Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Aron Berger Syversen | -- | 4421 | 2024-01-23 16:43:09 | | | |
| 2 | Camila Xu | -25 word(s) | 4396 | 2024-01-24 01:57:05 | | | | |
| 3 | Aron Berger Syversen | Meta information modification | 4396 | 2024-01-24 15:22:49 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Syversen, A.; Dosis, A.; Jayne, D.; Zhang, Z. Pre-Processing of Signals of Wearable Sensors. Encyclopedia. Available online: https://encyclopedia.pub/entry/54258 (accessed on 26 July 2026).
Syversen A, Dosis A, Jayne D, Zhang Z. Pre-Processing of Signals of Wearable Sensors. Encyclopedia. Available at: https://encyclopedia.pub/entry/54258. Accessed July 26, 2026.
Syversen, Aron, Alexios Dosis, David Jayne, Zhiqiang Zhang. "Pre-Processing of Signals of Wearable Sensors" Encyclopedia, https://encyclopedia.pub/entry/54258 (accessed July 26, 2026).
Syversen, A., Dosis, A., Jayne, D., & Zhang, Z. (2024, January 23). Pre-Processing of Signals of Wearable Sensors. In Encyclopedia. https://encyclopedia.pub/entry/54258
Syversen, Aron, et al. "Pre-Processing of Signals of Wearable Sensors." Encyclopedia. Web. 23 January, 2024.
Copy Citation
Surgery is a common first-line treatment for many types of disease, including cancer. Mortality rates after major abdominal surgery have seen significant decreases whilst postoperative complications remain a frequent occurrence. Preoperative assessment tools are used to support patient risk stratification but do not always provide a precise and accessible assessment. Wearable sensors (WS) provide an accessible alternative that offers continuous monitoring in a non-clinical setting. Pre-processing involves all changes to data that are made in order to prepare the data for analysis. Pre-processing can be the most vital stage in data processing and has a large impact on the inferences that can be made from a data set.
wearable sensors
exercise testing
preoperative assessment
perioperative pathway
1. Introduction
Demand for general surgery is expected to increase in line with population ageing [1]. For various cancer types, abdominal surgery is considered first-line treatment [2][3]; for advanced-stage cancers, surgical treatment when combined with neoadjuvant treatment may be the only possible cure [2][3][4]. A common example of this is bowel/colorectal cancer, globally the third most common cancer [5]. Survival from bowel cancer has seen significant improvements in recent decades, with developments in surgical and perioperative care being suggested as reasons [6][7]. Further, mortality in the postoperative period has seen international decline and is frequently reported at below 5% [8][9][10]. However, postoperative complication rates in these populations have not seen the same decline.
Postoperative complications following abdominal surgery are frequently reported; up to a third of patients report some form of complication [11][12]. Common complications include surgical site infection, cardio-respiratory complications, gastrointestinal (GI) motility problems and anastomotic leak [13]. Postoperative complications have a profound impact not only on patients’ quality of life but also on the hospital as a service provider [13]. They are strongly associated with prolonged length of hospital stay, readmission to ICU and hospital re-admissions [13]. One large cohort review concluded that 23.3% of patients undergoing colorectal surgery were readmitted to hospital [14]. This results in a huge economic burden and has been evidenced widely across many studies [15]. With the population ageing, these costs are expected to increase up to 10% each year [16]. The identification of high-risk patients poses a crucial challenge for healthcare providers to optimise their allocation of resources and for the perioperative management of the patient. Preoperative assessment tools are used to support risk stratification of patients; however, none currently provide a precise assessment that is accessible to all patients.
1.1. Preoperative Assessment
Preoperative assessment occurs during the first stage of the perioperative period, as seen in Figure 1. Here, preoperative measurements are recorded from patients and used to stratify them into risk groups. The major goal of this is to identify the patients at the highest risk of perioperative morbidity and mortality [17]. As explained previously, it can also support the healthcare provider in resource allocation by estimating the support a patient may require across the perioperative pathway. However, as outlined by NICE guidelines, excessive preoperative testing is related to patient anxiety and significant delays to treatment [18]. Therefore, the benefits of testing should be carefully considered before implementation. The most common preoperative assessment tools are outlined here (see Figure 2).
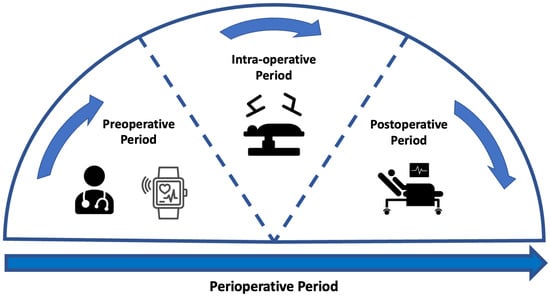
Figure 1. Figure to show the stages across the perioperative period. The perioperative pathway refers to the period that spans from the first point at which surgery is considered as a treatment option up until the full recovery [19]. This pathway has several sub-stages [20]. The preoperative period represents the period prior to surgery where any preoperative assessment takes place. The intra-operative period is representative of the period whilst the patient is undergoing treatment. The postoperative period relates to any period immediately following the operation and can continue after patient discharge.
