|
Cancer Type
|
Findings
|
Methods
|
Refs.
|
|
Oral cancer
|
C. albicans enhances the proliferation, migratory processes, as well as invasion of oral squamous cell carcinoma cells in laboratory conditions and also promotes tumor growth and metastases in test animals.
|
Modulation of tumor cell behavior and the host immune response by upregulating oncogenes and potentiating a premalignant phenotype.
|
[16][20]
|
|
C. albicans infection enhances the expression of interleukin-17A(IL-17A) and its receptor (IL-17RA) in oral cancer cells and macrophages.
|
The increased IL-17A/IL-17RA signaling activates macrophages and promotes the release of inflammatory cytokines, which in turn enhances the proliferation, migration, and invasion of oral cancer cells.
|
[17][21]
|
|
Immune cell infiltration was observed in carcinogenesis prompted by C. albicans infection.
|
Single-cell expression profiling
|
[18][22]
|
|
Upregulation in programmed death-ligand 1 (PD-L1) expression in oral cancer cells.
|
Inhibition of T cell activation and proliferation by upregulation of programmed death-ligand 1 (PD-L1) expression in vivo and in vitro.
|
[19][23]
|
|
C. albicans biofilm may contribute to the development and progression of oral cancer.
|
Induction of lipid droplet formation and decreasing the efficacy of chemotherapy drugs
|
[20][24]
|
|
Genetic mutations and chromosomal abnormalities can be associated with the development of cancer.
|
DNA damage and inhibition of DNA repair mechanisms cause by acetaldehyde.
|
[21][25]
|
|
Genetic mutations and chromosomal abnormalities can be associated with the development of cancer.
|
Reactive oxygen species promote chronic inflammation and cause mitochondrial damage.
|
[22][26]
|
|
Esophageal cancer
|
Development of epidermoid esophageal cancer.
|
Treatment-resistant esophageal candidiasis.
|
[23][27]
|
|
Chronic mucocutaneous candidiasis leads to squamous cell carcinoma.
|
Mutation in STAT1 protein
|
[24][25][28,29]
|
|
Gastric
cancer
|
An imbalance in fungal communities with changes in fungal composition and a large increase in the abundance of C. albicans leads to gastric cancer.
|
The increase in C. albicans is involved in the decrease in the abundance and diversity of other gastric fungi.
|
[26][30]
|
|
Deletion of the Dectin-3 gene led to a substantial increase in colorectal cancer development, with fungal burden in the feces of knockout mice.
|
The deletion of the Dectin-3 gene led to a significantly increased abundance/proportion of C. albicans in knockout mice.
|
[27][31]
|
|
Differences in the composition of the feces and abundance of C. albicans could promote the process of colorectal carcinogenesis.
|
Transplantation of feces from knockout, cancer-bearing mice into other mice confirmed that the feces and C. albicans could promote the process of colorectal carcinogenesis.
|
[27][31]
|
|
Skin
cancer
|
Compared with the control group, patients with Candida infection had a significantly higher risk for overall skin cancer.
|
A case-control study enrolled 34,829 patients with Candida infection and an equal number of controls.
|
[28][32]
|
|
Progression of verrucous candidiasis of lip to SCC after 12 months of follow-up.
|
A case report
|
[29][33]
|
3. The Role of Candida in Oral Malignancy
The most common cancer observed in the oral cavity is planocellular carcinoma, also known as oral squamous cell carcinoma, which comprises over 90% of oral cancers
[30][31][97,98]. It can develop in various sites of the mouth, including the tongue, buccal mucosa, lips, gingiva, or palate. In more than half of cases, oral planocellular carcinoma develops from premalignant lesions characterized by the appearance of white deposits or red lesions on the mucosa (leukoplakia/erythroplakia). Unfortunately, a prognosis and five-year survival rates are not particularly good, and 50% of cases end lethally
[32][33][99,100].
The relationship between
Candida spp. and oral carcinogenesis has been a topic of discussion for a long time. Various possible ways in which this fungal genus may interact with the development of oral cancer have been suggested
[22][34][26,47]. Several mechanisms that have been proposed are the induction of genetic instability in oral cells, promotion of epithelial cell transformation, carcinogenic byproducts, immune modulation, and chronic inflammation
[15][16][19,20]. A recent systematic review concluded that the existence of a hallmark species of the genus,
C. albicans, in the oral cavity could be linked to the development of oral cancer due to the changes it causes in the phenotypic structure of the cell, but also as a result of genotypic modifications
[35][101]. Additionally, it was emphasized that
C. albicans produces carcinogenic substances that can promote oral cancer progression
[35][101] (
Figure 1).
