Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Alexandro Guterres | -- | 2946 | 2024-03-07 18:43:36 | | | |
| 2 | Peter Tang | Meta information modification | 2946 | 2024-03-08 02:55:29 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Guterres, A.; Filho, P.N.S.; Moura-Neto, V. Glioblastoma Therapy with mRNA-Based Immunotherapies and Oncolytic Viruses. Encyclopedia. Available online: https://encyclopedia.pub/entry/55987 (accessed on 27 July 2026).
Guterres A, Filho PNS, Moura-Neto V. Glioblastoma Therapy with mRNA-Based Immunotherapies and Oncolytic Viruses. Encyclopedia. Available at: https://encyclopedia.pub/entry/55987. Accessed July 27, 2026.
Guterres, Alexandro, Paulo Niemeyer Soares Filho, Vivaldo Moura-Neto. "Glioblastoma Therapy with mRNA-Based Immunotherapies and Oncolytic Viruses" Encyclopedia, https://encyclopedia.pub/entry/55987 (accessed July 27, 2026).
Guterres, A., Filho, P.N.S., & Moura-Neto, V. (2024, March 07). Glioblastoma Therapy with mRNA-Based Immunotherapies and Oncolytic Viruses. In Encyclopedia. https://encyclopedia.pub/entry/55987
Guterres, Alexandro, et al. "Glioblastoma Therapy with mRNA-Based Immunotherapies and Oncolytic Viruses." Encyclopedia. Web. 07 March, 2024.
Copy Citation
Glioblastoma multiforme (here termed GBM), one of the most aggressive and lethal primary brain tumors, poses a significant challenge in the field of neuro-oncology. The use of mRNA-based immunotherapies that leverage the genomes of oncolytic viruses holds significant promise in addressing glioblastoma (GBM), an exceptionally aggressive neurological tumor.
molecular therapy
mRNA-based immunotherapy
oncolytic virus
glioblastoma
cancer treatment
Zika virus
glioblastoma stem cells
oncolytic virotherapy
1. Introduction
Brain tumors are a critical area of study within the realm of medical research and neuro-oncology. These neoplastic growths, originating from abnormal cell proliferation in the brain or its adjacent tissues, encompass a wide spectrum of biological behaviors and clinical manifestations [1]. These tumors can be broadly classified into two categories: primary brain tumors, which develop directly from brain cells, and secondary brain tumors, also known as metastatic tumors, which originate from cancer cells that have spread to the brain from other parts of the body [2]. Brain tumors pose complex medical challenges because of their intricate location in the central nervous system and their potential to affect various cognitive, motor, and sensory functions [3][4].
Glioblastoma multiforme (here termed GBM), one of the most aggressive and lethal primary brain tumors, poses a significant challenge in the field of neuro-oncology [5][6]. Its intricate biological characteristics, including rapid growth, high invasiveness, and resistance to conventional therapies contribute to its notorious reputation [7]. The presence of a family of proteins that are resistant and extrude drugs (multidrug resistance MDR) such as temozolomide contributes crucially to tumor survival. The genome landscape and heterogeneity of GBM further complicate treatment, necessitating an in-depth exploration of its molecular underpinnings [8][9]. With advances in genome profiling and molecular analysis, researchers are uncovering key genetic alterations and signaling pathways that drive GBM progression [8].
Despite advances in radiation therapy, chemotherapy and targeted agents, inherent biological heterogeneity, intricate cellular interactions, and the presence of a protective blood–brain barrier collectively thwart successful treatment outcomes [10][11][12]. The relentless recurrence of glioblastoma and the limited success in significantly extending patient survival underscore the urgent need for innovative and multidimensional therapeutic paradigms to combat this formidable malignancy. The difficulty of treating GBM lies in its cellular heterogeneity, which together with the surrounding microenvironment contributes to the tumor progression and “protection”. With respect to GBM, the singular contribution of their stem cells allows growth, diffusion, and establishment of the tumor in a second or third region of the brain, leading to recurrence. The central point of attack for this tumor could be these tumor stem cells [13]. These stem cells diffuse within the brain, generating new foci of tumorigenesis in different regions. Tumors are currently understood to derive originally from the monoclonal expansion of stem cells, clonal selection due to mutations, or chromosome instability [14]. Furthermore, expanding stem cells can differentiate into tumor cells or from these become stem cells, a transition followed by expression of markers such as indicated below in both phases of these changes [13] (Figure 1).