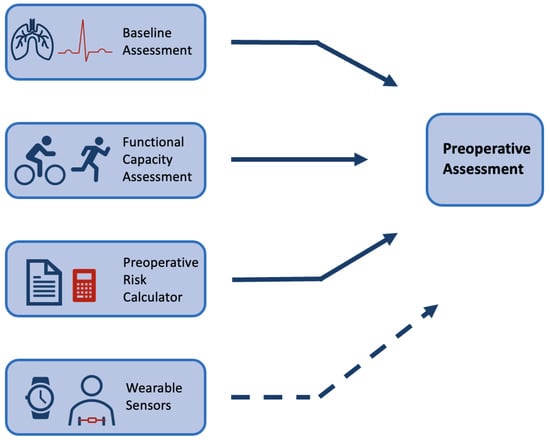
Figure 2. Figure to show common preoperative assessment tools used in practice. The top three boxes present common forms of preoperative assessment that are regularly used in practice (see Section 1.1), whilst the last box with a dashed arrow is included to show the potential for wearable sensors to be used alongside common methods in this context.
Physical examinations build on an assessment of the patient’s medical history. These pre-anaesthesia examinations include a physical assessment of the lungs, heart function and possible evaluation of the main vital signs using a variety of tests [17][18]. NICE guidelines provide a breakdown of recommendations for testing that vary depending on the severity of the surgical treatment and health status of the patient [18]. For example, an ECG is a common tool that has been shown to optimise risk stratification of cardiovascular complications for non-cardiac surgery [21]. However, for minor/intermediate treatments in young or patients considered healthy, a resting ECG is not recommended as part of routine preoperative assessment [18]. These physical assessments are routinely performed at a preoperative clinic appointment in a resting state.
Multiple preoperative assessment tools exist that calculate patients’ risk of adverse outcomes from routinely collected data. These tools are widely recommended by medical societies to be employed as a preoperative assessment tool [22]. The ASA system (American Society of Anaethesiology), the APACHE II (Acute Physiology and Chronic Health Evaluation) and the POSSUM (Physiological and Operative Severity Score forenUmeration of Mortality and morbidity) scores have been shown to have good predictive value [23][24][25]. A review of common preoperative tools has shown that they have comparable predictive performance to machine learning (ML) techniques [26]. However, these tools are not consistently employed in practice. Lack of time and trust in the accuracy of measurements has frequently been reported by clinicians as a barrier to the implementation of risk calculators [27]. They present issues in that they can be open to subjectivity and sometimes require the input of variables that are not available in the preoperative period [25][28]. Further, the majority were originally developed with evidence that predates the last three decades of research [23][24][25].
Functional capacity assessment is a measure that aims to quantify the ability of a patient to undertake activities from a free-living environment that need ’sustained aerobic metabolism’ [29]. Much research has identified the association between a higher functional capacity and a reduction in postoperative complications [30][31][32]. The 6-min walk test is a common exercise tolerance test but lacks accuracy [33]. In comparison, cardiopulmonary exercise testing (CPET) is considered the current gold standard for preoperative assessment. CPET is a non-invasive clinical tool that evaluates cardio-respiratory function to measure exercise capacity [34]. In the clinic, patients undergo an exercise test on a cycle-ergometer or a treadmill whilst ventilation and respiratory gas parameters are measured [35]. Multiple studies have been shown to support its use as a tool to identify patients at increased risk of developing postoperative complications following general surgery [36][37]. Although CPET is a proven tool for risk stratification and is routinely implemented, there are several barriers to CPET being accessible and precise. CPET requires trained specialists to complete testing with ready access to dedicated facilities; in 2018, only 53% of Trusts in the UK offered the service [38]. Further, CPET is an expensive test with costs estimated at £289 per unit of testing in 2018/2019 (NHS Improvement, 2019). Although the test measures direct oxygen consumption, there can be considerable subjectivity with one study reporting possible miss-classification of outcomes in up to 60% of tests completed [39]. Finally, CPET might be contraindicated meaning that patients who are at high risk of complications are not always able to achieve a representative score, or even complete the test [40]. Wearable technology has been proposed as a tool that can overcome some of the barriers that are common in these preoperative assessment tools.
1.2. Wearable Sensors
The development of technologies in wearable sensors (WS) in the last decade has led to a significant increase in consumer uptake [41]. As a result, there is a vast quantity of data relating to individuals’ health whilst in free-living environments. There are also many examples of WS being implemented in a clinical setting as a cost-effective tool to measure physiological signals [42]. There is evidence to suggest that these devices could hold a vast volume of data that can give clinicians a quantitative representation of patients’ health in their day-to-day environment [43].
WS have multiple attributes that make them a suitable tool for preoperative assessment. Physiological signals have inherent biological variation and therefore, recording these signals over a longer time period may allow detection of abnormalities that present at irregular time periods [44][45]. A further advantage of collecting data over a longer time period is that the data may be more representative of normal routines. When collecting physical activity data, an increase in the number of days recorded is associated with a more reliable weekly estimate [46][47]. WS are usually autonomous devices that can record signals away from the clinic. This can provide a simpler alternative for clinicians who, under time constraints, cannot always complete preoperative physical assessments [27][48]. In some cases, measurements recorded away from the clinical environment may be more accurate; the ’White-coat’ effect describes the increases in physiological measurements that are only seen when taking measurements in the clinical environment [49]. These attributes have led to multiple successful implementations of WS for diagnostics.
WS have high efficacy for continuous monitoring of numerous physiological variables [50]. Subsequently, this has been shown to be applicable to support the diagnosis of several diseases including Parkinson’s, kidney failure and viral infections [51][52][53]. Particularly in the case of cardiovascular disease monitoring, WS can provide live monitoring capabilities of patients’ medical status that can be used to alert clinicians [54][55]. In the postoperative period, wearable technology has shown consistent uptake and to be a particularly useful tool for monitoring recovery [56]. WS have been used to identify post-surgical cancer patients who are recovering slower than their predicted profile, this facilitates the determination of appropriate discharge dates and preventing re-admissions [57]. A wide range of wearable sensing technology has been shown to be useful for clinicians in the postoperative setting including chest patches and wrist-based fitness sensors [58][59][60][61]. In the preoperative period, initial research has reported similar successful applications of WS.
