The immunomodulatory property of curcumin results from its interaction with various immune mediators, including B and T lymphocytes, macrophage and dendritic cells, cytokines, and various transcription factors such as nuclear factor kappa B (NF-κB), activator protein-1 (AP-1), and signal transducer and activator of transcription (STAT)
[68][69][70][71][72][73][168,169,170,171,172,173]. It has been found that curcumin can inhibit the maturation and function of dendritic cells. This function of curcumin is achieved through reducing the expression of MHC-II and co-stimulatory molecules such as CD11c, CD40, CD54, CD80, CD83, CD86, CD252, and CD256. It can also be due to the reduction of proinflammatory cytokines such as IL-1, IL-6, IL-12, IL-12p40, IL-12p70, and TNF-α. In general, curcumin can keep dendritic cells in an immature state, and as a result, it suppresses dendritic cell-mediated stimulation of inflammatory T cells, which play a key role in the severity of symptoms observed in SLE
[63][21].
3.5. Emodin
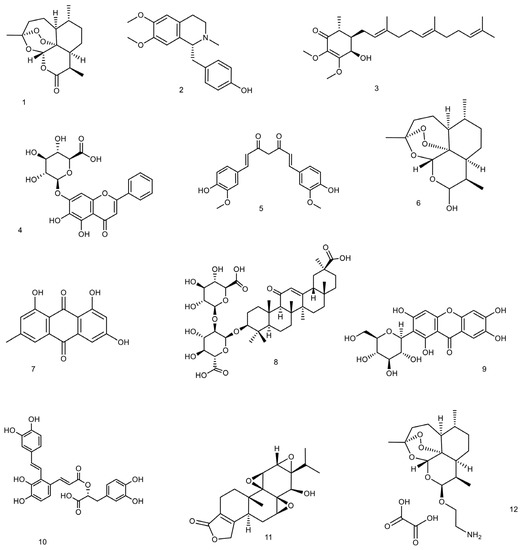
Emodin (1,3,8-trihydroxy-6-methylanthraquinone) is actually a natural anthraquinone that can be found in the barks and roots of many plants, lichens, and molds
[74][177]. One of the main sources of emodin is
Rheum palmatum (Polygonaceae) which is also known as Chinese rhubarb.
Emodin can reduce steroid resistance by inhibiting P-glycoprotein efflux function. Steroid therapy is part of the common treatment for SLE patients, and a decreased response to steroid therapy following overexpression of p-glycoprotein in peripheral lymphocytes has been observed in some patients
[75][178].
An attempt was made to investigate the effect of emodin on nephritis in a study on BXSB lupus mice. Mice were treated with different doses of emodin for 30 days. As a result, it has been shown that following emodin consumption, the level of proteinuria is reduced and the expression of intercellular adhesion molecule-1 (ICAM 1) in the renal glomerulus is also reduced
[76][107].
The effect of emodin on renal injury in lupus nephritis was investigated. Lupus-prone male BXSB mice were treated with 0, 5, 10, and 20 mg/kg/day emodin for 30 days. Finally, it was observed that following the administration of emodin, glomerular levels of TNF-α, ICAM-1, and fibronectin (FN) decreased, and the levels of urinary protein and serum anti-dsDNA antibody also decreased, and these decreases were dose-dependent. The mechanism of action of emodin is probably through inhibition of dsDNA antibody and decreased levels of TNF-α, ICAM-1, and FN in the glomeruli
[77][108].
Toxicity and Side Effects
According to reports, emodin can reduce sperm motility in a dose-dependent manner in mice. Emodin has also been found to have dose- and time-dependent toxicity in kidney and liver cell lines. Intestinal discomfort and severe diarrhea brought on by an overdose of emodin due to its laxative properties lead to an electrolyte imbalance and dehydration
[78][179]. Generally, it is also known to have kidney toxicity, hepatotoxicity, and reproductive toxicity, especially at high doses and long-term use
[79][180] The extremely low bioavailability of emodin further limits its use in therapeutic applications
[78][179].