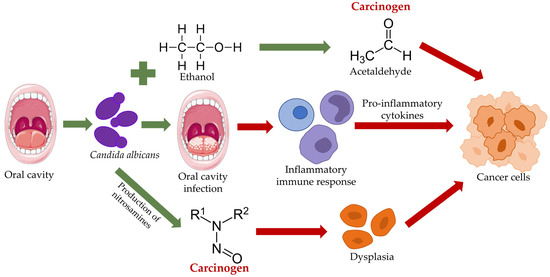
Figure 1.
An overview of the various pathways by which
Candida albicans
may contribute to the development of oral cancer.
Research suggests that
C. albicans can directly promote the development of oral cancer by producing certain carcinogenic enzymes and other substances that can damage DNA and promote the growth and survival of cancer cells. Some specific compounds in that realm are nitrosamines and acetaldehyde
[36][37][102,103]. The ability of oral
Candida to metabolize alcohol into acetaldehyde has proven to be very important. Acetaldehyde is known to cause DNA damage and inhibit DNA repair mechanisms, leading to genetic mutations and chromosomal abnormalities associated with cancer development
[21][25]. This substance also binds indirectly to the important antioxidant glutathione, which increases the presence of reactive oxygen species, promotes chronic inflammation, and causes mitochondrial damage
[22][38][26,104]. In addition, infection with
C. albicans can suppress the immune system, making the host more susceptible to developing cancer. Finally, this fungus can also interfere with apoptosis or programmed cell death, which generally helps remove damaged or abnormal cells from the body, allowing them to continue proliferating and potentially leading to cancer
[39][105].
This is in agreement with some recent findings. A study from Hungary demonstrated how
C. albicans enhances the proliferation, migratory processes, as well as invasion of oral squamous cell carcinoma cells in laboratory conditions and also promotes tumor growth and metastases in test animals
[16][20]. These authors observed that
C. albicans infection increases gene expression pertinent to cell cycle regulation, frank inflammation, and epithelial-mesenchymal transition in cancerous cells. Such findings suggest that
C. albicans may contribute to the progression of oral squamous cell carcinoma (both in early and late stages) through the modulation of tumor cell behavior and the host immune response by upregulating oncogenes and potentiating a premalignant phenotype, which has substantial implications for clinical practice
[16][20].
Wang et al. aimed to investigate the underlying mechanism of how
C. albicans promotes oral cancer from the vantage point of the tumor immune microenvironment
[40][55]. They have discovered that a
C. albicans infection enhances the expression of interleukin-17A (IL-17A) and its receptor (IL-17RA) in oral cancer cells and macrophages. Consequently, the increased IL-17A/IL-17RA signaling activates macrophages and promotes the release of inflammatory cytokines, which in turn enhances the proliferation, migration, and invasion of oral cancer cells
[17][21]. In addition, the study shows that
C. albicans-induced IL-17A/IL-17RA signaling promotes the growth of oral cancer xenografts in vivo
[17][21].
There is further evidence for this association. By using single-cell expression profiling, Hsieh et al. found that immune cell infiltration can be observed in carcinogenesis prompted by a
C. albicans infection and elucidated comprehensive mechanisms that underpin such processes
[18][22]. Wang and colleagues established how
C. albicans upregulates the expression of programmed death-ligand 1 (PD-L1) in oral cancer cells both in vitro and in vivo, leading to an inhibition of T cell activation and proliferation
[19][23]. Moreover, Marin-Dett et al. (2023) found that a
C. albicans biofilm may contribute to the development and progression of oral cancer by inducing lipid droplet formation and decreasing the efficacy of chemotherapy drugs
[20][24]. Although there are no clear-cut conclusions for now, there is increasing evidence to suggest that the presence of this
Candida species is indeed linked to a higher risk of oral squamous cell carcinoma development
[41][106].
Another important virulence factor that may play a role in the influence of
C. albicans on the development of oral cancer is candidalysin. Candidalysin is a protein toxin secreted by the fungus
C. albicans, which is known to cause oral candidiasis, a common fungal infection in the mouth. The significance of candidalysin in the development of oral cavity carcinoma is not yet completely understood; still, some research suggests that it may play a role in the early stages of carcinogenesis
[42][77]. Studies have shown that candidalysin can activate the immune system and promote inflammation, possibly contributing to cancer development. In addition, candidalysin has been found to interact with and disrupt oral epithelial cell membranes, which can lead to DNA damage and mutations
[43][78]. In addition, candidalysin has been shown to promote angiogenesis and the formation of new blood vessels. Angiogenesis is a crucial step in the growth of cancer and metastasis of primary tumors in other tissue and organs, suggesting that candidalysin may contribute to the progression of oral cavity carcinoma. Overall, although more research is needed to fully understand the role of candidalysin in oral cavity carcinoma, it is clear that this toxin may play an important role in the development and progression of this disease
[44][45][107,108].