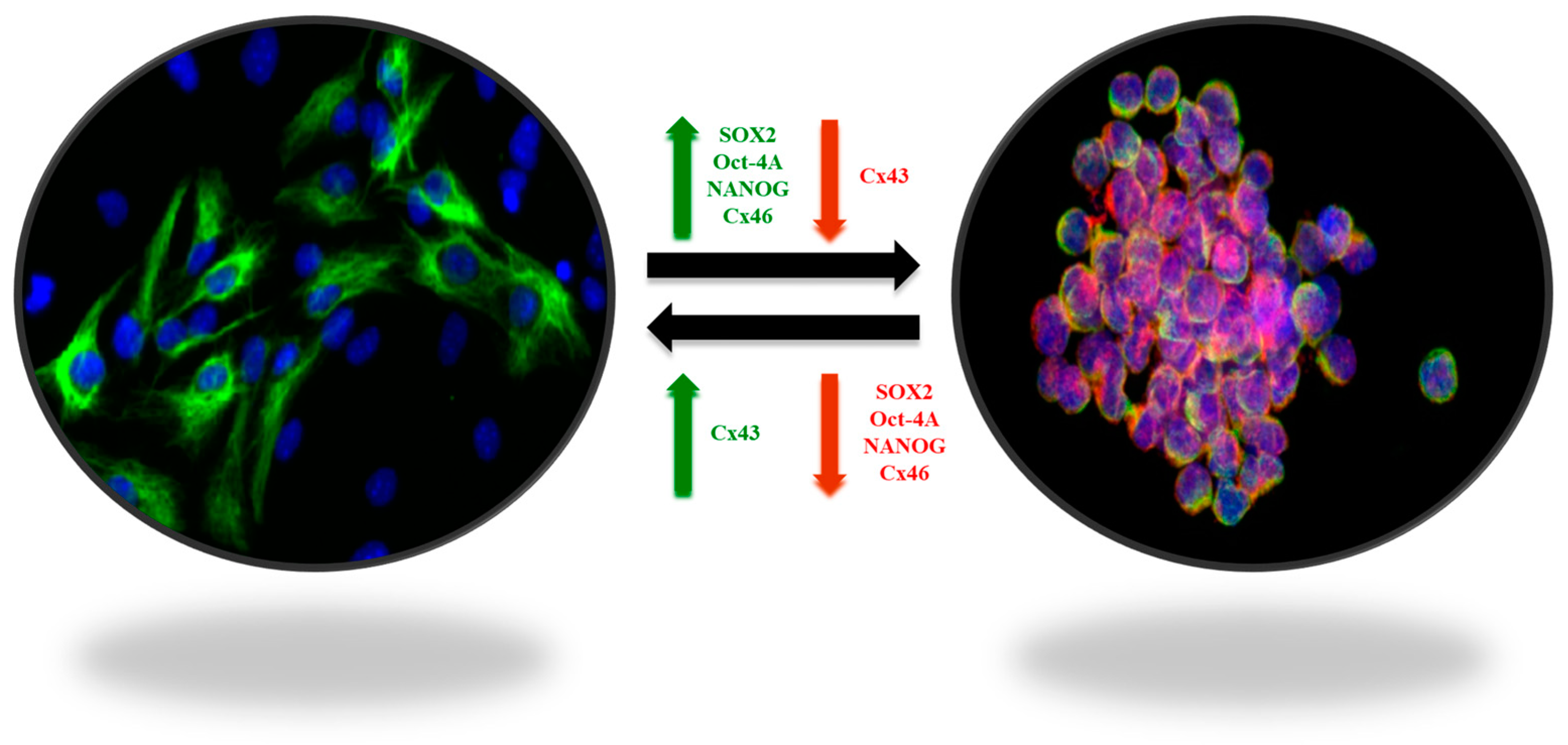
Figure 1. Plasticity of GBM stem-like cells. The balance between self-renewal and differentiation properties is dynamic and controlled by interactions of tumor cells with their microenvironment. The stem-like cell markers SOX2, OCT-4A, Nanog, and connexin 46 (Cx46), involved in cell-to-cell communication processes, are overexpressed in GSCs (green arrow), whereas connexin 43 (Cx43) is downregulated (red arrow). In contrast, in non-GSCs, SOX2, OCT-4A, Nanog, and Cx46 are downregulated (red arrow), whereas Cx43 in overexpressed (green arrow) [13].
2. Oncolytic Virotherapy
Oncolytic virotherapy, an expanding frontier in cancer treatment, revolves around the strategic use of viruses as therapeutic agents to target and eliminate malignant cells [15]. This innovative approach capitalizes on the inherent ability of certain viruses to selectively infect and replicate in cancer cells, leading to their destruction while sparing healthy tissues. Engineered virotherapies leverage modifications that enhance tumor selectivity, replication efficiency, and immune activation, fostering a multifaceted assault on the tumor microenvironment [16][17]. The viral oncolysis, coupled with the potential for tumor-specific antigen release, fuels antitumor immune responses, thereby amplifying the therapeutic impact [18]. A spectrum of viruses, including adenoviruses, herpesviruses, and measles viruses, among others, have yielded promising outcomes in preclinical and clinical settings. Oncolytic virotherapy, bridging virology and oncology, harnesses viruses as powerful allies in the ongoing quest to develop more effective, targeted, and personalized strategies to combat cancer [16].
