desiccation and form biofilms, and the presence of fundamental virulence factors, such as secretion systems, surface adhesins, and glycoconjugates, aggravate their pathogenicity [19][20][19,20]. Pseudomonas aureginosa, is an example of another Gram-negative bacterium that causes urinary tract infections, surgical site infections, pneumonia, septicemia, and bacteremia, especially in immunocompromised individuals [21]. P. aeruginosa displays innate resistance to a wide array of antibiotics. It is resistant to a wide spectrum of antibiotic classes, including penems and β-lactam, and its resistance to fluroquinolones is due to its ability to mutate on DNA gyrase or topoisomerase [21][22][21,22]. P. aeruginosa employs a variety of mechanisms such as alterations in porin channels, efflux pumps, targets modifications, and β-lactamases to exert resistance to antimicrobial agents [21][22][23][21,22,23]. A. baumannii, P. aeruginosa, and several members of the Enterobacteriales family exhibit broad resistance to carbapenems antibiotics; hence, at the top of the WHO priority list is research and development for new antibiotics, which are urgently needed [17][24][17,24]. The Gram-positive bacteria of clinical concern include the genera Bacillus (e.g., Enterococcus species, Staphylococcus aureus), Clostridium (C. botulinum, C. perfringens), Listeria (L. monocytogenes), Gardenella (G. vaginalis), and Corynebacterium (C. diphtheriae) [24]. Enterococcus faecalis is an enterococcal bacterium that is responsible for infections in the gut of humans, and is known to cause severe infections in immunocompromised individuals [13][16][13,16]. VRE readily accumulate mutations and exogenous genes (VanA, VanB, VanD, VanE, VanG, VanL) that confer resistance to vancomycin, including other antibiotics classes such as β-lactam [25][26][25,26]. S. aureus is a Gram-positive spherical bacterium that is normal microflora of the skin and the nasal mucosa, which can also be pathogenic [27][28][27,28]. Pathogenic strains of S. aureus normally cause life-threatening soft tissue abscesses, pneumonia, septicemia, and bacteremia, and can cause infections from contaminated medical implants. Its ability to form biofilms also poses a challenge in antibiotics-mediated treatments [29]. Additionally, due to the secretion of the TSST-1 exotoxin in some strains, S. aureus can also cause toxic shock syndrome [30][31][30,31]. S. aureus has evolved to develop resistance to vancomycin, methicillin, and many β-lactam classes of antibiotics [31]. MRSA harbors a mecA gene on the staphylococcal cassette chromosome mec (SCCmec) and codes for PBP2a [32]. A protective protein bound to the ribosomes of the bacterial cell inactivates the antibiotics via ‘target alteration’ by altering their structural confirmation [33]. The general mechanisms of antibacterial resistance range from alterations of binding sites, alterations of the bacterial porins’ structure, antibiotics efflux through the bacterial efflux pump structure, and destruction of antibacterial agents by hydrolytic enzymes [5][16][5,16]. Additionally, MDR bacteria can resist antibiotics via one mechanism or by combining more than one to produce their multiple resistance to antibiotics and other antimicrobials, including disinfectants and heavy metals in personal care products [7].3. Diversity and Distribution of African Medicinal Plants with Potential Antimicrobial Properties
Thirty-six promising medicinal plant species are highlighted in this resviearchw. They are widely distributed across the African region. Southern Africa has the majority, followed by East Africa, then Central Africa, while West Africa and North Africa have the least. Hibiscus calyphyllus is common to all the regions; Cassia abbreviata, Dicoma anomala Sond, and Securidosa longipendunculata are also found in all the regions except North Africa. Dichrostachys cinerea is also universal to all regions except West Africa. Fifteen species (Adansonia digitata, Aloe zebrina Baker, Aloe ferox, Artemisia afra, Boscia albitrunca, Colophospermum mopane, Combretum hereroense, Commiphora glandulosa, Cynodon transvaalensis, Euclea undulata, Harpagophytum procumbens, Hirpicium bechuanense, Lippia javanica, Ozoroa paniculosa, Sanseviera scabrifolia, Sclerocarya birrea) were found to be unique to the Southern African