3.6. Esculetin
Esculetin (also known as aesculetin, 6,7-dihydroxycoumarin, and cichorigenin) is a coumarin that has been isolated from a variety of medicinal and toxic plants such as
Cichorium intybus (chicory) and in
Hydrangea paniculate Siebold. In a study conducted on MRL/lpr mice, esculetin significantly attenuated renal impairment by reducing BUN, serum creatinine, and albuminuria. Esculetin could improve glomerular hypertrophy and tubular interstitial fibrosis and reduce mononuclear cell infiltration into the interstitium. It was suggested that this molecule could significantly down-regulate the complement cascade as well as the inflammation and fibrosis pathway. In addition, esculetin could up-regulate Nrf2-related antioxidation genes. The authors reported that esculetin could inhibit complement activation both in classical and alternative pathways. The molecule blocked the C3 convertase (C4b2a) to exert this inhibitory capability. Moreover, it was suggested that the antioxidation effect of esculetin was dependent on Nrf2 activation, which means that esculetin could inhibit NFκB nuclear translocation and TGFβ-smad3 profibrosis pathway
[80][109]. Lupus nephritis is one of the important complications of lupus, and complement activation contributes to kidney injury; the inhibition of complement activation by herbal compounds might be beneficial for lupus. It was also reported that the coumarin derivates that are isolated from
H. paniculata could improve renal injuries in cationized-BSA-induced membranous nephropathy. The suggested mechanism was the inhibition of complement activation and interleukin 10-mediated interstitial fibrosis
[81][181].
Toxicity and Side Effects of Esculetin
Acute toxicity studies reported LD
50 for intraperitoneal injection to mice as 1450 mg/kg and >2000 mg/kg by mouth. No reported adverse effects are known other than LD
50 [82][182].
3.7. Mangiferin
The main source of mangiferin is
Mangifera indica, although it is found in 96 species, 28 genera, and 19 families of angiospermic plants.
Mangifera indica belongs to the family Anacardiaceae and is known as mango. Almost all parts of
M. indica, such as fruits, twigs, leaves, and stem bark, contain mangiferin
[83][183]. Mangiferin is a xanthonoid polyphenol with a variety of pharmacological effects such as anti-inflammatory, antioxidant, immunomodulatory, nephroprotective, hepatoprotective, anti-cancer, anti-diabetic, and anti-asthma
[84][184]. According to certain research, its renal protective actions may be beneficial for those with lupus nephritis
[66][67][166,167].
Mangiferin has been shown to improve lupus nephritis in lupus-prone B6/gld mice. In a study, the effect of mangiferin on lupus nephritis was investigated. Mice were treated orally with 20 or 40 mg/kg/day of mangiferin for 12 weeks. Finally, Mangiferin has been shown to be effective in treating lupus nephritis with its anti-inflammatory and immunomodulatory effects. Mangiferin was effective by suppressing mTOR signaling pathways, upregulating CD4
+ FoxP3
+ Tregs, and inhibiting T cell proliferation. Mangiferin improved renal immunopathology and reduced renal T cell infiltration. It also lowered serum creatinine and urinary protein levels and increased CD4
+ FoxP3
+ Treg frequencies in the spleens, lymph nodes, and kidneys
[85][113].
Toxicity and Side Effects
Mangiferin is typically regarded as a non-toxic natural substance. Adults receiving 0.9 g of mangiferin orally demonstrated no toxicity. LD
50 of the mangiferin was considered to be 400 mg/kg on mice
[86][185]. Mangiferin was found to be safe and helpful in enhancing cellular function, according to numerous research works
[87][186]. In a study that assessed the toxicity of mango leaf extract, which was given orally to rats for three months at a dose of 2 g/kg body weight per day, neither mortality nor toxic effects were observed
[88][187]. The
Mangifera indica leaf aqueous extract was not particularly mutagenic or genotoxic. Mangiferin has generally been shown to be safe in cell and animal research. In contrast, there are insufficient safety data from human research
[87][186].
3.8. Salvianolic Acid A
Salvianolic acid A (or Dan phenolic acid A) is a phenolic compound extracted from
Salvia miltiorrhiza (Lamiaceae family). The plant is also known as Chinese sage, Danshen, and red sage. Salvia species such as
S. officinalis and
S. miltiorrhiza have shown antioxidant, antibacterial, anti-cancer, and anti-diarrheal effects and have been used to treat lupus and autism, lower cholesterol, treat Alzheimer’s, reduce sweating, and reduce menopausal hot flashes
[89][188].