The field of neuro-oncology research has seen promising growth with the emergence of clinical trials investigating adenovirus-based therapies for brain tumors [19]. Adenoviruses, renowned for their broad cell infectivity, have been strategically repurposed to capitalize on their oncolytic potential against brain malignancies. Engineered through genetic modifications, adenoviruses, exemplifying their prowess, selectively replicate in tumor cells by capitalizing on their distinct signaling pathways and inducing targeted cell death [20][21]. Furthermore, adenoviruses can be equipped with therapeutic transgenes to increase their antitumor properties. Many clinical trials, meticulously documented on platforms such as ClinicalTrials.gov, have examined the safety and therapeutic efficacy of adenovirus-based interventions in patients with brain tumors, including glioblastoma and various intracranial malignancies. These trials have used an array of treatment strategies, ranging from localized intratumor administration of replication-competent adenoviruses to the delivery of engineered adenoviral vectors encoding tumor-suppressive genes or immune-boosting agents [21][22]. Preliminary results have indicated tumor regression, extended survival rates, and potential synergistic interactions with complementary therapeutic modalities. The multifaceted approach of adenovirus-based therapies, combining oncolytic and immunomodulatory mechanisms, offers a promising avenue to surmount the complex hurdles posed by brain tumors and transcend the confines of traditional treatments [23][24]. As research in this area evolves, clinical trials using adenovirus-based strategies may result in innovative therapeutic initiatives for brain tumors [25][26]. These trials, in addition to underscoring the adaptability of adenoviruses as versatile tools in the realm of neuro-oncology, spark a renewed sense of optimism for the development of more efficacious and individualized treatments, rekindling hope for patients contending with these formidable malignancies [23][27][28].
The selection of specific virus entities for oncolytic virotherapy involves a careful consideration of the potential advantages and disadvantages inherent to each candidate. Adenoviruses, for instance, are renowned for their efficient gene delivery capabilities and well-established safety profiles, making them attractive candidates for oncolytic applications. However, concerns about preexisting immunity and limited capacity for sustained replication may impact their therapeutic efficacy. Herpes simplex viruses (HSV), including those engineered such as G47, exhibit strong lytic activity against tumor cells and have the advantage of prolonged replication within the neoplastic environment. Nevertheless, the potential for neurotoxicity and the development of antiviral resistance are noteworthy considerations [29]. RNA viruses, such as measles viruses, are characterized by robust oncolytic potential and the ability to trigger potent antitumor immune responses. However, their rapid clearance by the immune system and the risk of toxicity poses challenges [30]. A careful evaluation of these advantages and disadvantages is essential for informed decision making in the development of oncolytic virotherapies, with the aim of optimizing their safety and efficacy profiles for cancer treatment [31]. Ensuring the stability and activity of oncolytic viruses is paramount for their successful clinical utilization in cancer therapy. The imperative for long-term storage stability in clinical settings underscores the importance of formulation design in preserving the efficacy of oncolytic viruses. Some authors address critical degradation factors and their mechanisms, including pH variations, thermal stress, freeze–thaw damage, surface adsorption, and oxidation, which oncolytic viruses encounter during storage [32].
While the majority of clinical studies are currently in phase II [33], a notable exception is observed in Japan where the Ministry of Health, Labour and Welfare (MHLW) granted conditional approval to Daiichi Sankyo’s oncolytic virotherapy, Delytact (G47∆; teserpaturev), for the treatment of malignant glioma in 2021. This groundbreaking decision not only marks the first approval of Delytact, but also signifies the inaugural approval of an oncolytic virus treatment for brain cancer. Delytact, a collaborative development of Daiichi Sankyo and the University of Tokyo’s Institute of Medical Science, is a triple-mutated, replication-conditional herpes simplex virus type 1 (HSV-1) engineered to selectively replicate within cancer cells. Referred to as oncolytic immunotherapy, these engineered viruses exhibit selective replication in tumor cells until cellular lysis occurs, followed by the release of additional viruses targeting successive tumor cells. The approval, valid for seven years, is based on data from a single-arm, investigator-initiated Phase II study in Japan in patients with residual or recurrent glioblastoma, where Delytact met the primary endpoint of a one-year survival rate [34][35].
3. Oncolytic Virotherapy and Self-Amplifying RNA Technology
Groundbreaking advances in cancer therapeutics include the fusion of oncolytic virotherapy and self-amplifying RNA technology. These cutting-edge methods not only harness the potential of mRNA-based platforms within immunotherapies but also may alleviate the risks inherent in employing live viruses in the treatment of cancer [36][37]. In recent years, mRNA, the intermediary between DNA and protein synthesis, has been ingeniously repurposed to elicit robust immune responses against a range of diseases. This innovation capitalizes on the inherent ability of mRNA to encode antigenic information, thereby enabling the precise design and production of immunogenic proteins within host cells [38]. This revolutionary approach has opened avenues to address the complex challenges posed by various diseases, prominently including cancer. In the context of cancer, mRNA technology offers unprecedented opportunities for personalized and targeted therapeutic strategies [39]. By leveraging the customizable nature of mRNA sequences, researchers can precisely tailor therapeutic agents to trigger immune responses against cancer-specific antigens. This has inaugurated a new era in cancer immunotherapy, where mRNA-based vaccines and therapeutics have immense promise in harnessing the immune system to selectively recognize and eliminate malignant cells while minimizing damage to healthy tissues [40][41][42].