Some research reports utilising WS as a method to measure adherence to prehabilitation programmes rather than as a preoperative risk assessment tool [62][63]. In other cases, WS have been utilised specifically for preoperative assessment with an exclusive focus on accelerometer data [64][65]. More recently, there have been instances where research has combined Heart Rate (HR) data with accelerometer data to approximate outcomes of cardiovascular fitness testing [40][66].
2. Pre-Processing of Signals
Pre-processing involves all changes to data that are made in order to prepare the data for analysis. Pre-processing can be the most vital stage in data processing and has a large impact on the inferences that can be made from a data set. Wearable data, even when collected in a controlled clinical environment, often requires heavy pre-processing due to the nature of the data. There are two main challenges in WS data that pre-processing aims to overcome: missing data and noise.
2.1. Missing Data
Missing data is a frequently reported problem across research involving WS, particularly when using data from free-living environments [67]. Poor electrode placement, poor contact with skin or removal of device might lead to significant portions of poor quality or missing data. Often, the underlying reasons for periods of missing data are unknown. The prevalence of missing data in WS used in the preoperative period is outlined.
There is a wide variety of missing data reported across studies using wearable sensors in the preoperative period. Missing data was frequently reported at ranges of up to 25% from WS in this context [68][69][70]. One study reported that across all accumulative days of collected data, only 0.25% of days had complete HR data [69]. For the majority of research, the reporting of missing data refers to HR rate, rather than movement data. The reporting of missing data differed between research; some researchers report the overall percentages of data that were missing whilst others report the number of participants excluded due to missing data [40]. In both of these cases, research rarely goes into detail as to the causes of missing periods and how to categorise these. Missing data can generally be classified into three separate categories: missing completely at random (MCAR) where no systematic relationship is present between values that are missing and existing values; missing at random (MAR) where missing data is systematically related to existing data that has been observed but not unobserved data and missing not at random (MNAR) where missing data is systematically related to unobserved data [71]. Depending on the category of missing data that is assumed for the data, different methods may be better suited for minimising the potential bias that may be introduced [72].
Across research applicable to the preoperative period, three different strategies for handling missing periods of data were employed. As seen in Figure 3, missing periods of data were either deleted entirely, tolerated or imputed. These techniques have been previously identified in research using WS and are common solutions for missing data across fields [71][73].
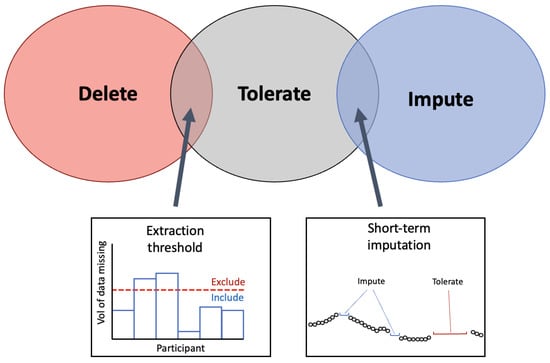
Figure 3. Venn-diagram to present the common methods for handling missing data from WS. The three techniques identified in the literature for handling the missing periods of data are presented in the Venn diagram. At the intersection between ‘delete’ and ‘tolerate’ the implementation of an extraction threshold was identified to delete data below the threshold and tolerate missing data above the threshold. At the intersection between ‘tolerate’ and ‘impute’, imputation on short-term segments of missing periods was identified as a solution that employs that imputation on select segments.
2.1.1. Extraction Threshold
The extraction threshold identifies a point at which a subject’s data will be included in final analyses or is abandoned/processed further. This extraction threshold is usually only applied to wearable devices that measure HR in some format. For research that only utilised the pre-extracted step count, it is not possible to assess the exact volume of missing data. Step count data can appear as null values and still represent viable recordings indicating sedentary periods and so it is not always obvious to know whether this is as a result of non-wear, device malfunction or sedentary behaviour [74]. This is particularly true when step-count is only reported at the daily level [75][76][77].
These extraction thresholds differ widely between research. One study set a daily yield extraction threshold at a minimum of 8 hours of collected data for that day to be included in analysis [69]. Other research set their extraction threshold at 10%, defining that any day with data of a daily yield above 10% would be included for analysis [68]. These studies indicate that the daily extraction threshold can be set at a relatively low value to allow for a high level of missingness in data and prevent this data from being abandoned. Research that used large data sets could set their extraction thresholds at a higher level; one study with over 80,000 participants only selected participants that had a minimum daily yield of 20 h [66]. However, this study did not report what percentage of participants had to be excluded as a result. Large data sets may have more flexibility in their extraction thresholds whilst a small research study may have to accept a higher level of missingness in order to prevent excluding a large portion of their sample.
A total yield extraction threshold can also be applied to the number of days in the monitoring period that have data [70]. This can be employed by only including participants that have above x number of days of data, with x indicating the threshold. The employment of a daily extraction threshold (i.e., 8 h of data) versus an extraction threshold for total data yield (i.e., 3 days of data needed) will depend on whether the data are subdivided into daily segments or kept as a total per participant.
3.1.2. Selecting an Extraction Threshold
Extraction thresholds should not be randomly selected. To investigate the influence of the extraction threshold on the predictive performance of analysis, one study varied their extraction threshold from 1 to 10 h and identified that between 8 and 10 h achieves the best performance [69]. This highlights the importance of identifying an optimal extraction threshold. Setting a high threshold for inclusion will result in less data available for analysis; a low threshold has the potential to allow data from days with large missing periods into analysis. If this is the case then the underlying reasons for missing periods should be assessed to prevent bias in the data.