In a study performed on BALB/c mice, the effect of salvianolic acid A isolated from the root of
S. miltiorrhiza, on lupus nephritis was investigated. Mice were treated with 5 mg/kg/day of salvianolic acid A for 5 months. As a result, it was observed that following the consumption of salvianolic acid A, anti-Sm autoantibodies decreased, phosphorylation of IKK, IκB, and NFκB in kidney tissue was inhibited, and pathological effects were reduced
[90][114].
Toxicity and Side Effects
In an acute toxicity study, the LD
50 of salvianolic acid A was reported as 1161.2 mg/kg in mice. In dogs’ animal model, the minimum lethal dose and maximal non-lethal dose of salvianolic acid A were reported as 682 mg/kg and 455 mg/kg in dogs, respectively. Based on a 4-week repeated-dose, no observed adverse effect level was 20 mg/kg. It was suggested to examine liver and kidney function during the administration of salvianolic acid A in a clinic
[91][189]. According to a system review of the drug’s safety, the clinical use of salvianolate injection did not result in the occurrence of any common or major side effects. Blood loss and allergic reactions are the most common adverse effects of salvianolic acid injections. In general, it has been determined that salvianolic acid is well tolerated in the general population. Rash, erythemas, pruritus, palpitations, headaches, dizziness, elevated blood bilirubin, elevated transaminases, elevated blood creatinine, positive fecal occult blood, and abnormal platelet count are among the most common adverse effects that were reported for salvianolic acids
[92][190].
3.9. Triptolide
Triptolide is a diterpene triepoxide isolated from
Tripterygium wilfordii Hook F (
T. wilfordii). The molecule has immunosuppressive and anti-inflammatory effects and has been shown to have therapeutic effects on autoimmune and inflammatory diseases such as lupus nephritis, arthritis, neurodegenerative disorders, and asthma
[33][93][23,139]. Despite the beneficial effects of Triptolide in the treatment of various inflammatory disorders, it should be noted that the use of
T. wilfordii can cause severe toxicity and side effects. This may limit the clinical use of this plant
[94][191]. Triptolide’s anti-inflammatory and immunosuppressive effects are due to its ability to inhibit the proliferation of immune cells and inflammation-related cells and reduce cytokines and proinflammatory mediators
[95][192].
The effects of triptolide on SLE are assumed to be through induction of miR-125a-5p and an increase in the proportion of Treg
[96][124]. Triptolide has been shown to reduce the expression of transforming growth factor-beta (TGF-β) and vascular cell adhesion molecule (VCAM-1)
[97][193]. It can also reduce the expression of C3 and CD40, so it generally has immunosuppressive and anti-inflammatory effects and is useful in renal disorders
[98][194]. Another way triptolide can be immunosuppressive and anti-inflammatory is through changing signaling pathways. Triptolide has been reported to inhibit nuclear factor-κB (NF-κB) signaling pathway
[99][195], lower the IL-17 level, and suppress IL-6/signal transducer and transcription 3 (STAT3) signaling pathway
[100][196].
(5R)-5-Hydroxytriptolide (LLDT-8) is a triptolide analogue. It has strong anti-inflammatory and immunosuppressive activity
[100][196]. LLDT-8 improves anti-GBM glomerulonephritis because it can regulate Fcγ signaling pathway
[101][197]. It can also improve lupus nephritis and reduce the infiltration of kidney immune cells because it inhibits the expression of renal chemokines
[102][125].
Toxicity and Side Effects
The subject of triptolide‘s safety in clinical applications has been brought up because of its broad usage. Despite the valuable pharmacological effects of triptolide, its application requires particular caution because it is well known to have hepatotoxicity, nephrotoxicity, reproductive toxicity, etc.
[103][198]. Hepatic cytochrome P450s are involved in the metabolism of triptolide, and triptolide toxicity and CPY3A also have a close relationship. Clinical case reports have shown through research that triptolide exposure can be involved in damaging a variety of organs, including the kidney, liver, heart, ovary, and testicles. Additionally, it has been shown that triptolide has a variety of harmful effects on cells, including damage to membranes, oxidative stress, endoplasmic reticulum stress, metabolism dysfunction, mitochondrial dysfunction, apoptosis, and autophagy
[104][199].
