Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Rocco Antonio Montone and Version 2 by Camila Xu.
Myocardial bridging (MB) is the most frequent congenital coronary anomaly characterized by a segment of an epicardial coronary artery that passes through the myocardium. MB is an important cause of myocardial ischemia and is also emerging as a possible cause of myocardial infarction with non-obstructed coronary arteries (MINOCA). There are multiple mechanisms underlying MINOCA in patients with MB (i.e., MB-mediated increased risk of epicardial or microvascular coronary spasm, atherosclerotic plaque disruption and spontaneous coronary artery dissection).
- MINOCA
- myocardial bridge
- pathogenesis
- diagnosis
- management
1. Introduction
Myocardial infarction with non-obstructed coronary arteries (MINOCA) is defined as the clinical evidence of acute myocardial infarction (MI) with normal or near-normal coronary arteries at coronary angiography (i.e., <50% diameter stenosis in any major epicardial vessel) after excluding systemic non-coronary causes of chest pain and troponin elevation, such as severe anaemia or pulmonary embolism [1][2][1,2]. MINOCA may account for up to 10% of patients presenting with acute MI, and, although it was initially considered a benign condition, accumulating evidence has demonstrated that MINOCA patients have worse cardiovascular (CV) outcomes compared with the general population [3][4][5][3,4,5]. Indeed, MINOCA patients have a 1-year mortality and a rehospitalization rate only slightly lower than that of those with acute MI due to obstructive coronary artery disease (CAD) [6]. Furthermore, up to 25% of MINOCA patients might experience angina in the 12 months following the acute event, which has a significant impact on patients’ quality of life and healthcare-related costs [7].
Myocardial bridging (MB) is a congenital coronary anomaly, in which a segment of an epicardial coronary artery, most frequently the left anterior descending artery, deviates its canonical epicardial course by passing through the myocardium [8]. The reported prevalence of MB varies widely according to the different diagnostic tools, ranging from 2–6% at coronary angiography to 19–22% at coronary computed tomography angiography (CCTA) [9][10][11][9,10,11]. Notably, in patients presenting with MINOCA, the prevalence of MB may be as high as 20–40% [12][13][14][12,13,14]. Recent evidence has demonstrated that MB, alone or in combination with other superimposed pathogenetic mechanisms, is a frequent yet commonly overlooked cause of MINOCA [13]. Moreover, the identification of MB and of the pathogenetic mechanism underlying MINOCA may have important therapeutic implications [14].
2. Pathophysiology of MB and Its Association with MINOCA
The main feature associated with MB is a dynamic compression of the tunnelled artery during the systole. As coronary blood flow occurs primarily during diastole, only a small percentage (≃15%) of coronary blood flow should theoretically be compromised by the presence of a bridge; accordingly, MB has been long considered a benign condition. However, recent evidence has demonstrated that MB could lead to clinically evident myocardial ischemia through different mechanisms, including the interplay between a high sympathetic tone and a delayed early diastolic coronary artery relaxation [15], the occurrence of a Venturi-like effect along the bridged artery [16], an MB-mediated increased risk of epicardial or microvascular coronary spasm [13][17][13,17], atherosclerotic plaque disruption (i.e., plaque rupture or plaque erosion) [18], spontaneous coronary artery dissection (SCAD) [19] or their combination. Each of these mechanisms associated with MB may potentially be the underlying aetiology of MINOCA. The presence of MB is associated with a delayed early diastolic coronary artery relaxation within the intramyocardial segment and a hindered rapid early diastolic hyperaemia, leading to a reduced coronary blood flow. This mechanism may be particularly relevant in the sub-endocardium, as it is more susceptible to ischemia, and it may be accentuated by an increased sympathetic tone [20][21][20,21]. Indeed, the latter increases the heart rate, decreases the diastolic perfusion time, increases the strength of contraction across the MB and delays the relaxation beyond systole into the early diastolic phase, thus impairing coronary blood flow. Moreover, the presence of MB is associated with the occurrence of a Venturi-like effect at the ostium of the side branches, in particular the septal branches, also known as “branch steal”. Indeed, flowing through the tunnelled artery in the end systole/early diastole, the blood passes through a constricted segment leading to an increase in fluid velocity and a decrease in the perfusion pressure at the ostium