Aside from reported extraction thresholds within their own data sets, very little research has focused on quantifying the volume of data that is needed to obtain reliable preoperative baseline measurements. It has been reported that when using a PPG sensor combined with an accelerometer, a minimum of three days of monitoring should be completed; however, an extraction threshold within each day was not specified and whether the location and type of sensors have an impact on this threshold was not discussed [78]. An appropriate extraction threshold is a useful tool for selecting data for analysis but does not provide a solution to missing periods. To overcome the missing periods of data that remain, several imputation methods can be employed.
2.1.3. Imputation
Data imputation in WS data is a complex process. Individuals will often have varying levels of missingness between them due to compliance with wearing the device. Further, there may be missing portions caused by technical issues in a device. Therefore, imputation techniques in WS data should generalise to both the participants’ behaviour and the device’s patterns [79]. Often in research collecting data in the preoperative period, data that was identified as missing was abandoned. Little effort is made to impute the missing values and to investigate why they are missing; this could reduce the size of the data sample and in some cases may introduce bias [80]. The imputation techniques that were employed in the research are outlined in the sections below.
The simplest method to replace missing data points in HR signals is with the mean HR values of activities at waking periods [81]. However, if the mechanism for missing portions is known to occur during sedentary periods or periods of vigorous activity then this may lead to under or over-estimations of daily HR. One particular study substituted missing HR values for HR recorded during a hospital visit [82]. This technique was not common across research, likely due to inconsistencies that may be present between free-living data and data collected in-clinic. For the studies that utilised the temporal aspects of data to employ imputation, they both did this using a two-layered pipeline [68][69].
The k-nearest neighbours (KNN) technique was shown to be a common method to impute missing HR values [68][69]. KNN has previously been implemented as a technique to address missing data in a range of applications [83]. The KNN algorithm is implemented as a ’sliding window’ that allows missing HR data to be calculated from a combination of recent step count and HR data [68]. This method is rationalised by explaining that imputation is useful for short-term missing segments where previous values of step count and HR have a high correlation with future values. One technique employed a k-nearest neighbours (KNN) algorithm for an entire day of data if the daily yield for the relevant day was above 10% [68]. A different study utilised the same technique but for all portions of missing data that were shorter than 10 min long, regardless of daily yield. If the segments of missing data were less than 10 min, a KNN sliding window (length of 5) utilised recent HR and step counts to predict HR values [69], see Figure 4. Using this method, the feature vector is imputed to the KNN algorithm where hrt and stept represent HR and step data at time t.
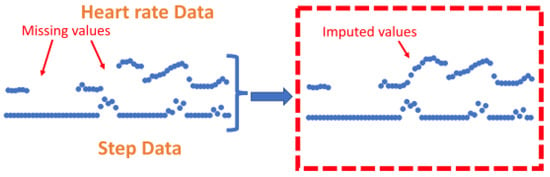
Figure 4. Figure to show imputation using K-nearest-neighbours. Zhang et al. (2023) utilise the KNN technique to impute on short-term segments of missing data under 10 min in length by utilising previous values from both the step count and heart rate signals to calculate missing values. This figure was produced by Zhang et al. (2023) and was taken from a larger figure but had no changes made, taken as part of the Creative Commons Attribution International 4.0 License [69][84].
To assess the performance of various imputation techniques, several metrics can be employed. Root Mean Square Error (RMSE) is a commonly used metric for assessing imputation in signals [79][85]. RMSE measures the average magnitude of the errors of the imputed values. It is particularly useful for assessing imputation because it penalises larger errors more heavily making it especially sensitive to values that are big outliers from the predicted values. Mean Absolute Error (MAE) provides an alternative to the RMSE in that it is not sensitive to outliers. It presents the absolute differences between the imputed and original values and is focused on the overall accuracy of the algorithm. It may be useful to compare the outcomes of the MAE with the RMSE and the two have previously been used in combination [79]. For the MAE and RMSE, lower values indicate better performance. However, in order to assess imputation techniques using these metrics, ground truth values are needed. One method to do this is to add missing periods of data into a signal and perform imputation on these fabricated missing periods to compare outputs against original values as ground truths. It should be noted that this has been very rarely implemented in research across this field.
2.1.4. Feature Level Imputation
In instances where data has been abandoned due to significant periods of missing data, this can be imputed by employing feature-level imputation techniques. After abandoning days with a daily yield below the extraction threshold, a feature-level imputation technique can be employed to compute the features that represent the days with high portions of missing periods. In one case, researchers again utilise the KNN method to impute statistical and semantic features based on the neighbouring features that are available for that participant, rather than attempting to impute the missing values in the signal [68]. A further technique to deal with missing data that fell below the daily yield of 8 h was to employ imputation on high-level features that have been calculated from daily features [69]. Further application of Detrended Fluctuation Analysis was used to reduce the incomplete data.
It is important to note that research only employed imputation for HR data, this was not performed for other features extracted from accelerometer data. For research where HR signals are collected alongside step count data, the proportion of missing step count data can be extrapolated from the time periods with missing data points of the HR signal. Step count data is reported as being significantly less correlated and so less predictable than HR data [69]. Instead, these data were normalised by dividing the step count by the daily yield so as to prevent the step count from being drastically increased just for those patients with more data accumulated.