3.10. Total Glycosides of Paeony (TGP)
Total glycosides of paeony (TGP) are extracted from the root of
Paeonia lactiflora. TGP has long been used to treat autoimmune diseases
[105][200]. The beneficial effects of TGP on lupus patients are dependent on its anti-inflammatory and immunosuppressive effects
[106][201]. The effects of TGP on the production of proinflammatory cytokines, antibody production, apoptosis of lymphocytes, and lymphocyte proliferation are dual and dose-dependent
[107][202]. TGP increased the mouse splenocytes’ proliferation at low doses (0.05~0.4 mg/L), while it decreased it at high doses (0.4~1.6 mg/L)
[107][108][109][202,203,204]. The ratio of T helper cells to T suppressor cells (Th/Ts) increases at low doses of TGP (0.2 mg/L) and decreases at high doses of TGP (6.0 mg/L)
[109][204]. IL-1 production increases at low doses of TGP (0.5~12.5 mg/L) and decreases at high doses of TGP (12.5~312.5 mg/L)
[108][203]. IgM-antibody production increases at low doses of TGP (0.1~0.4 mg/L) and decreases at high doses of TGP (0.4~3.2 mg/L)
[110][111][205,206]. Therefore, it is assumed that the immunomodulatory effects of TGP are dose-dependent, and the dose should be adjusted for best results.
The beneficial effect of TGP on SLE has been discussed in several studies. It was reported that the anti-inflammatory effect of TGP is due to its ability to inhibit the production of nitric oxide, leukotriene B4, and prostaglandin E2
[107][202]. TGP reduces the SLEDAI score in SLE patients and also reduces the average daily dose of prednisolone
[112][115]. A decrease in renal pathology has been observed following the consumption of TGP by MRL/lpr mice. TGP has also reduced the levels of anti-dsDNA antibodies and antinuclear antibodies (ANA). It could also reduce urinary protein levels. Consequently, it was concluded that TGP consumption in patients with lupus nephritis can have therapeutic effects
[113][119]. TGP causes down-regulated Foxp3 promoter methylation levels, thus increasing the expression of Foxp3 in lupus CD4
+ T cells. TGP increased the number and percentage of Treg cells in lupus CD4
+ T cells and increased IFN-γ and IL-2 expression
[105][200]. TGP increases DNA methylation of ITGAL promoter in CD4
+ T cells, thereby reducing CD11a gene expression
[114][120].
Toxicity and Side Effects
In general, TGP is considered a safe and effective compound that is tolerable and does not cause any serious side effects. According to studies, the likelihood of developing diarrhea after consuming TGP may rise. TGP can accelerate the gastrointestinal tract’s peristalsis, which may be the cause of the diarrhea. The majority of patients only experience moderate and acceptable symptoms, and the gastrointestinal system is not organically harmed. Drowsiness, dry mouth, dizziness, and weakness are some additional side effects that have been reported
[115][207].
4. Fatty Acids, Vitamins, and Minerals
Certain nutrients and vitamins as dietary supplements have been consumed to improve lupus
[116][208]. The efficacy of some of them have been investigated and discussed in several studies
(Table 2). Safety and side effects of fatty acids, vitamins, and minerals is well studied by numerous publications and are available even on the indications of these over-the-counter (OTC) medicines.
4.1. Fatty Acids
Unsaturated oils play an important role in the immune system regulation. In human nutrition and/or healthcare, seed oils have long been utilized as a daily supplement, a food ingredient, or a therapeutic cure. Long chain fatty acids (LCFAs) are fatty acids with more than 14 carbons and make up the majority of vegetable oils. They are necessary for the human body’s ongoing regular cell growth and development. Among these, polyunsaturated fatty acids (PUFA) like n-3 and n-6 fatty acids are crucial for the prevention and treatment of many chronic diseases, including diabetes, coronary artery disease, inflammatory and autoimmune disorders, and many other ailments. Some significant fatty acids, such as linoleic acid (an n-6 fatty acid) found in the majority of vegetable oils and plant seeds, are regarded as essential fatty acids (EFAs). Arachidonic acid, which can be further elongated and desaturated to form prostaglandins, thromboxanes, and leukotrienes, is one of these EFAs. A different class of EFA is the n-3 fatty acids, which include linolenic acid and are present in soy, linseed, and flaxseed oils. According to some evidence, n-3 fatty acids have protective effects on eicosanoid metabolism. Docosahexaenoic acid (DHA), a crucial component of cellular membranes and another significant n-3 fatty acid, has a favorable impact on coronary heart disease, inflammatory disease, atherosclerosis, and disorders of the nervous system
[117][209]. Dietary lipids are also involved in autoimmune phenomena by affecting the balance between Th1 and Th2 cells
[118][119][210,211].