The use of self-amplifying RNA (saRNA) technology represents a cutting-edge approach in the field of nucleic acid-based therapeutics. This innovative technology involves the design and engineering of RNA molecules capable of not only encoding therapeutic proteins but also facilitating their own replication within host cells [43][44]. The constructs of saRNA are relatively large, with reports indicating sizes of up to 15,000 nucleotides [44][45]. Unlike conventional mRNA, saRNA possesses elements derived from positive-sense RNA viruses, such as alphaviruses. SaRNA vaccines employ RNA-dependent RNA polymerases (RDRP) derived primarily from RNA viruses, predominantly alphaviruses, to facilitate the amplification of the delivered RNA, thus augmenting the production of antigen proteins. In addition to the typical mRNA components, saRNA encompasses substantial open reading frames (ORF) encoding the elements necessary for RDRP, comprising nonstructural proteins 1-4 (nsP1-4), and the gene of interest, all under the control of a subgenomic promoter. The nsP1, 2, 3, and 4 sequences govern the synthesis of proteins responsible for mRNA capping, NTPase/Helicase/protease, macrodomain, and RDRP, respectively [46][47]. Upon cellular uptake, the saRNA enters the host cell’s cytoplasm, where it utilizes the cellular machinery to both translate the therapeutic protein of interest and replicate its own RNA. This inherent self-amplification feature results in a robust and prolonged protein expression, enhancing the efficiency of the therapeutic intervention [44][48]. Alphaviruses, for instance, can accumulate an estimated 106 RNA copies per cell [49]. The expression in saRNA technology is considerably more enduring compared to the conventional mRNA platform, with a persistence typically extending over several days. This prolonged duration is attributed to the inherent characteristics of saRNA, making it particularly suitable for applications in vaccine development and cancer therapy [47]. Additionally, the multifunctional composition permits the simultaneous encoding of multiple antigens or immunomodulatory elements within a single construct, thus engendering a more nuanced and versatile immune response. The inherent capability of saRNA to accommodate multifunctional compositions is a pivotal point in the advancement of genetic therapeutics [43][44][50]. This attribute confers on saRNA a unique versatility, enabling the concurrent encoding of several antigens or immunomodulatory elements within a single construct. By orchestrating such complex genetic architectures, saRNA can trigger a dynamic and multifaceted immune response, heightening the efficacy of disease intervention [43][51][52][53]. This nuanced approach has the potential to stimulate the activation of various components of the immune system, including cellular and humoral responses, while simultaneously tailoring the immune environment to target specific pathogenic challenges. In addition, the multifunctional capacity of saRNA not only amplifies the immunity stimulating potential but also streamlines the administration process, as multiple therapeutic components can be delivered simultaneously [45][54][55].
Strategic integration of the saRNA multifunctional composition for use in oncolytic virotherapy is a remarkable advancement, with transformative implications for antitumor interventions. By capitalizing on the unique capability to accommodate the simultaneous encoding of various antigens or immunomodulatory elements within a unified construct [43][44][51], the potential of saRNA-driven oncolytic virotherapy is poised for a paradigm shift. Through this approach, saRNA can be tailored to elicit an intricately orchestrated and adaptable immune response against malignancies [45][55]. For instance, this strategy could encompass the delivery of a composition of structural proteins that assemble into nonreplicating virus-like particles, potentially mimicking viral presentation while mitigating replication risk. Alternatively, a hybrid composition could be devised, blending structural and non-structural proteins with intrinsic oncolytic capabilities (Figure 2). This multifaceted approach enables the therapeutic construct to exert concerted antitumor effects, utilizing multiple modalities of immune engagement while targeting distinct aspects of tumor biology. Consequently, this innovative integration embodies a convergence of precise genetic manipulation and oncolytic viral vectors, culminating in a finely tuned arsenal capable of triggering an adaptable, versatile, and potentially curative immune response against cancer.

Figure 2. The mRNA platform, primarily self-amplifying RNA technology, demonstrates a broad range of possibilities for potential therapeutic constructs employing the genome of an oncolytic virus, represented here by the Zika virus. In the first construct, the entire genome of the Zika virus is used with modifications that make it attenuated. In the second construct, structural proteins of the Zika virus are employed, resulting in the formation of a non-infectious empty particle. In the third construct, non-structural proteins are used to create a cluster of proteins with potential oncolytic properties. In the fourth construct, a combination of two Zika virus polyproteins is proposed, one containing structural and the other non-structural elements, potentially forming an infectious viral particle. In the fifth construct, it is possible to combine some structural and non-structural proteins to form a cluster of oncolytic proteins or even a non-infectious particle containing both structural and select non-structural proteins.