region, nine (Elephantorhiza goetzei, Grewia bicolor, Grewia flava, Harpagophytum procumbens, Lippia scaberrima, Mimusopus zeyheri, Myrothamnus flabellifolius, Scadoxus puniceus, Terminalia sericea) are common to Southern and East Africa, and two (Capparis tomentosa, Laphangium luteoalbum) are found only in Southern and North Africa. Asparagus africanus, Vanguera infausta, Ximenia americana, and Ximenia caffra were found to be distributed in Central, East, and Southern Africa. Over 10% of the Southern African vegetation is applied in traditional medicine, with over 15 species being partially or fully commercialized, which can be found in local pharmacies. These include Hibiscus calyphyllus, Harpagophytum procumbens, Cassia abbreviata, Aloe ferox, Lippia javanica, and Artemisia afra, amongst many others [34][35][36][37][38][39][35,36,37,38,39,40]. C. abbreviata, which is also known as long-tail Cassia (or Monepenepe in Setswana, a native language of Botswana), belongs to the Caesalpiniaceae family and is characterized by thick bushes, brown bark, a rounded crown, yellowish leaves, and sweet-scented flowers, as well as long cylindrical dark brown fruits hanging in pods [40][41]. The sun-dried bark is boiled in water and served as a hot tea to individuals with miscellaneous stomach ailments, skin problems, and STIs [37][38]. H. calyphyllus, described as a large yellow hibiscus (or Motsididi in Setswana), is a leafy shrub with wide and simple serrate leaves and yellow flowers with a dark red center, belonging to the Malvaceae family [39][40]. The flowers, which have been reported to be rich in flavonoids and phenolic acids, are traditionally sun-dried, boiled, and served as a hot beverage to treat intestinal ailments in many sub-tropical parts of Africa [39][41][40,42]. A. afra, also known an African wormwood, belongs to the Asteraceae family [42][43]. It is an erect, perennial woody shrub with oval-shaped, greyish-looking leaves. The leaves, stems, and roots are rich in terpenoids, tannins, saponins, and glycosides, which are active against colds, coughs, influenza, sore throat, malaria, asthma, pneumonia, and diabetes [43][44]. These parts of the plants are served pulverized as a hot beverage [44][45]. L. javanica (lemon bush), of the family Verbenaceae, is a woody shrub with aromatic leaves that gives a lemon-like smell, which is used as a culinary spice, as well as to treat coughs, colds, fever, chest ailments, kidney stones, measles, rashes, and stomach problems [36][45][37,46]. Small, dense spikes of white flowers are borne in the axils of leaves. Dried lemon bush leaves are boiled and consumed as is or applied on affected areas [46][47]. H. procumbens of the sesame seed or Pedaliaceae family, popularly known as devil’s claw, is rich in terpenoids, iridoid glycosides, glycosides, and acetylated phenolic compounds [46][47]. It is a tuberous perennial plant with creeping stems and dark pink flowers. Devil’s claw is used for a wide variety of health conditions in the form of hot or cooled infusions, decoctions, tinctures, powders, and extracts to treat blood diseases, urinary tract infections, postpartum pains, sprains, sores, sexually transmitted diseases, ulcers, and boils [47][48]. Commercially, the secondary tubers or roots are pulverized into capsules [46][47]. Aloe ferox (Xanthorrheaceae, previously Asphodelaceae, Aloaceae, or Liliaceae; commonly known as the bitter aloe in English and kgwaphane or mokhwapha in Setswana) is a cherished, popular, ornamental single-stemmed plant with erect racemes of red, orange, yellow, or rarely white flowers, with spreading or gracefully curved thorny leaves [48][49][49,50]). Traditionally, the fresh leaf is cut up, the flesh is extracted and directly applied on the affected areas, and it is consumed as is or diluted in cold water [38][39]. Commercially, it is incorporated into different cosmetic products, health drinks, foods, and beverages to deal with various ailments [49][50]. B. albitrunca is a medium-sized evergreen tree belonging to the Capparaceae or Caper family and is served as hot coffee or tea [50][51]. The bark, leaves, and roots are mainly used as herbal medicines for STIs and skin and stomach infections [50][51]. In fact, in a study by Pendota et al. in 2015, crude, dichloromethane, ethyl acetate, and butanol leaf