of the side branches [16]. The key aspects for the risk of myocardial ischemia associated with MB are the depth and the length of the tunnelled segment. Indeed, the depth of MB (<2 mm superficial, ≥2 mm deep, ≥5 very deep) is one of the main determinants of the degree of systolic compression and course of the affected artery. The length of MB is related not only to the amount of affected arteries but also to the number of side branches affected [8]. Of importance is the fact that, as demonstrated by a recent study from researchers' group enrolling patients with myocardial ischemia and non-obstructive coronary arteries undergoing intracoronary provocative testing with acetylcholine (ACh), the prevalence of epicardial or microvascular coronary vasospasm is high among patients with MB (up to 79%, mainly epicardial spasm rather than microvascular spasm). Moreover, coronary spasm coexists more frequently in patients with MINOCA than in stable patients with no obstructive CAD (21.3% vs. 7%, p = 0.002). Of note is the fact that the presence of MB was a predictor of MINOCA only in patients with a positive ACh test, and patients with MB and a positive ACh test had a lower major adverse cardiac-event-free survival, representing the group with the worst prognosis [14]. Another study by Nam et al. demonstrated that severe MB (defined as bridge narrowing >90%) was significantly associated with a high risk of coronary spasm, and patients with both conditions were more likely to have recurrent angina compared with MB patients without spasm [17]. Epicardial coronary vasospasm is defined as the vasoconstriction of an epicardial coronary artery caused by vascular smooth muscle hyper-reactivity due to increased sympathetic stimulation, local or systemic inflammation or environmental factors (i.e., smoking, alcohol consumption, environmental exposures) [22]. Microvascular spasm results from an increased constriction of coronary microvessels due to a reduced production and/or enhanced degradation of nitric oxide and other endothelial-derived relaxation factors [23][24][23,24]. Mechanistically, the compression–relaxation effect of MB on the coronary arteries may result in injury to the intima and endothelium, leading to impaired endothelium-dependent vasodilatation and enhanced local vascular reactivity to systemic vasoconstrictor stimuli [25]. Moreover, a reduced expression of endothelial nitric oxide synthase has been demonstrated in the MB segment compared to the proximal and distal segments [26]. These alterations also involve coronary microcirculation, as the presence of MB has been associated with alterations in vasoactive agents such as nitric oxide synthase and endothelin-1 and local variations in shear stress [27]. The anatomical features of MB, such as the length and percentage of systolic compression, may further promote the occurrence of coronary vasospasm [28][29][28,29]. Importantly, the presence of MB might favour the progression and destabilization of atherosclerotic plaques in the segment proximal to the tunnelled one [18]. Plaque rupture is caused by a fibrous cap discontinuity, which exposes the plaque core to the coronary lumen, leading to the activation of a pro-thrombotic cascade and a consequent thrombus formation [30][31][30,31]. Plaque erosion is due to the apoptosis of endothelial cells leading to thrombus formation without fibrous cap discontinuity [31][32][31,32]. Both plaque rupture and plaque erosion may not determine an angiographically evident flow-limiting stenosis and present as MINOCA through different mechanisms, including a transient thrombosis with spontaneous thrombolysis, distal embolization, superimposed vasospasm or a combination of these processes [33]. In patients with MB, the longstanding compression–relaxation effect of the intramural segment can cause changes in the wall shear stress, leading to the formation of an area of reduced wall shear stress proximal to the MB and the release of inflammatory mediators and endothelial vasoactive agents [25]. Conversely, the wall shear stress is increased along the tunnelled artery, thus sparing this segment from atherosclerosis. Another mechanism that could promote atherosclerotic plaque formation and progression in the segment proximal to the MB is the abnormal blood flow profiles in this area caused by the collision of anterograde coronary flow with the retrograde flow due to the compression of the MB during the systole. Such alterations can determine endothelial injury, thus promoting plaque formation and disruption [34]. The presence of MB might increase the risk of SCAD, a frequently overlooked cause of MINOCA, especially in young women. SCAD is caused by the separation of the layers of an epicardial coronary artery wall by intramural haemorrhage, with or without an intimal tear, not associated