Both DNA and RNA viruses induce a metabolic shift and exploit cellular mechanisms, including the cell cycle and signaling pathways, within host cells to optimize viral production [56]. The genomic structure of viruses encompasses two transcriptional units responsible for encoding structural and non-structural proteins. Structural proteins, integral to viral particles, perform vital functions such as cellular recognition, fusion, entry, or replication [57][58]. On the other hand, non-structural proteins (NS) are implicated in diverse cellular hijacking processes, such as the formation of inclusion bodies, interaction with the cytoskeleton, induction of apoptosis, and modulation of autophagy [59][60]. Although the functional roles of all NS proteins remain incompletely understood, some actively participate in the virus’s replication and latency cycle. Varied viral proteins follow distinct yet converging pathways to selectively modulate cellular events like the cell cycle and apoptosis in human cancer cells, leveraging existing aberrations for targeted effects [61]. Leveraging saRNA technology makes it possible to seamlessly integrate structural proteins, which exhibit high affinity for tumor cells (in terms of cell recognition, fusion, and entry), with non-structural proteins known for their robust oncolytic capabilities. This strategic fusion enables a nuanced and targeted approach, capitalizing on the distinct strengths of each protein category to amplify the efficacy of the oncolytic virus against cancer cells. This genetic manipulation opens avenues to leverage the best attributes of diverse oncolytic viruses, regardless of their genomic types.
The utilization of various viral genomes within the saRNA platform requires a careful consideration of distinct mechanisms associated with different viral types. The selection of viral genomes plays a pivotal role in defining the characteristics and potential applications of saRNA. For dsDNA viruses, such as adenovirus, vaccinia virus, and herpesvirus, saRNA sequences must encompass the essential elements needed for these processes. The design should consider encoding components like need to include promoters that facilitate the transcription of viral genes and regulatory elements to control the timing and efficiency of gene expression [62][63][64]. This involves designing saRNA sequences that mimic the necessary viral components responsible for initiating these processes, ensuring compatibility with the host cell machinery.
On the other hand, for ssRNA viruses, whether positive-sense (e.g., coxsackievirus, Seneca Valley virus, poliovirus) or negative-sense (e.g., measles virus, Newcastle Disease virus, vesicular stomatitis virus), the saRNA platform must be tailored to replicate the specific genomic features of these viruses. In positive-sense ssRNA viruses, saRNA sequences should be designed to directly translate into proteins upon entering host cells. In contrast, for negative-sense ssRNA viruses, the saRNA design needs to account for the complementary nature of the viral mRNA, ensuring an intermediate step of transcription into positive-sense RNA before translation occurs. The challenge lies in precisely mimicking the viral genomic elements while maintaining the inherent safety and stability associated with saRNA technology [62][65][66]. Strategies may involve integrating coding sequences for essential viral proteins and utilizing subgenomic promoters to drive the expression of genes of interest. Careful consideration of the unique replication strategies of each virus type is crucial for achieving effective and controlled gene expression within the saRNA platform.
Expanding on the insights garnered from the current research, it is imperative to recognize that within the domain of oncolytic virotherapy, a myriad of viruses, each harboring unique oncolytic potential, can be explored beyond the exemplified Zika virus (ZIKV). In addition to ZIKV, other oncolytic viruses, including adenoviruses, herpesviruses, and measles viruses, exhibit distinct genomic attributes that can be strategically employed in the design of protein compositions [21][27]. This strategic approach seeks to optimize oncolytic potential while simultaneously mitigating the inherent risks associated with live virus applications. This inclusive exploration of different oncolytic viruses, coupled with the utilization of saRNA technology, enriches the oncolytic virotherapy toolkit. Not only does it broaden the spectrum of therapeutic options, it also underscores the potential for a nuanced and personalized approach in the ongoing pursuit of effective cancer treatments [18][21]. Continued investigation of various oncolytic viruses, augmented by the capabilities of saRNA technology, holds the promise of advancing precision medicine in cancer therapeutics.
References
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro Oncol. 2021, 23, 1231–1251.
- Aldape, K.; Brindle, K.M.; Chesler, L.; Chopra, R.; Gajjar, A.; Gilbert, M.R.; Gottardo, N.; Gutmann, D.H.; Hargrave, D.; Holland, E.C.; et al. Challenges to Curing Primary Brain Tumours. Nat. Rev. Clin. Oncol. 2019, 16, 509–520.
- Giglio, P.; Gilbert, M.R. Neurologic Complications of Cancer and Its Treatment. Curr. Oncol. Rep. 2010, 12, 50–59.
- Lee, E.Q.; Chukwueke, U.N.; Hervey-Jumper, S.L.; de Groot, J.F.; Leone, J.P.; Armstrong, T.S.; Chang, S.M.; Arons, D.; Oliver, K.; Verble, K.; et al. Barriers to Accrual and Enrollment in Brain Tumor Trials. Neuro Oncol. 2019, 21, 1100–1117.
- Davis, M. Glioblastoma: Overview of Disease and Treatment. Clin. J. Oncol. Nurs. 2016, 20, S2–S8.