2.2. Noise
Aside from missing data in the signal, noise can also prevent meaningful features from being extracted. Accelerometry data can be plagued by white noise, altered by human motion or vibration whilst both ECG and PPG signals can be corrupted by motion artefact, baseline wonder and electromyography (EMG) noise [86][87]. In certain cases, some removal of noise from signals was completed. Previously, Gaussian process robust regression has shown to be successful for noisy HR data and was implemented by one study to utilise prior knowledge of the HR data to reduce noise [66][88]. In comparison, a simpler method to limit the noise in HR data was to average the HR extracted from R-R intervals over a set time period, this varied from between 15 s to 15 min [89][90]. When employing this technique, all inaccurate HR values were identified and removed from the data where consecutive HR values varied by more than 20% [90]. Cardiac signals were very rarely passed through a low-pass filter; however, one study resampled the HR to 1 Hz before passing HR through a 0.01 Hz low-pass filter to remove high-frequencies affected by non-linearities introduced from circulatory distortions [91].
For accelerometry, to convert the raw signal data into magnitude of acceleration the Euclidean norm minus one and high-passed filtered vector magnitude were used [66]. Altini et al. (2016) employed a different filter technique where a low-pass filter (1Hz) was used to isolate the static component in the signal due to gravity and a band-pass filter (0.1 Hz, 10 Hz) was used to isolate dynamic components due to body noise [90]. As mentioned above, Beltrame et al. (2017) used a similar low-pass filter at 0.01 Hz for accelerometer as well as HR data [91]. The only implementation of a fast Fourier transformation (FFT) was to integrate the frequency in accelerometer data between 1 Hz and 10 Hz [92]. One particular paper reports a method for outlier detection within data by removing values that are greater than 3 standard deviations from the mean [93]. Building on the techniques commonly employed on HR data by averaging values over a short period, research employing a pedometer categorised each accelerometer period of 10 s into either lying, stationary or active periods [92].
For research using large-scale cohort data, after normalising their data through standard scaling with unit variance, researchers applied Principle Component Analysis (PCA) onto the original training data set that retained the components that explained 99.9% of variance [94]. To prevent any information leakage across the data sets, the fitted PCA scaler was applied individually to the test set. In a different project utilising the same large dataset, researchers attempted to reduce the noise that is seen in the labelling of HR data from the ECG wearable using deep learning [89]. The authors propose UDAMA (Unsupervised Domain Adaptation and Multi-discriminator Adversarial) training network [66]. However, these techniques utilising deep learning will require a large pool of data and may not be suitable for smaller single-centre studies. In order to reduce the noise that is present in daily features, one research study utilised singular spectrum analysis to further extract high-level features from daily features [69]. This allows trends to be extracted from the noisy data with missing portions by computing the mean, variance and slope from each time series of daily features.
2.3. Encoding Time
The temporal aspect of the HR and accelerometer data can provide useful insights but is infrequently used in analysis. To investigate the temporal aspect or reduce the bias that can be related to the time of recordings, it is possible to encode timestamps from sensors [66][94]. This is performed to help capture any periodic nature of certain behaviours, particularly those that may exhibit daily or monthly habits. By incorporating these cyclical components the model can better understand the cyclical nature of time. This was completed by encoding either the month of the year or hour of the day as (x, y) co-ordinates on a circle using Equations (1) and (2) where t represents the temporal aspect.

This is to ensure that when including time in analyses neighbouring timestamps are always consistent; December is only one month from January and 23:59 is only one minute from 00:00. This is particularly important for large data sets that are likely to be collecting data over an extended time period.
References
- Liu, J.H.; Etzioni, D.A.; O’Connell, J.B.; Maggard, M.A.; Ko, C.Y. The Increasing Workload of General Surgery. Arch. Surg. 2004, 139, 423–428.
- Shinji, S.; Yamada, T.; Matsuda, A.; Sonoda, H.; Ohta, R.; Iwai, T.; Takeda, K.; Yonaga, K.; Masuda, Y.; Yoshida, H. Recent Advances in the Treatment of Colorectal Cancer: A Review. J. Nippon Med. Sch. 2022, 89, 246–254.
- Brunner, M.; Wu, Z.; Krautz, C.; Pilarsky, C.; Grützmann, R.; Weber, G.F. Current Clinical Strategies of Pancreatic Cancer Treatment and Open Molecular Questions. Int. J. Mol. Sci. 2019, 20, 4543.
- Orditura, M.; Galizia, G.; Sforza, V.; Gambardella, V.; Fabozzi, A.; Laterza, M.M.; Andreozzi, F.; Ventriglia, J.; Savastano, B.; Mabilia, A.; et al. Treatment of gastric cancer. World J. Gastroenterol. Wjg 2014, 20, 1635.
- World Cancer Research Fund. Colorectal Cancer Statistics; World Cancer Research Fund: London, UK, 2023.
- Cutsem, E.V.; Borràs, J.M.; Castells, A.; Ciardiello, F.; Ducreux, M.; Haq, A.; Schmoll, H.J.; Tabernero, J. Improving outcomes in colorectal cancer: Where do we go from here? Eur. J. Cancer 2013, 49, 2476–2485.
- Cancer Research UK. Bowel Cancer; Cancer Research UK: London, UK, 2023.
- Morris, E.J.; Taylor, E.F.; Thomas, J.D.; Quirke, P.; Finan, P.J.; Coleman, M.P.; Rachet, B.; Forman, D. Thirty-day postoperative mortality after colorectal cancer surgery in England. Gut 2011, 60, 806–813.
- Wells, C.I.; Varghese, C.; Boyle, L.J.; McGuinness, M.J.; Keane, C.; O’Grady, G.; Gurney, J.; Koea, J.; Harmston, C.; Bissett, I.P. “Failure to Rescue” following Colorectal Cancer Resection: Variation and Improvements in a National Study of Postoperative Mortality. Ann. Surg. 2023, 278, 87–95.
- Ketelaers, S.H.; Orsini, R.G.; Burger, J.W.; Nieuwenhuijzen, G.A.; Rutten, H.J. Significant improvement in postoperative and 1-year mortality after colorectal cancer surgery in recent years. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2019, 45, 2052–2058.