Dysregulation of PUFAs induces a wide range of neurological and developmental disorders. Linoleic acid and linolenic acid are required as part of the immune cell membrane
[120][212]. α-linolenic acid and γ-linolenic acid are among the omega-3 acids that have beneficial effects following the reduction of TNF-α and IL-2 in SLE patients. Omega-3 fatty acid supplementation has shown potential benefit on SLE disease activity as demonstrated by Systemic Lupus Activity Measure-Revised (SLAM-R), SLE Disease Activity Index (SLEDAI), and British Isles Lupus Assessment Group (BILAG) scores as well as plasma membrane arachidonic acid composition and urinary 8-isoprostane levels, with minimal adverse effects
[121][213].
Finding the optimal ratio of ω-6/ω-3 PUFAs is essential in therapeutic interventions. As an example, linoleic/alpha-linolenic of 1:3 is the optimal ratio for enhancing both the proliferation and differentiation of cells such as neural stem cells
[122][214]. Wei et al. concluded in a meta-analysis that low-ratio n-6/n-3 PUFA supplementation could significantly reduce serum TNF-α and IL-6 concentrations but not CRP concentrations
[123][215].
In the NZB × NZW mice animal models, essential fatty acid deficient diets can reduce arachidonic acid levels, thus reducing proinflammatory prostaglandins and leukotrienes, and also reduce nephritis by inhibiting autoantibody production
[120][212]. Studies have shown that the lifespan increased and autoantibody levels decreased in animal models of SLE following a diet rich in omega-3 fatty acids
[124][22].
The presence of omega-3 PUFA in the diet of SLE patients can regulate blood pressure and proteinuria and also reduce anti-dsDNA levels, as well as TNF-α, IL-1α, IL-1β, and IL-2
[121][125][126,213].
A meta-analysis conducted in 2020 found that omega-3 fatty acids could reduce SLE activity. In this study, 136 patients in the comparison group and 138 in the treatment group were used, and the mean age of patients was 43 years. The follow-up time of the trial varied between 12 and 52 weeks. This study showed that the use of omega-3 fatty acids is more effective than placebo in reducing disease activity in SLE
[124][22].
Eicosapentaenoic (EPA) and docosahexaenoic (DHA) are some of the unsaturated fatty acids that exert their anti-inflammatory effects by lowering the level of C reactive protein (CRP) and other inflammatory mediators
[125][126][127][126,216,217]. The most widely available dietary source of EPA and DHA is cold-water oily fish, such as salmon, herring, mackerel, anchovies, and sardines.
EPA and DHA can affect the immune system through various mechanisms. They can inhibit the enzyme lipoxygenase and subsequently reduce the inflammatory factors derived from arachidonic acid. DHA can inhibit nuclear factor κB (NF-κB) and TNF-α
[128][218].
DHA has increased the lifespan of and suppressed glomerulonephritis in NZB × NZW mice with systemic lupus erythematosus, possibly due to inhibition of IL-18 induction
[125][126]. DHA has also reduced IL-18 levels, lowered serum levels of anti-dsDNA, and regulated IgG renal deposition in mice
[125][129][126,219].
4.2. Vitamin A
Some studies have been conducted to investigate the effectiveness of vitamin A in lupus. Retinoic acid is a metabolite of vitamin A. Vitamin A deficiency in lupus patients has been shown to have a negative effect on the prognosis of the disease. Consumption of retinoic acid and vitamin A regulates the balance between Th17 and Treg. It was reported that following the intake of vitamin A by lupus patients, the level of Th17 decreased and the level of Treg increased
[130][131][127,128].
4.3. Vitamin B
Vitamins B6, B12, and folate reduce homocysteine levels, so they can be helpful in improving atherosclerosis in SLE patients. They can also lower levels of inflammatory cytokines and C-reactive protein (CRP). Vitamin B6 can also reduce the risk of active disease by lowering homocysteine
[132][129]. Following the use of niacin, a decrease in triglyceride and LDL-C levels was observed, with no significant effect on HDL-C levels
[133][130]. In general, it was suggested that taking supplements of the vitamin B complex could be beneficial for people with SLE.