with atherosclerosis, iatrogenic injury or trauma, leading to the formation of a false lumen wherein the axial propagation of blood flow may result in a narrowing of the true lumen. The exact pathophysiology of SCAD is complex and likely involves multiple predisposing and precipitating factors, including genetic predisposition, hormonal influences, vascular and systemic inflammation, intense exercise, emotional stress and drug abuse [35][36][35,36]. Different case reports showed that SCAD might occur in patients with MB even in the absence of other predisposing or precipitating factors and tends to localize within the intramyocardial segment or distal to the MB [37][38][37,38]. Several mechanisms may be involved, including the occurrence of coronary vasospasm in the bridged segment that could increase its susceptibility to dissection or the presence of MB-induced endothelial dysfunction [19][39][19,39]. Moreover, the flow disturbance caused by the pressure gradient between the bridged and non-bridged segment can lead to a state of chronic coronary pressure overload, which may cause intimal trauma, which eventually leads to intimal tearing and coronary dissection [40]. Finally, previous studies have reported that MINOCA might be associated with a low but still not neglectable rate of complications during the acute phase, mainly represented by intraventricular septal rupture, free wall rupture with pericardial effusion or cardiac tamponade and ventricular arrhythmias [41]. A case of ventricular septal rupture caused by MINOCA has recently been reported, in which a septal branch steal phenomenon might have contributed to its occurrence [42]. However, to date, there are no data reporting the risk of mechanical complications in MB-related MINOCA, likely because this association is still frequently underdiagnosed in clinical practice.3. Invasive Diagnostic Approach to Patients with MINOCA and MB
Coronary angiography is the cornerstone for the diagnosis of MINOCA by excluding the presence of stenosis of more than 50% in any major epicardial coronary artery. The use of intracoronary vasodilators during diagnostic coronary angiography can increase the systolic “milking” of the tunnelled artery induced by the systolic compression of the intramural artery and facilitate the detection of MB [43][44][43,44]. A significant “milking effect” is present when there is a visual >70% reduction in the minimal luminal diameter during systole and a persistent >35% reduction in the minimal luminal diameter during mid-to-late diastole. Once the diagnosis of MINOCA and MB has been established or suspected, the use of advanced diagnostic techniques might be performed at the time of coronary angiography, aiming at confirming the presence of MB and identifying the presence of one of the above-described mechanisms of MINOCA associated with MB (Figure 1).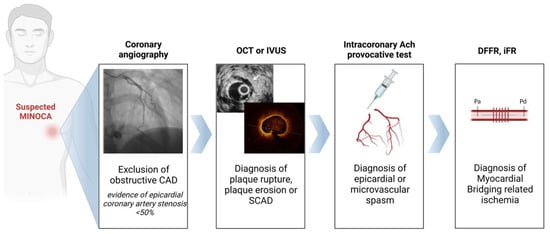
Figure 1. Invasive diagnostic algorithm in patients with MINOCA associated with myocardial bridging. Abbreviations: CAD: coronary artery disease; DFFR: diastolic fractional flow reserve; iFR: instantaneous wave-free ratio; IVUS: intravascular ultrasound; MINOCA: myocardial infarction with non-obstructed coronary arteries; OCT: optical coherence tomography; SCAD: spontaneous coro-nary artery dissection.
4. Therapeutic Implications
The management of MINOCA still has a limited number of evidence-based studies, as only a few registries have addressed this issue, and there is a strong need for randomized controlled trials in this setting [66][67][66,67]. Adding complexity, specific therapeutic considerations are likely needed in patients presenting with MINOCA in which a specific pathogenetic mechanism associated with MB is diagnosed (Table 1). However, there is a lack of evidence supporting any specific intervention as well as reporting the incremental prognosis of MINOCA associated with a MB. Accordingly, there is a strong need for properly designed randomized clinical trials as well as for data from observational studies or registry to support recommendations in future clinical consensus or guidelines in these patients.Table 1. Therapeutic implications according to the underlying pathogenetic mechanism of MINOCA associated with a MB.
| Pathogenetic Mechanism of MINOCAAssociated with a MB | Therapeutic Implications |
|---|---|
| Plaque rupture |
|
| Plaque erosion |
|
| SCAD |
|
| Epicardial coronary spasm |
|
| Microvascular coronary spasm |
|
| MB-related ischaemia |
|
Abbreviations: MINOCA: myocardial infarction with non-obstructed coronary arteries; MB: myocardial bridge; PCI: percutaneous coronary intervention; DAPT: dual antiplatelet therapy; SAPT: single antiplatelet therapy; SCAD: spontaneous coronary artery dissection; CCBs: calcium channel blockers; CABG: coronary artery bypass grafting.