- Silva, S.D.; Ma, C.; Proulx, M.C.; Crespin, M.; Kaplan, B.S.; Hubbard, J.; Prusinkiewicz, M.; Fong, A.; Panaccione, R.; Ghosh, S.; et al. Postoperative Complications and Mortality Following Colectomy for Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2011, 9, 972–980.
- Alves, A.; Panis, Y.; Mathieu, P.; Mantion, G.; Kwiatkowski, F.; Slim, K. Postoperative Mortality and Morbidity in French Patients Undergoing Colorectal Surgery: Results of a Prospective Multicenter Study. Arch. Surg. 2005, 140, 278–283.
- Tevis, S.E.; Kennedy, G.D. Postoperative complications and implications on patient-centered outcomes. J. Surg. Res. 2013, 181, 106.
- Wick, E.C.; Shore, A.D.; Hirose, K.; Ibrahim, A.M.; Gearhart, S.L.; Efron, J.; Weiner, J.P.; Makary, M.A. Readmission rates and cost following colorectal surgery. Dis. Colon Rectum 2011, 54, 1475–1479.
- Louis, M.; Johnston, S.A.; Churilov, L.; Ma, R.; Christophi, C.; Weinberg, L. Financial burden of postoperative complications following colonic resection: A systematic review. Medicine 2021, 100, e26546.
- Ludbrook, G.L. The Hidden Pandemic: The Cost of Postoperative Complications. Curr. Anesthesiol. Rep. 2022, 12, 1–9.
- Zambouri, A. Preoperative evaluation and preparation for anesthesia and surgery. Hippokratia 2007, 11, 13.
- Royal College of Physicians Developed by the National Guideline Centre. Preoperative Tests (Update) Routine Preoperative Tests for Elective Surgery; National Guideline Centre UK: London, UK, 2016.
- Grocott, M.P.; Pearse, R.M. Perioperative medicine: The future of anaesthesia? Bja Br. J. Anaesth. 2012, 108, 723–726.
- Grocott, M.P.; Edwards, M.; Mythen, M.G.; Aronson, S. Peri-operative care pathways: Re-engineering care to achieve the ‘triple aim’. Anaesthesia 2019, 74, 90–99.
- Noordzij, P.G.; Boersma, E.; Bax, J.J.; Feringa, H.H.; Schreiner, F.; Schouten, O.; Kertai, M.D.; Klein, J.; Urk, H.V.; Elhendy, A.; et al. Prognostic Value of Routine Preoperative Electrocardiography in Patients Undergoing Noncardiac Surgery. Am. J. Cardiol. 2006, 97, 1103–1106.
- Vernooij, J.E.; Koning, N.J.; Geurts, J.W.; Holewijn, S.; Preckel, B.; Kalkman, C.J.; Vernooij, L.M. Performance and usability of pre-operative prediction models for 30-day peri-operative mortality risk: A systematic review. Anaesthesia 2023, 78, 607–619.
- Wagner, D.P.; Draper, E.A. Acute physiology and chronic health evaluation (APACHE II) and Medicare reimbursement. Health Care Financ. Rev. 1984, 1984, 91.
- Jones, H.J.S.; Cossart, L.D. Risk scoring in surgical patients. Br. J. Surg. 1999, 86, 149–157.
- Copeland, G.P. The POSSUM System of Surgical Audit. Arch. Surg. 2002, 137, 15–19.
- Dosis, A.; Helliwell, J.; Syversen, A.; Tiernan, J.; Zhang, Z.; Jayne, D. Estimating postoperative mortality in colorectal surgery—A systematic review of risk prediction models. Int. J. Color. Dis. 2023, 38, 155.
- Pradhan, N.; Dyas, A.R.; Bronsert, M.R.; Lambert-Kerzner, A.; Henderson, W.G.; Qiu, H.; Colborn, K.L.; Mason, N.J.; Meguid, R.A. Attitudes about use of preoperative risk assessment tools: A survey of surgeons and surgical residents in an academic health system. Patient Saf. Surg. 2022, 16, 13.
- Goffi, L.; Saba, V.; Ghiselli, R.; Necozione, S.; Mattei, A.; Carle, F. Preoperative APACHE II and ASA scores in patients having major general surgical operations: Prognostic value and potential clinical applications. Eur. J. Surg. Acta Chir. 1999, 165, 730–735.
- Arena, R.; Myers, J.; Williams, M.A.; Gulati, M.; Kligfield, P.; Balady, G.J.; Collins, E.; Fletcher, G. Assessment of Functional Capacity in Clinical and Research Settings. Circulation 2007, 116, 329–343.
- Ferreira, V.; Lawson, C.; Ekmekjian, T.; Carli, F.; Scheede-Bergdahl, C.; Chevalier, S. Effects of preoperative nutrition and multimodal prehabilitation on functional capacity and postoperative complications in surgical lung cancer patients: A systematic review. Support. Care Cancer 2021, 29, 5597–5610.
- Mayo, N.E.; Feldman, L.; Scott, S.; Zavorsky, G.; Kim, D.J.; Charlebois, P.; Stein, B.; Carli, F. Impact of preoperative change in physical function on postoperative recovery: Argument supporting prehabilitation for colorectal surgery. Surgery 2011, 150, 505–514.
- Makker, P.G.S.; Koh, C.E.; Solomon, M.J.; Steffens, D.; BMedSc, P.G.S.M.; MBBS, C.E.K.; BCH, M.J.S.M.; BPhyt, D.S. Preoperative functional capacity and postoperative outcomes following abdominal and pelvic cancer surgery: A systematic review and meta-analysis. Anz J. Surg. 2022, 92, 1658–1667.