It has to be emphasized that
C. albicans normally colonizes the oral cavity of humans
[46][47][109,110]. It is the most abundant yeast fungus on both the healthy and infected oral mucosa
[1][46][1,109], which is why there is a need for further studies to establish the link in the chain of cancer development fully. Its conversion to a pathogenic state and the occurrence of opportunistic infections are the results of disturbances in homeostasis caused by various environmental and hereditary factors, which may be local or systemic
[1].
It has long been known that
C. albicans infection of the oral cavity is pervasive in oncology patients as a result of chemotherapy and radiotherapy and—as an opportunistic pathogen that takes advantage of the state of immunosuppression—has usually been associated with malignancies
[14][48][49][18,111,112]. However, alongside the already mentioned studies, its role in initiating and developing oral cancer has recently been increasingly studied
[14][22][34][35][48][50][51][18,26,47,101,111,113,114].
C. albicans infections in the oral cavity have a wide spectrum of manifestations; on this basis, there are several subdivisions of candidiasis. The color of the change in the mouth can be divided into red and white and, according to the origin, into primary and secondary. Primary candidiasis refers to infections that affect only the perioral area and oral cavity. However, when the infection occurs in the context of systemic diseases and the mucosa is already altered (and, thus, amenable to infection), it is referred to as secondary candidiasis
[1][52][1,115]. Pseudomembranous candidiasis, acute erythematous candidiasis, chronic erythematous candidiasis, and chronic hyperplastic or nodular candidiasis are considered primary forms of the disease. Conversely, angular cheilitis, medial rhomboid glossitis, and chronic mucocutaneous candidiasis are secondary
[1][46][52][1,109,115].
Chronic hyperplastic candidiasis, also known as
Candida leukoplakia, has the highest rate of malignant transformations of the aforementioned
Candida-induced oral lesions
[35][49][53][101,112,116]. It is characterized by white deposits on the mucous membrane that cannot be easily removed with gentle scraping. This distinguishes it from other types of candidiasis and lesions that also appear in the form of white deposits. The reason for this is fungal hyphae’s deep infiltration of the oral cavity tissues. White deposits in the mouth can be homogeneous or heterogeneous, with the latter being particularly prone to malignant alteration. Changes on the oral mucosa are usually painless but may be sensitive to touch, spicy foods, or heat. They can occur anywhere in the mouth but are most common on the lateral parts, under the tongue, and on the buccal mucosa
[1][52][1,115]. The exact cause of oral leukoplakia is unknown; nonetheless, it is thought to be related to a chronic irritation of the oral tissues, such as from smoking, rough teeth, or dental appliances. Treatment for oral leukoplakia usually involves eliminating the source of irritation, such as smoking cessation or replacing bad-fitting dental appliances and monitoring the patches for changes or growth over time. In some cases, a biopsy may be needed to determine whether the patches are cancerous or precancerous
[54][117].
A
Candida infection has been suggested to act as a co-carcinogen in the presence of other risk factors. For example, in individuals who smoke or consume alcohol excessively, a
Candida infection may synergistically interact with these habits to increase the risk of developing oral precancerous lesions
[35][101]. Although the importance of
C. albicans in oral cancerogenesis is not fully understood, some evidence suggests that it may play a contributing role. Studies have shown that chronic inflammation, which can be caused by a
C. albicans overgrowth, is a key factor in the formation of many cancers, including oral cancer. In addition, interactions between
Candida and other groups of oral microorganisms may contribute to the development of specific oral diseases. For example,
Candida has been found to interact with bacteria such as
Streptococcus mutans, which is related to dental caries and
Porphyromonas gingivalis, which is related to periodontal disease. These interactions can subsequently lead to the formation of mixed-species biofilms, which can increase the virulence of these microorganisms and contribute to the progression of severe oral diseases—including oral premalignancy and malignancy
[34][47].
In a nutshell, individuals with chronic or recurrent
Candida infections, particularly those with compromised immune systems or other risk factors for oral cavity cancer, may be prone to develop cancer of the oral cavity
[1]. Maintaining a healthy oral microbiome through good oral hygiene and continuous dental visits can help prevent these conditions from developing. For these individuals, it is important to seek immediate medical attention for oral symptoms, such as white patches or sores, as well as treat the underlying risk factors to prevent the potential occurrence of oral cancer
[55][118].