- Hanif, F.; Muzaffar, K.; Perveen, K.; Malhi, S.M.; Simjee, S.U. Glioblastoma Multiforme: A Review of Its Epidemiology and Pathogenesis through Clinical Presentation and Treatment. Asian Pac. J. Cancer Prev. 2017, 18, 3–9.
- Rominiyi, O.; Vanderlinden, A.; Clenton, S.J.; Bridgewater, C.; Al-Tamimi, Y.; Collis, S.J. Tumour Treating Fields Therapy for Glioblastoma: Current Advances and Future Directions. Br. J. Cancer 2021, 124, 697–709.
- Lombardi, M.Y.; Assem, M. Glioblastoma Genomics: A Very Complicated Story. In Glioblastoma; Codon Publications: Singapore, 2017; pp. 3–25.
- Liu, D.; Chen, J.; Hu, X.; Yang, K.; Liu, Y.; Hu, G.; Ge, H.; Zhang, W.; Liu, H. Imaging-Genomics in Glioblastoma: Combining Molecular and Imaging Signatures. Front. Oncol. 2021, 11, 699265.
- Park, J.H.; de Lomana, A.L.G.; Marzese, D.M.; Juarez, T.; Feroze, A.; Hothi, P.; Cobbs, C.; Patel, A.P.; Kesari, S.; Huang, S.; et al. A Systems Approach to Brain Tumor Treatment. Cancers 2021, 13, 3152.
- Tan, A.C.; Ashley, D.M.; López, G.Y.; Malinzak, M.; Friedman, H.S.; Khasraw, M. Management of Glioblastoma: State of the Art and Future Directions. CA Cancer J. Clin. 2020, 70, 299–312.
- Fernandes, C.; Costa, A.; Osório, L.; Lago, R.C.; Linhares, P.; Carvalho, B.; Caeiro, C. Current Standards of Care in Glioblastoma Therapy. In Glioblastoma; Codon Publications: Singapore, 2017; pp. 197–241.
- Balça-Silva, J.; Matias, D.; Do Carmo, A.; Dubois, L.G.; Gonçalves, A.C.; Girão, H.; Silva Canedo, N.H.; Correia, A.H.; De Souza, J.M.; Sarmento-Ribeiro, A.B.; et al. Glioblastoma Entities Express Subtle Differences in Molecular Composition and Response to Treatment. Oncol. Rep. 2017, 38, 1341–1352.
- Magee, J.A.; Piskounova, E.; Morrison, S.J. Cancer Stem Cells: Impact, Heterogeneity, and Uncertainty. Cancer Cell 2012, 21, 283–296.
- Kelly, E.; Russell, S.J. History of Oncolytic Viruses: Genesis to Genetic Engineering. Mol. Ther. 2007, 15, 651–659.
- Lin, D.; Shen, Y.; Liang, T. Oncolytic Virotherapy: Basic Principles, Recent Advances and Future Directions. Signal Transduct. Target. Ther. 2023, 8, 156.
- Chaurasiya, S.; Chen, N.G.; Fong, Y. Oncolytic Viruses and Immunity. Curr. Opin. Immunol. 2018, 51, 83–90.
- Bommareddy, P.K.; Shettigar, M.; Kaufman, H.L. Integrating Oncolytic Viruses in Combination Cancer Immunotherapy. Nat. Rev. Immunol. 2018, 18, 498–513.
- Fares, J.; Ahmed, A.U.; Ulasov, I.V.; Sonabend, A.M.; Miska, J.; Lee-Chang, C.; Balyasnikova, I.V.; Chandler, J.P.; Portnow, J.; Tate, M.C.; et al. Neural Stem Cell Delivery of an Oncolytic Adenovirus in Newly Diagnosed Malignant Glioma: A First-in-Human, Phase 1, Dose-Escalation Trial. Lancet Oncol. 2021, 22, 1103–1114.
- Rosewell Shaw, A.; Porter, C.; Biegert, G.; Jatta, L.; Suzuki, M. HydrAd: A Helper-Dependent Adenovirus Targeting Multiple Immune Pathways for Cancer Immunotherapy. Cancers 2022, 14, 2769.
- Harrington, K.; Freeman, D.J.; Kelly, B.; Harper, J.; Soria, J.-C. Optimizing Oncolytic Virotherapy in Cancer Treatment. Nat. Rev. Drug Discov. 2019, 18, 689–706.
- Cunliffe, T.G.; Bates, E.A.; Parker, A.L. Hitting the Target but Missing the Point: Recent Progress towards Adenovirus-Based Precision Virotherapies. Cancers 2020, 12, 3327.
- Nandi, S.; Lesniak, M.S. Adenoviral Virotherapy for Malignant Brain Tumors. Expert Opin. Biol. Ther. 2009, 9, 737–747.
- Hensen, L.C.M.; Hoeben, R.C.; Bots, S.T.F. Adenovirus Receptor Expression in Cancer and Its Multifaceted Role in Oncolytic Adenovirus Therapy. Int. J. Mol. Sci. 2020, 21, 6828.
- de Gruijl, T.D.; van de Ven, R. Adenovirus-Based Immunotherapy of Cancer: Promises to Keep. Adv. Cancer Res. 2012, 115, 147–220.
