|
Layer
|
Major cellular Constituents
|
Major Functions
|
References
|
|
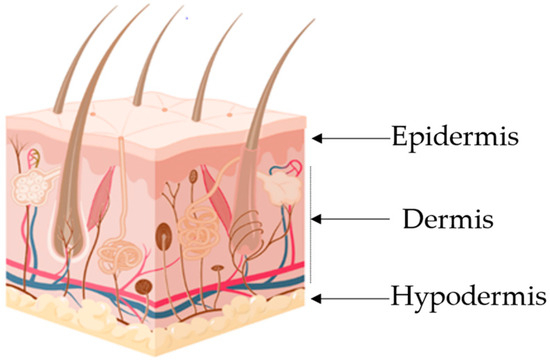
Hypodermis
|
Adipocytes, fibroblasts, endothelial and muscle cells
|
Insulation, mechanical integrity, support, conductance of vascular and neural signals
|
[1][2][1,2]
|
|
Dermis
|
Endothelial cells, fibroblasts, Langerhans and muscle cells
|
Mechanical integrity, support, thermal barrier, energy storage, protection from physical injury
|
[2][3][2,3]
|
|
Epidermis
|
Keratinocytes, melanocytes, Langerhans and Markel cells
|
Outermost barrier, immune function, protection from oxidative and mechanical stress
|
[4][5][4,5]
|
2. Atopic Dermatitis
Atopic dermatitis is one of the most common and recurrent chronic non-infectious skin inflammatory diseases, which is characterized by a persistent itching sensation in the skin. It is a skin disorder that usually appears in early childhood (about 80% of the cases) and is reported to affect 15–20% of children. Although ca. 70% of paediatric patients outgrow the disease, the prevalence in adults remains around 1–3%, although the figures vary greatly from country to country
[6][7][8][9][6,7,8,9]. AD’s worldwide prevalence is rising, with two- to three-fold increases in incidence in industrialized countries being reported for the last decades, having reached a plateau only in countries where its prevalence is highest
[7][10][7,10]. In contrast to most allergic diseases, AD has a high social and economic impact. The chronic skin inflammation with continuous itching leads to skin thickening, lichenification and overall discomfort. This will lead to a compromise in sleep patterns, which have social consequences and create economic burdens. All of these social and economic impacts are what makes AD a disease with a high toll on patients and their families
[11][12][11,12].
From a clinical standpoint, AD belongs to the spectrum of atopic disorders, such as allergic asthma or food allergies. Coincidently, these are companion diseases of AD patients due to the commonly denominated “atopic march”, a curious denomination given to the range of allergic disorders that, in later years, manifest in AD patients
[13][14][15][13,14,15]. Atopic dermatitis clinical diagnostics are characterized by eczema-like eruptions, papules, exudative lesions, and various degrees of skin dryness. In addition, there are several comorbidities, such as skin infections and cardiovascular and neuropsychiatric disorders, which have also recently been associated with AD, despite the mechanism behind these associations being still unknown
[11][16][17][18][19][20][11,16,17,18,19,20]. As with most atopic diseases, there is a strong environmental link with immunoglobulin E (IgE)-related environmental responses, with this factor being one of the primary drivers of AD outbreaks
[21]. However, AD is a complex multifactorial disease that cannot be attributed to one single cause.
From a pathophysiologic standpoint, AD results from several genetic defects that potentiate the immune response and disrupt the skin barrier. The most reported mutations are associated with filaggrin (FLG) production, which have been recognized as some of the most relevant, with various authors reporting that up to 60% of Europeans with AD exhibit alterations in FLG expression
[11]. Another defect which plays a key role in AD are tight junctions (TJs) mutations and alterations. These are structures that have a connection role between cells, exist in every human epithelium, and have various roles depending on the tissue they are located in (e.g., homeostasis control in the central nervous system or impeding the penetration of pathogens in the intestine)
[22][23][22,23]. In healthy skin, TJs are part of the mechanism for managing cellular differentiation, proliferation and cascading processes involved in maintaining and managing skin homeostasis and permeability
[24][25][24,25]. On the other hand, in AD patients, TJs are normally dysfunctional and contribute to the irregular barrier function of the skin. They appear to impede stratum corneum (SC, the outermost layer of the epidermis) formation due to increased pH values and, among other effects, affect the processing of polar lipids and profillagrin, both of which are critical for SC formation. All these alterations lead to increased permeability to exogenous material and bacteria, which results in an increased inflammatory condition and a vicious circle, where the barrier dysfunction potentiates the skin’s inflammatory response. Interestingly, the TJ dysfunction is not directly affected by the FLG mutation, with both mechanisms appearing to be independent
[26][27][26,27].
In addition to these two main alterations, several other structural proteins have been described as downregulated in AD, such as desmogleins, desmocolins, involucrin and keratins
[28][29][30][31][32][28,29,30,31,32]. These alterations to expression and mutations again result in compromise of the skin’s shield function, increased transepidermal water loss (i.e., higher dehydration), and an increased exposure to external toxins and allergens that translates into activation of the local immune system.