- Silvapulle, E.; Darvall, J. Objective methods for preoperative assessment of functional capacity. Bja Educ. 2022, 22, 312–320.
- Levett, D.Z.; Jack, S.; Swart, M.; Carlisle, J.; Wilson, J.; Snowden, C.; Riley, M.; Danjoux, G.; Ward, S.A.; Older, P.; et al. Perioperative cardiopulmonary exercise testing (CPET): Consensus clinical guidelines on indications, organization, conduct, and physiological interpretation. Br. J. Anaesth. 2018, 120, 484–500.
- Albouaini, K.; Egred, M.; Alahmar, A.; Wright, D.J. Cardiopulmonary exercise testing and its application. Heart 2007, 93, 1285.
- Hennis, P.J.; Meale, P.M.; Grocott, M.P. Cardiopulmonary exercise testing for the evaluation of perioperative risk in non-cardiopulmonary surgery. Postgrad. Med. J. 2011, 87, 550–557.
- Levett, D.Z.; Grocott, M.P. Cardiopulmonary exercise testing for risk prediction in major abdominal surgery. Anesthesiol. Clin. 2015, 33, 1–16.
- Reeves, T.; Bates, S.; Sharp, T.; Richardson, K.; Bali, S.; Plumb, J.; Anderson, H.; Prentis, J.; Swart, M.; Levett, D.Z.H. Cardiopulmonary exercise testing (CPET) in the United Kingdom-a national survey of the structure, conduct, interpretation and funding. Perioper. Med. 2018, 7, 2.
- Rose, G.A.; Davies, R.G.; Appadurai, I.R.; Williams, I.M.; Bashir, M.; Berg, R.M.; Poole, D.C.; Bailey, D.M. ‘Fit for surgery’: The relationship between cardiorespiratory fitness and postoperative outcomes. Exp. Physiol. 2022, 107, 787–799.
- Jones, L.; Tan, L.; Carey-Jones, S.; Riddell, N.; Davies, R.; Brownsdon, A.; Kelson, M.; Williams-Thomas, R.; Busse, M.; Davies, M.M.; et al. Can wearable technology be used to approximate cardiopulmonary exercise testing metrics? Perioper. Med. 2021, 10, 9.
- Ferreira, J.J.; Fernandes, C.I.; Rammal, H.G.; Veiga, P.M. Wearable technology and consumer interaction: A systematic review and research agenda. Comput. Hum. Behav. 2021, 118, 106710.
- Vijayan, V.; Connolly, J.; Condell, J.; McKelvey, N.; Gardiner, P. Review of Wearable Devices and Data Collection Considerations for Connected Health. Sensors 2021, 21, 5589.
- Smuck, M.; Odonkor, C.A.; Wilt, J.K.; Schmidt, N.; Swiernik, M.A. The emerging clinical role of wearables: Factors for successful implementation in healthcare. npj Digit. Med. 2021, 4, 45.
- Ontario, H.Q. Long-Term Continuous Ambulatory ECG Monitors and External Cardiac Loop Recorders for Cardiac Arrhythmia: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2017, 17, 1–56.
- Turakhia, M.P.; Hoang, D.D.; Zimetbaum, P.; Miller, J.D.; Froelicher, V.F.; Kumar, U.N.; Xu, X.; Yang, F.; Heidenreich, P.A. Diagnostic Utility of a Novel Leadless Arrhythmia Monitoring Device. Am. J. Cardiol. 2013, 112, 520–524.
- Yao, J.; Tan, C.S.; Lim, N.; Tan, J.; Chen, C.; Müller-Riemenschneider, F. Number of daily measurements needed to estimate habitual step count levels using wrist-worn trackers and smartphones in 212,048 adults. Sci. Rep. 2021, 11, 9633.
- Ricardo, L.I.C.; Wendt, A.; Galliano, L.M.; Muller, W.D.A.; Cruz, G.I.N.; Wehrmeister, F.; Brage, S.; Ekelund, U.; Silva, I.C.M. Number of days required to estimate physical activity constructs objectively measured in different age groups: Findings from three Brazilian (Pelotas) population-based birth cohorts. PLoS ONE 2020, 15, e0216017.
- Böhmer, A.B.; Wappler, F.; Zwilßer, B. Preoperative Risk Assessment—From Routine Tests to Individualized Investigation. Dtsch. Ärzteblatt Int. 2014, 111, 437.
- Lequeux, B.; Uzan, C.; Rehman, M.B. Does resting heart rate measured by the physician reflect the patient’s true resting heart rate? White-coat heart rate. Indian Heart J. 2018, 70, 93–98.
- Deshmukh, S.D.; Shilaskar, S.N. Wearable sensors and patient monitoring system: A Review. In Proceedings of the 2015 International Conference on Pervasive Computing (ICPC), Pune, India, 8–10 January 2015; pp. 1–3.
- Maetzler, W.; Domingos, J.; Srulijes, K.; Ferreira, J.J.; Bloem, B.R. Quantitative wearable sensors for objective assessment of Parkinson’s disease. Mov. Disord. 2013, 28, 1628–1637.
- Promphet, N.; Hinestroza, J.P.; Rattanawaleedirojn, P.; Soatthiyanon, N.; Siralertmukul, K.; Potiyaraj, P.; Rodthongkum, N. Cotton thread-based wearable sensor for non-invasive simultaneous diagnosis of diabetes and kidney failure. Sens. Actuators Chem. 2020, 321, 128549.
- Quer, G.; Radin, J.M.; Gadaleta, M.; Baca-Motes, K.; Ariniello, L.; Ramos, E.; Kheterpal, V.; Topol, E.J.; Steinhubl, S.R. Wearable sensor data and self-reported symptoms for COVID-19 detection. Nat. Med. 2020, 27, 73–77.