- Chu, R.L.; Post, D.E.; Khuri, F.R.; Van Meir, E.G. Use of Replicating Oncolytic Adenoviruses in Combination Therapy for Cancer. Clin. Cancer Res. 2004, 10, 5299–5312.
- Hemminki, O.; dos Santos, J.M.; Hemminki, A. Oncolytic Viruses for Cancer Immunotherapy. J. Hematol. Oncol. 2020, 13, 84.
- Sato-Dahlman, M.; LaRocca, C.J.; Yanagiba, C.; Yamamoto, M. Adenovirus and Immunotherapy: Advancing Cancer Treatment by Combination. Cancers 2020, 12, 1295.
- Scanlan, H.; Coffman, Z.; Bettencourt, J.; Shipley, T.; Bramblett, D.E. Herpes Simplex Virus 1 as an Oncolytic Viral Therapy for Refractory Cancers. Front. Oncol. 2022, 12, 940019.
- Marchini, A.; Daeffler, L.; Pozdeev, V.I.; Angelova, A.; Rommelaere, J. Immune Conversion of Tumor Microenvironment by Oncolytic Viruses: The Protoparvovirus H-1PV Case Study. Front. Immunol. 2019, 10, 1848.
- Kaufman, H.L.; Kohlhapp, F.J.; Zloza, A. Oncolytic Viruses: A New Class of Immunotherapy Drugs. Nat. Rev. Drug Discov. 2015, 14, 642–662.
- Pan, L.; Liu, X.; Fan, D.; Qian, Z.; Sun, X.; Wu, P.; Zhong, L. Study of Oncolytic Virus Preservation and Formulation. Pharmaceuticals 2023, 16, 843.
- Todo, T.; Ito, H.; Ino, Y.; Ohtsu, H.; Ota, Y.; Shibahara, J.; Tanaka, M. Intratumoral Oncolytic Herpes Virus G47∆ for Residual or Recurrent Glioblastoma: A Phase 2 Trial. Nat. Med. 2022, 28, 1630–1639.
- Maruyama, Y.; Sakurai, A.; Noda, S.; Fujiwara, Y.; Okura, N.; Takagi, T.; Asano, J.; Honda, F. Regulatory Issues: PMDA—Review of Sakigake Designation Products: Oncolytic Virus Therapy with Delytact Injection (Teserpaturev) for Malignant Glioma. Oncologist 2023, 28, 664–670.
- Wu, X.; Alvarez-Breckenridge, C. Moving the Pendulum for Glioblastoma Treatment: One Injection at a Time. Oncologist 2023, 28, 651–653.
- Pardi, N.; Hogan, M.J.; Porter, F.W.; Weissman, D. MRNA Vaccines—A New Era in Vaccinology. Nat. Rev. Drug Discov. 2018, 17, 261–279.
- Chehelgerdi, M.; Chehelgerdi, M. The Use of RNA-Based Treatments in the Field of Cancer Immunotherapy. Mol. Cancer 2023, 22, 106.
- Schlake, T.; Thess, A.; Fotin-Mleczek, M.; Kallen, K.-J. Developing MRNA-Vaccine Technologies. RNA Biol. 2012, 9, 1319–1330.
- Al Fayez, N.; Nassar, M.S.; Alshehri, A.A.; Alnefaie, M.K.; Almughem, F.A.; Alshehri, B.Y.; Alawad, A.O.; Tawfik, E.A. Recent Advancement in MRNA Vaccine Development and Applications. Pharmaceutics 2023, 15, 1972.
- Huang, X.; Kong, N.; Zhang, X.; Cao, Y.; Langer, R.; Tao, W. The Landscape of MRNA Nanomedicine. Nat. Med. 2022, 28, 2273–2287.
- Deng, Z.; Tian, Y.; Song, J.; An, G.; Yang, P. MRNA Vaccines: The Dawn of a New Era of Cancer Immunotherapy. Front. Immunol. 2022, 13, 887125.
- Han, G.; Noh, D.; Lee, H.; Lee, S.; Kim, S.; Yoon, H.Y.; Lee, S.H. Advances in MRNA Therapeutics for Cancer Immunotherapy: From Modification to Delivery. Adv. Drug Deliv. Rev. 2023, 199, 114973.
- Bloom, K.; van den Berg, F.; Arbuthnot, P. Self-Amplifying RNA Vaccines for Infectious Diseases. Gene Ther. 2021, 28, 117–129.
- Papukashvili, D.; Rcheulishvili, N.; Liu, C.; Ji, Y.; He, Y.; Wang, P.G. Self-Amplifying RNA Approach for Protein Replacement Therapy. Int. J. Mol. Sci. 2022, 23, 12884.
- Blakney, A.K.; Ip, S.; Geall, A.J. An Update on Self-Amplifying MRNA Vaccine Development. Vaccines 2021, 9, 97.
- Abu Bakar, F.; Ng, L. Nonstructural Proteins of Alphavirus—Potential Targets for Drug Development. Viruses 2018, 10, 71.