4.4. Vitamin C
Vitamin C has an antioxidant effect. It can release inflammatory mediators and modulate immune function. It also lowers anti-dsDNA levels and IgG. Vitamin C can prevent active SLE
[134][131]. Concomitant use of 500 mg of vitamin C and 800 mg of vitamin E daily for 3 months has shown a slight decrease in lipid peroxidation. In SLE patients with high doses of vitamin C, ascorbate is found in the urine, so the maximum dose of vitamin C is 1000 mg/day
[135][220].
4.5. Vitamin D
It has been shown that there is a link between vitamin D deficiency and the severity of SLE. Higher SLEDAI scores have been reported in patients with low levels of vitamin D. Supplementation with vitamin D in SLE patients inhibits dendritic cell activation and maturation
[136][132]. Calcitriol is the active form of vitamin D and acts on autoimmune diseases such as SLE by regulating the response of T and B cells and boosting the innate immune response
[137][133]. SLE patients are photosensitive and should use sunscreen when exposed to the sun. On the other hand, sunlight is needed to produce vitamin D, so it can be assumed that taking vitamin D supplements might be useful for SLE patients
[138][139][221,222].
4.6. Vitamin E
Vitamin E has antioxidant and anti-inflammatory effects and, because of its anti-inflammatory effect, seeks to reduce IL-2, IL-4, and TNF-α, which can be effective in lupus
[140][223]. Furthermore, vitamin E consumption by SLE patients reduces the generation of autoantibodies
[141][134].
4.7. Calcium
In some SLE patients, a decrease in bone mineral density has been observed, which may or may not be dependent on corticosteroid use. On the other hand, these patients are mostly deficient in vitamin D and avoid exposure to sunlight. Therefore, adequate calcium intake is important for SLE patients
[140][223].
4.8. Iron
There should be a balance of iron intake in SLE patients. Iron supplementation to MRL/MPJ-lpr/lpr mice resulted in cell damage, renal lesions, and worsened renal impairment in an in vivo study. Iron chelators have also been shown to be beneficial in autoimmune diseases. In contrast, iron deficiency increases the symptoms of the disease, so iron should be used in SLE patients who have anemia
[142][143][135,224].
4.9. Selenium
Selenium supplementation has been considered in the treatment of lupus because of its antioxidant and anti-inflammatory effects. A study on NZB/NZW female mice found that survival increased following selenium supplementation, which may be due to increased levels of natural killer cell activity
[144][136]. In an in vitro study performed on the B6.Sle1b mouse model of lupus, an attempt was made to find the mechanism of the effect of selenium on lupus. It has been shown that selenium can inhibit the activation, differentiation, and maturation of macrophages and B cells. Therefore, its use can be useful in patients with lupus
[145][137]. Reduced selenium levels have been observed in patients with autoimmune diseases, which may be considered a risk factor for the onset of autoimmunity and inflammation. Due to the anti-inflammatory effect of selenium, it has been suggested that consuming a certain amount of selenium in patients with autoimmune diseases can lead to better management of disease complications
[146][225].
4.10. Zinc
It was shown that a zinc-restricted diet can increase serum levels of corticosteroids and subsequently reduce the symptoms of autoimmune diseases such as SLE, so it can be useful in controlling SLE
[147][226]. A study of NZB/NZW mice showed a decrease in autoantibody production. In MRL/lpr mice, the use of zinc-restricted diets decreased the level of anti-dsDNA, decreased lymphoproliferation, and recovered glomerulonephritis
[118][210]. On the other hand, it should be noted that a study conducted on humans has shown that zinc deficiency causes immune dysfunction by acting on Th cells and can lead to neurosensory disorders and reduced body mass
[148][227].
5. Herbal Medicines, Medicinal Plants, Mushrooms, and Fungi and Their Crude Extracts
A variety of medicinal plants and mushrooms have been reported to exhibit efficacy against lupus conditions. In some traditional remedies, they have been used in the form of dried powdered plant material or fungi. In some others, a crude extract of the plant or fungus was prepared using solvents such as water or ethanol or a mixture of both (hydroalcoholic extract). Crude extracts are a complex mixture of molecules with the same range of polarity but different concentrations. Sometimes, several molecules with a variety of mechanisms work synergistically to produce a specific effect. Although the crude extracts of herbal medicine can reflect the efficacy of a special herb or fungi, due to the variation of compounds in the natural sources, special attention should be given to the standardization and authentication of them in order to have repeatable and reliable effects. Compared to purified bioactive molecules, crude extracts usually exhibit milder efficacy and side effects, and introducing supplements from herbal medicine to the market is much easier.