Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Rhea Nugraha and Version 2 by Wendy Huang.
Volumetric absorptive microsampling (VAMS) is the newest and most promising sample-collection technique for quantitatively analyzing drugs, especially for routine therapeutic drug monitoring (TDM) and pharmacokinetic studies. This technique uses an absorbent white tip to absorb a fixed volume of a sample (10–50 µL) within a few seconds (2–4 s), is more flexible, practical, and more straightforward to be applied in the field, and is probably more cost-effective than conventional venous sampling (CVS).
- volumetric absorptive microsampling (VAMS)
- conventional venous sampling (CVS)
- therapeutic drug monitoring
- pharmacokinetic studies
- drug concentration
1. Introduction
The essential goal of clinical pharmacology is to understand the dose–concentration–effect relationship. The study of pharmacokinetics seeks to explain the time course of drug concentrations in the body (dose–concentration relationship). However, the time course of drug concentrations cannot predict the magnitude of the drug effect (concentration–effect relationship) [1][2][1,2]. This dose–concentration–effect relationship is now used as the central concept of therapeutic drug monitoring (TDM), which individualizes drug dosage by attaining specific target plasma concentrations (therapeutic ranges) guided by the measurement of plasma drug concentrations [3]. TDM is used for assessing efficacy, diagnosing undertreatment, preventing adverse effects, guidance to stop the treatment, monitoring and detecting drug interaction, and monitoring adherence [4]. It is recommended for drugs with a narrow therapeutic range, significant pharmacokinetic variability, and a clear relationship between drug concentrations and clinical response [5].
The sampling technique commonly used to routinely measure drug concentration, either for TDM or pharmacokinetic studies, is conventional venous sampling (CVS), which draws blood from the vein. CVS can lead to unexpected complications, such as hematoma and thrombophlebitis [6][7][6,7]. This technique requires much blood for each sample (up to 5 mL), is invasive and inconvenient, has a relatively high cost, sometimes needs special conditions (a cold chain) for transport, and samples must be centrifuged before storage as plasma or serum. If the sample is not immediately analyzed, it must be frozen at −20 up to −80 °C. These characteristics cause CVS to be less flexible for application in the field [8][9][10][8,9,10]. An advantage of CVS is that the sample volume is large, while analysis only needs a small volume; therefore, the leftover sample could be stored and re-analyzed [6][7][6,7].
Considering the many limitations of CVS, which can complicate TDM programs or pharmacokinetic studies, there have been many innovations in sampling techniques for drug concentration measurement in the past decade, called microsampling techniques. Microsampling is a sampling technique that only takes a small volume of samples (<100 µL for blood) from the body for analysis; it is less invasive, less painful, and more efficient. This technique is also more practical compared to CVS [11]. Therefore, this technique may improve routine clinical care in TDM and benefit pharmacokinetic studies, including those with children as subjects. Some microsampling techniques that have already been developed are capillary microsampling (CMS), dried blood spots (DBS), dried plasma spots (DPS), plasma preparation technologies, solid-phase microextraction (SPME), and volumetric absorptive microsampling (VAMS) [12]. VAMS and DBS have been the most researched to analyze drugs [12][13][14][15][16][17][12,13,14,15,16,17]. Previously, the most commonly used and straightforward microsampling design was DBS, which requires small volume sizes (30 µL per spot). But DBS has some limitations primarily related to the effect of hematocrit values that may affect measured concentrations. The VAMS technique was then developed to tide over the boundaries of DBS [12][18][19][12,18,19]. VAMS is a promising sample-collection technique for the quantitative analysis of drugs, which only takes a 10–50 µL volume of samples by an absorbent tip [20][21][20,21]. Compared to CVS, the VAMS technique has some superiority in practicality and flexibility of the sampling process because it only needs a small sample volume. The sampling process is relatively fast and less invasive and there is no need to freeze the sample before transport; thus, it may be more cost-effective, there is no need for centrifugation before storage, and it also reduces the amount of freezers needed to keep samples in the long term [18][19][22][18,19,22]. Therefore, this VAMS technique is more flexible for application in the field than CVS and can be innovative for sampling processes that are more practical and simpler [18][22][18,22].
2. Sampling Procedure with VAMS
VAMS is the newest innovation in microsampling techniques. VAMS was designed to absorb a minimal and fixed volume, such as 10, 20, and 50 µL. VAMS devices contain a white hydrophilic pore absorbent tip attached to a plastic handler [19]. The picture of the VAMS device is shown in Figure 1, which comes with two different types of devices, namely clamshells and cartridges. The sampling procedure with VAMS is simple: dipping the tip of VAMS in the location that has been punctured using a lancet at a 45° angle for 2–4 s until the tip is entirely red. The sample for this device is not only blood; VAMS has also been used to collect urine, saliva, or other liquid biological samples [18][19][18,19]. After obtaining the sample, the devices are dried at room temperature for at least 2 h. The samples can be transferred at room temperature for storage or analysis [19][23][19,26]. The drying of the devices could correlate with the limitation of VAMS itself. Care is also taken to ensure that the tips do not touch either other tips or their surroundings to prevent blood transfer during drying. If it touches others, it could be contaminated. Also, the variation in drying times could be an issue with reproducible recovery. Drug extraction is more inconvenient when samples become drier. Understanding the effect of drying on VAMS samples is essential for method development and validation. The total time for drying depends on the size of the absorbent tip on the VAMS devices. It has been known that 1 h of drying at room temperature is adequate when using 10 µL VAMS. Furthermore, the drying time also could generate the degradation of the sample; thus, the stability of analytics in drying time needs to be evaluated [18][24][18,27].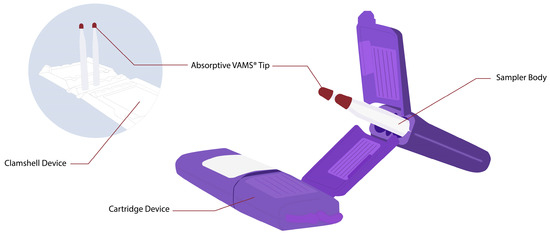
Figure 1.
Volumetric absorptive microsampling devices (
left
picture is VAMS in clamshell device;
right
picture is VAMS in cartridge device).