- Kim, J.; Eygeris, Y.; Gupta, M.; Sahay, G. Self-Assembled MRNA Vaccines. Adv. Drug Deliv. Rev. 2021, 170, 83–112.
- Gote, V.; Bolla, P.K.; Kommineni, N.; Butreddy, A.; Nukala, P.K.; Palakurthi, S.S.; Khan, W. A Comprehensive Review of MRNA Vaccines. Int. J. Mol. Sci. 2023, 24, 2700.
- Frolov, I.; Hoffman, T.A.; Prágai, B.M.; Dryga, S.A.; Huang, H.V.; Schlesinger, S.; Rice, C.M. Alphavirus-Based Expression Vectors: Strategies and Applications. Proc. Natl. Acad. Sci. USA 1996, 93, 11371–11377.
- Ballesteros-Briones, M.C.; Silva-Pilipich, N.; Herrador-Cañete, G.; Vanrell, L.; Smerdou, C. A New Generation of Vaccines Based on Alphavirus Self-Amplifying RNA. Curr. Opin. Virol. 2020, 44, 145–153.
- Kwon, S.; Kwon, M.; Im, S.; Lee, K.; Lee, H. MRNA Vaccines: The Most Recent Clinical Applications of Synthetic MRNA. Arch. Pharm. Res. 2022, 45, 245–262.
- Maruggi, G.; Ulmer, J.B.; Rappuoli, R.; Yu, D. Self-Amplifying MRNA-Based Vaccine Technology and Its Mode of Action. In mRNA Vaccines; Springer International Publishing: Cham, Switzerland, 2021; pp. 31–70.
- Schmidt, C.; Schnierle, B.S. Self-Amplifying RNA Vaccine Candidates: Alternative Platforms for MRNA Vaccine Development. Pathogens 2023, 12, 138.
- Pourseif, M.M.; Masoudi-Sobhanzadeh, Y.; Azari, E.; Parvizpour, S.; Barar, J.; Ansari, R.; Omidi, Y. Self-Amplifying MRNA Vaccines: Mode of Action, Design, Development and Optimization. Drug Discov. Today 2022, 27, 103341.
- Minnaert, A.-K.; Vanluchene, H.; Verbeke, R.; Lentacker, I.; De Smedt, S.C.; Raemdonck, K.; Sanders, N.N.; Remaut, K. Strategies for Controlling the Innate Immune Activity of Conventional and Self-Amplifying MRNA Therapeutics: Getting the Message Across. Adv. Drug Deliv. Rev. 2021, 176, 113900.
- Thaker, S.K.; Ch’ng, J.; Christofk, H.R. Viral Hijacking of Cellular Metabolism. BMC Biol. 2019, 17, 59.
- Verdaguer, N.; Ferrero, D.; Murthy, M.R.N. Viruses and Viral Proteins. IUCrJ 2014, 1, 492–504.
- Fan, Y.; Sanyal, S.; Bruzzone, R. Breaking Bad: How Viruses Subvert the Cell Cycle. Front. Cell Infect. Microbiol. 2018, 8, 396.
- Tenorio, R.; Fernández de Castro, I.; Knowlton, J.J.; Zamora, P.F.; Sutherland, D.M.; Risco, C.; Dermody, T.S. Function, Architecture, and Biogenesis of Reovirus Replication Neoorganelles. Viruses 2019, 11, 288.
- Muscolino, E.; Luoto, L.-M.; Brune, W. Viral Induced Protein Aggregation: A Mechanism of Immune Evasion. Int. J. Mol. Sci. 2021, 22, 9624.
- Manocha, E.; Caruso, A.; Caccuri, F. Viral Proteins as Emerging Cancer Therapeutics. Cancers 2021, 13, 2199.
- Rampersad, S.; Tennant, P. Replication and Expression Strategies of Viruses. In Viruses; Elsevier: Amsterdam, The Netherlands, 2018; pp. 55–82.
- Koonin, E.V.; Krupovic, M.; Yutin, N. Evolution of Double-stranded DNA Viruses of Eukaryotes: From Bacteriophages to Transposons to Giant Viruses. Ann. N. Y. Acad. Sci. 2015, 1341, 10–24.
- Modrow, S.; Dietrich, F.; Truyen, U.; Schätzl, H. Viruses with a Double-Stranded DNA Genome. In Molecular Virology; Springer: Berlin/Heidelberg, Germany, 2013; pp. 625–873.
- Ho, J.S.Y.; Zhu, Z.; Marazzi, I. Unconventional Viral Gene Expression Mechanisms as Therapeutic Targets. Nature 2021, 593, 362–371.
- Poltronieri, P.; Sun, B.; Mallardo, M. RNA Viruses: RNA Roles in Pathogenesis, Coreplication and Viral Load. Curr. Genomics 2015, 16, 327–335.
More
Information
Subjects:
Neurosciences
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
485
Revisions:
2 times
(View History)
Update Date:
08 Mar 2024
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No