Of all the identified changes, the FLG mutation is a particularly interesting one when seeking to understand the cascade of potential problems that arise from a single mutation: (1) it disrupts the production of moisturizing factors in the skin’s stratum granulosum; (2) it disrupts lamellar body secretion and, therefore, alters the composition of the SC; (3) it arrests the metabolic pathway part-way through resulting in the absence of acidic metabolites. This translates into an upswing of the SC pH and allows for an increase in proteolytic enzyme activity (increased desquamation) and the proliferation of
Staphylococcus aureus (
S. aureus), a bacterial species whose predominance in skin flora has been strongly associated with AD flares
[17][33][34][35][17,33,34,35].
Considering the pathophysiology of AD, it would be natural to expect that its treatment would involve a multifaceted approach capable of mitigating or ameliorating several facets of the disease, with a multitude of approaches and options for patients. However, this could not be further from reality. As AD is considered as being only a skin disorder, the treatments follow the paradigm “one-size-fits-all”, with solutions being very limited, and an almost recipe-like approach being followed by physicians all over the world
[21]. In fact, most AD patients’ treatment has, as a first line of approach, anti-inflammatory treatment, more particularly, topical corticosteroids or topical calcineurin inhibitors, in conjunction with an antimicrobial ointment to help with
S. aureus control
[36][37][47,48]. For more severe cases, this is normally followed by the use of ultraviolet light and potent cocktails of immunosuppressant drugs, such as ciclosporin A, methotrexate and mycophenolate mofetil
[21][36][38][21,47,49]. These regimens, while mostly effective, are not without costs, as several side-effects related to cutaneous application of immunosuppressants are well-described in the literature
[39][40][50,51]. Thus, there has been an increasing demand for alternative solutions to AD treatment.
Currently, there are already some therapeutic alternatives being tested, such as Janus kinase inhibitors (e.g., Delgocitinib and Ruxolitinib), phosphodiesterase-4 inhibitors (e.g., Crisaborole and Difamilast) and aryl hydrocarbon receptor agonists (e.g., Tapinarof), all of which, through topical application, target the inhibition of enzymes, receptors or transcriptional factors involved in AD
[41][42][43][52,53,54]. Another option is the use of human monoclonal antibodies (mAbs), which are also already being applied in AD patients via systemic application
[44][45][55,56]. However, both of these alternatives are used mainly for moderate to severe cases and, thus, are not suitable for everyday applications
[46][57]. Thus, alternatives are still required for the daily management of AD. Among the natural alternatives currently being studied, antimicrobial peptides (AMPs) are some of the most promising.
3. Antimicrobial Peptides
By definition, AMPs are small molecules that are widely present in nature and are part of the immune response of most human inflammatory responses. They are generally constituted by 100 amino acid residues or less and have a positive net charge and amphiphilic structure, which provides these molecules enhanced biological potential due to their natural strong interaction with hydrophobic surfaces and membranes
[47][58]. In terms of their characterization, AMPs can be divided according to their structure (α-helical, β-sheets, extended peptides and loop peptides) and covalent bonds (class I to IV)
[48][59].
In the context of the epidermis, naturally produced AMPs play a crucial role in the maintenance of a healthy skin microbiome through modulation of the microbiota composition, proliferation and death, and, thus, also play a role in the metabolites produced by them. Produced within the epidermis, primarily in keratinocytes, this family of ca. 20 peptides not only exhibits antibacterial activity, but these peptides also exert immunomodulatory effects as they activate various cell-related functions, such as migration and proliferation, regulate cytokine production and help maintain the skin’s barrier function, and play critical roles in both innate and adaptative immunity
[49][75]. In this family, the most studied AMPs are defensins, LL-37, RNase 7, psoriasin and dermcidin, with most of these AMPs being expressed at basal or low levels in healthy skin, with the only exception being the β-defensin AMPs which are crucial for the homoeostasis of healthy skin and its protection against infections
[50][76]. For the ones that are expressed at basal levels, their production is normally induced in injury, inflammation or infection scenarios
[12][49][50][12,75,76].
Disruptions to AMP production or activity have been shown to contribute significantly to the increased susceptibility of AD patients to skin infections by fungi, bacteria and viruses and, thus, are perceived as an important factor in AD pathophysiology
[11]. In fact, in AD patients AMPs such as Dermcidin, LL-37 and β-defensins are un-der-expressed, a fact that has been shown to directly influence the progression of AD. This is due to these AMPs being involved in numerous adaptative and innate immune responses (through the recruitment of a broad range of leukocytes) among which are: (i) the regulation of the itch sensation; (ii) secretion of IL-31 from mast cells induced by β-defensins and LL-37; (iii) under expression of AMPs, due to overexpression of Th2 cytokines, hampering S. aureus killing in keratinocytes
[12][16][12,16]. On the other hand, under AD conditions, some AMPs are overexpressed, such as Rnase7, leading to imbalances in the skin microbiota. There is also the curious case of β-defensins and LL-37, which can be the cause of their own inhibition, as they recruit and activate a broad range of leukocytes. This leads to the production of IL-4, IL-13 and IL-31, the major interleukins involved in the development of AD, thus creating a perfect inflammatory environment for the pathogenesis of AD and their own inhibition
[51][83].