extracts were evaluated and confirmed for antibacterial activities against B. subtilis, S. aureus, E. coli, and K. pneumoniae. Motlhanka et al. conducted a study to assess the antibacterial properties from the resin of C. glandulosa. This is a single-stemmed tree with greyish-green to yellowish-green flaking bark that belongs to the family Burseraceae [51][52]. Crude aqueous and chloroform extracts of the stem resin, as well as the isolated compound, exhibited good in vitro antibacterial activity against Gram-positive bacteria, B. subtilis, C. perfringens, and S. aureus, as well as multi-drug-resistant S. aureus, XU212-tetracycline-resistant, and SA1199B-norfloxacin-resistant strains [46][47]. X. caffra (Ximeniaceae), commonly known as “sour plum”, is traditionally used both topically and orally to treat a wide range of bacterial infections such as wounds, STIs, respiratory ailments, digestive tract ailments, colds, and coughs [52][53][53,54]. Phytochemical investigations of the bark, fruits, leaves, roots, and seeds of the sour plum revealed various compounds, including flavonoids, phenols, phytosterols, and tannins as active compounds against bacterial pathogens [54][55]. The methanol extracts of X. caffra roots exhibited antibacterial activities against S. aureus and S. epidermidis [55][56]. D. cinerea is a thornbush belonging to the Leguminosae subfamily Mimosoideae. It is a medicinal plant that is native to Africa and rich in tannins in its leaves, bark, and roots [56][57][57,58]. Tannins were isolated from D. cinerea and assayed against S. aureus, S. boydii, S. flexneri, E. coli, and P. aeruginosa using the agar diffusion method [56][57]. The associated tannins exhibited antibacterial activities against all test microorganisms. This explains why the dried bark, roots, and leaves are served as a hot tea to traditionally treat sexually transmitted, respiratory, dental, skin, and intestinal infections [57][58]. In a study aimed at investigating the in vitro antimicrobial activity of ethanolic extracts of seventeen species of Sansevieria, including S. scabrifolia, against E. coli using the agar disk diffusion method, a degree of inhibition was found [34][35]. The leaves of this species are used to treat ear infections, toothache, and diarrhea [53][54]. C. tomentosa (belonging to the family Capparaceae) is a scrambling shrub that grows as high as 10 m tall and is found across North Africa and Southern Africa. It is used to treat pneumonia, coughs, headaches, tuberculosis, and gonorrhea [58][59]. The associated phytochemicals that are extracted from the hairy yellow-green twigs and leaves are linked to its unique biological, bactericidal, and bacteriostatic activities, which include alkaloids, L’stachydrine, saponin glycosides, phytosterols, terpenoids, tannins, and anthranoids [58][59]. Studies have shown that this species has good antimicrobial activity against antibiotic-resistant S. aureus, S. pyogenes, E. coli, and P. aeruginosa [59][60]. O. paniculosa (Anacardiaceae) is an evergreen, semideciduous, small- to medium-sized single-stemmed tree that is rich with phenols [60][61]. Phenolic-enriched leaf extracts of O. paniculosa were prepared using a mixture of 1% HCl-acidified 70% acetone and n-hexane, and then tested against S. aureus, P. aeruginosa, E. coli, and E. faecalis [60][61]. These extracts had good activities relating to diarrhea mechanisms or pharmacological relevance. E. undulata (belonging to the Ebenaceae or Ebony family) has egg-shaped to wide, bluntly pointed waxy leaves, yellowish fragrant flowers, and globose fleshy fruits that are all traditionally used for the treatment of body pains, chest complaints, cough, diarrhea, headaches, heart disease, and tooth aches because of their wealth of diterpenes, flavonoids, naphthoquinones, phytosterols, saponins, and tannins [61][62]. In a previous study, the antimicrobial activity of E. undulata chewing sticks against multi-drug-resistant S. mutans was determined [62][63]. The minimum inhibitory concentrations ranged from 0.385 to 11.22 mg/mL and the minimum bactericidal concentrations from 0.485 to 20.20 mg/mL. T. sericea (of the family Combretaceae) is a small to medium deciduous rounded flowering shrub whose roots are traditionally used to treat diarrhea, skin rashes, tuberculosis, and opportunistic infections associated with HIV/AIDS in Botswana [63][64]. It has been reported that dichloromethane/methanol (1:1) extracts of the stems, bark, leaves, and roots have antibacterial activity against B. subtilis, B. cereus, S. aureus, E. coli, K. pneumoniae, P. aeruginosa, S. sonnei, S. typhimurium, and S. epidermidis [64][65]. The compounds isolated from this species so far include a triterpene sericoside, resveratrol-3-O-β-D-rutinoside, and hydroxystilbene glycoside [65][66]. S. scabrifolia (also known as Mosokelatsebeng in Setswana) is a stemless evergreen perennial succulent that grows from a thick rhizome. Its fleshy leaves are warmed in a fire and the juice is squeezed into the ear or tooth to treat ear infections and cavities in Botswana [53][54]. In Namibia, the leaf sap is applied to wounds to prevent infection and accelerate healing [66][67]. This bactericidal capacity was also confirmed by Tkachenko et al., showing that the crude extracts had antibacterial activity against pathogenic E. coli [66][67]. The antibacterial activity in the Sansevieria genus may be due to the presence of alkaloids, saponins, terpenoids, steroids, glycosides, and tannins [64][65].43. Plant Secondary Metabolites with Antimicrobial Potential
Plants are known to synthesize and produce diverse groups of organic compounds that are involved in assorted metabolically related functions of the plant, known as secondary metabolites [67][81]. Their primary function to the plants is in the interaction of the plant with the environment, and they are mostly released in response to abiotic and biotic stresses, thereby supporting plant survival as molecules of defenses [68][82]. Examples of classes of secondary metabolites include terpenoids, phenols, and derivatives, as well as glucosinolates and alkaloids [69][70][83,84].43.1. Alkaloids
Alkaloids are nitrogenous compounds that can be classified as natural, semi-synthetic, and synthetic or based on their chemical structure into typical alkaloids with a heterocyclic ring or atypical alkaloid non-heterocyclic ring [5]. Additionally, they may be split into several classes: tropanes, indole, purines, imidazole, pyrrolidine, pyrrolizidine, isoquinoline, piperidine, and quinolizidine [71][85]. The antibacterial capacity of alkaloids has been documented and has been linked to efflux pump inhibition, bacterial cell wall synthesis inhibition, changes in cell membrane permeability, inhibition of bacterial metabolism, and nucleic acid and protein synthesis [71][72][85,86]. For example, strychnine from C. tomentosa has antibacterial activity against E. coli, P. aeruginosa, and K. pneumoniae. Other plant-associated alkaloids include nicotine, ephedrine, morphine, and quinine (Figure 1).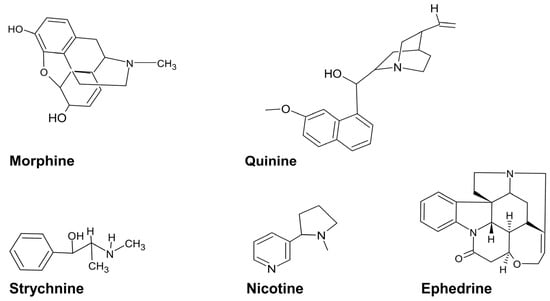
43.2. Polyphenols
Polyphenols are a large group of secondary metabolites that are classified according to their phenolic groups and structural elements as flavonoids, stilbenes, lignans, tannins, and phenolic acids [73][87]. The antibacterial capacity levels of polyphenols towards Gram-negative and positive MDR bacteria have been linked to their ability to bind to bacterial enzymes via a hydrogen bond, inducing several modifications in cell membrane permeability and cell wall integrity [72][74][75][86,88,89]. Examples include catechin from Adansonia digitata and vitexin from tannic acid from Dichrostachys cinerea. Tannin is a descriptive name for a group of polymeric phenolic substances capable of tanning leather or precipitating gelatin from solution [56][57].43.3. Terpenes
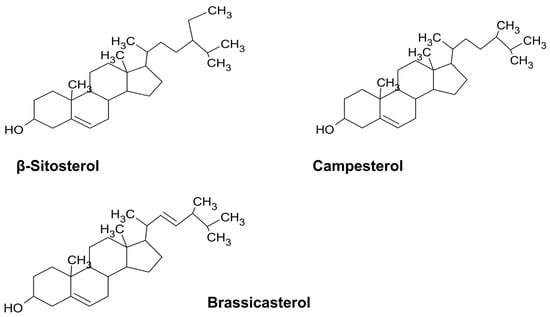
Terpenes are a large group of hydrocarbons synthesized from the 5-carbon precursor units of isopentenyl pyrophosphate and its functional isomer dimethylallyl pyprophosphate [76][90]. According to the number of isoprenes, they are classified into monoterpenes (e.g., limonene from A. afra), diterpenes (e.g., retinol), triterpenes (e.g., oleanolic acid from the Hibiscus spp.), and tetraterpenes (e.g., lutein, brassicasterol, campesterol, and β-sitosterol from Artemisia) [34][77][78] (Figure 2)[35,91,92]. The broad antibacterial activity of the terpenes includes efflux pump inhibition and the inhibition of bacterial growth and membrane properties towards MDR bacteria E. coli, S. aureus, and Enterobacter species [77][79][80][91,93,94].