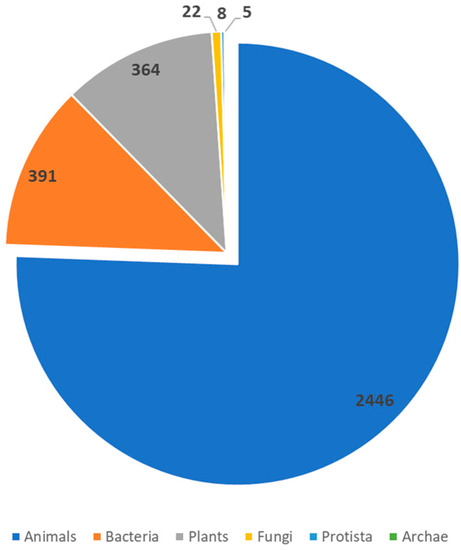
With this clear influence upon various and critical factors involved in AD pathogenesis, AMPs have risen to prominence as valid alternatives for the treatment/management of AD. In recent years, research has centered on the use of AMPs either as an alternative to antimicrobials or as a pharmaceutical agent capable of exerting immunomodulatory activity, with several natural and synthetic sources being explored. A total of 3324 AMPs has now been registered with the Antimicrobial Peptide Database from sources of the six traditional kingdoms (bacteria, archaea, protists, fungi, plants and animals) (
Figure 2)
[52][84].
Figure 2.
Distribution of known AMPs across the different sources. Data accessed from the Antimicrobial Peptide Database
(accessed on 15 August 2023).
From a mechanistic standpoint, the application of AMPs as pharmacodynamic agents is dependent on a variety of factors (such as peptide concentration, tissue location, the local environment and the target pathogen) that one must consider when evaluating AMP potential application in skin and AD in particular
[53][85]. While there are some disadvantages regarding the clinical application of AMPs, like their rapid degradation by esterases or aminopeptidases and their low stability in vivo, there are also advantages to their use. These include their capability for penetrating deeper skin layers, as shown by their presence in viable skin even 24 h after application, and the fact that AMP-based treatment provides opportunities for interventions that closely resemble natural pathways and represent more of a replacement therapy than conventional treatment. In this regard, they supplement patients with AMPs in locations where their endogenous levels are low or absent and, consequently, are less likely to promote adverse responses
[52][54][84,86]. Furthermore, even the previously mentioned disadvantages do not represent a limitation to AMP application in AD management, as, nowadays, there are several strategies to enhance their bioavailability and overcome their limitations. These include, penetration enhancers, encapsulation, or even chemical modification to increase AMP permeability through the skin
[55][87].
4. AMPs in Clinical Trials
As with all pharmaceutical-related applications, clinical trials are the last and crucial step that a formulation must pass to be European Medicines Agency (EMA) or Food and Drug Agency (FDA) approved for human application
[56][106]. The purpose of these trials is twofold—first, to validate in vivo the biological activity verified in vitro; second, to establish a safety profile of the formulated peptides so correct dosages and side-effects can be correctly ascertained
[57][107].
As can be seen in
Table 2, there are numerous examples of AMPs under consideration with a vast array of applications being considered, with their status ranging from phase I to III. The success rate of these trials and the posterior application of AMPs as therapeutic agents is variable as, while there are currently several AMPs approved for clinical use, such as ghrelin, nisin, gramicidin or daptomycin, there are others, such as CZEN-002 or NVB-302, which have been discontinued as they failed in their clinical trials
[56][57][58][59][106,107,108,109]. The causes for these failures are usually unknown and unexpected as all AMPs are validated by various in vitro, in silico and in vivo models before reaching this stage
[58][108]. One example of such failures is the Friulimicin AMP, which was terminated due to unfavorable kinetics in healthy volunteers and another is the Murepavadin AMP as, in a stage III trial of patients with nosocomial pneumonia, it caused higher than expected kidney injuries
[58][108].
Table 2.
Examples of AMPs which underwent and are undergoing clinical trials.
a—Discontinued; b—Ongoing; c—Completed; d—Unknown; n.a.—not applicable.
Of the examples presented in
Table 2, it is interesting to see that only Omiganan targets AD-related factors directly. In fact, a cursory analysis of the table shows that most AMPs target bacterial growth, a clear reflection of their namesake, and which has directed research efforts over the past years. When one considers this, the scope for AD-related applications grows immensely as various AMPs in clinical trials target AD-critical aspects, such as bacterial skin infection and, more particularly,
Staphylococcal growth.