- Kakria, P.; Tripathi, N.K.; Kitipawang, P. A real-time health monitoring system for remote cardiac patients using smartphone and wearable sensors. Int. J. Telemed. Appl. 2015, 2015, 373474.
- Huang, J.D.; Wang, J.; Ramsey, E.; Leavey, G.; Chico, T.J.A.; Huang, J.D.; Wang, J.; Ramsey, E.; Leavey, G.; Chico, T.J.A.; et al. Applying Artificial Intelligence to Wearable Sensor Data to Diagnose and Predict Cardiovascular Disease: A Review. Sensors 2022, 22, 8002.
- Wells, C.I.; Xu, W.; Penfold, J.A.; Keane, C.; Gharibans, A.A.; Bissett, I.P.; O’Grady, G. Wearable devices to monitor recovery after abdominal surgery: Scoping review. BJS Open 2022, 6, zrac031.
- van den Eijnden, M.A.C.; van der Stam, J.A.; Bouwman, R.A.; Mestrom, E.H.J.; Verhaegh, W.F.J.; van Riel, N.A.W.; Cox, L.G.E. Machine Learning for Postoperative Continuous Recovery Scores of Oncology Patients in Perioperative Care with Data from Wearables. Sensors 2023, 23, 4455.
- Daskivich, T.J.; Houman, J.; Lopez, M.; Luu, M.; Fleshner, P.; Zaghiyan, K.; Cunneen, S.; Burch, M.; Walsh, C.; Paiement, G.; et al. Association of Wearable Activity Monitors With Assessment of Daily Ambulation and Length of Stay Among Patients Undergoing Major Surgery. JAMA Netw. Open 2019, 2, e187673.
- Esteban, P.A.; Hernández, N.; Novoa, N.; Varela, G. Evaluating patients’ walking capacity during hospitalization for lung cancer resection. Interact. Cardiovasc. Thorac. Surg. 2017, 25, 268–271.
- Rinne, J.K.; Miri, S.; Oksala, N.; Vehkaoja, A.; Kössi, J. Evaluation of a wrist-worn photoplethysmography monitor for heart rate variability estimation in patients recovering from laparoscopic colon resection. J. Clin. Monit. Comput. 2023, 37, 45–53.
- Breteler, M.J.; Huizinga, E.; Loon, K.V.; Leenen, L.P.; Dohmen, D.A.; Kalkman, C.J.; Blokhuis, T.J. Reliability of wireless monitoring using a wearable patch sensor in high-risk surgical patients at a step-down unit in the Netherlands: A clinical validation study. BMJ Open 2018, 8, e020162.
- Waller, E.; Sutton, P.; Rahman, S.; Allen, J.; Saxton, J.; Aziz, O. Prehabilitation with wearables versus standard of care before major abdominal cancer surgery: A randomised controlled pilot study (trial registration: NCT04047524). Surg. Endosc. 2022, 36, 1008.
- Beilstein, C.M.; Krutkyte, G.; Vetsch, T.; Eser, P.; Wilhelm, M.; Stanga, Z.; Bally, L.; Verra, M.; Huber, M.; Wuethrich, P.Y.; et al. Multimodal prehabilitation for major surgery in elderly patients to lower complications: Protocol of a randomised, prospective, multicentre, multidisciplinary trial (PREHABIL Trial). BMJ Open 2023, 13, e070253.
- Feeney, C.; Reynolds, J.V.; Hussey, J. Preoperative physical activity levels and postoperative pulmonary complications post-esophagectomy. Dis. Esophagus 2011, 24, 489–494.
- Greco, M.; Angelucci, A.; Avidano, G.; Marelli, G.; Canali, S.; Aceto, R.; Lubian, M.; Oliva, P.; Piccioni, F.; Aliverti, A.; et al. Wearable Health Technology for Preoperative Risk Assessment in Elderly Patients: The WELCOME Study. Diagnostics 2023, 13, 630.
- Spathis, D.; Perez-Pozuelo, I.; Brage, S.; Wareham, N.J.; Mascolo, C. Self-supervised transfer learning of physiological representations from free-living wearable data. In Proceedings of the ACM CHIL 2021–2021 ACM Conference on Health, Inference, and Learning, Virtual, 8–9 April 2021; Volume 21, pp. 69–78.
- Cho, S.; Ensari, I.; Weng, C.; Kahn, M.G.; Natarajan, K. Factors Affecting the Quality of Person-Generated Wearable Device Data and Associated Challenges: Rapid Systematic Review. Jmir Mhealth Uhealth 2021, 9, e20738.
- Cos, H.; Li, D.; Williams, G.; Chininis, J.; Dai, R.; Zhang, J.; Srivastava, R.; Raper, L.; Sanford, D.; Hawkins, W.; et al. Predicting Outcomes in Patients Undergoing Pancreatectomy Using Wearable Technology and Machine Learning: Prospective Cohort Study. J. Med. Internet Res. 2021, 23, e23595.
- Zhang, J.; Li, D.; Dai, R.; Cos, H.; Williams, G.A.; Raper, L.; Hammill, C.W.; Lu, C. Predicting Post-Operative Complications with Wearables. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2022, 6, 1–27.
- Haveman, M.E.; van Melzen, R.; Schuurmann, R.C.; Hermens, H.J.; Tabak, M.; de Vries, J.P.P. Feasibility and patient’s experiences of perioperative telemonitoring in major abdominal surgery: An observational pilot study. Expert Rev. Med. Devices 2022, 19, 515–523.
- Little, R.J.; Rubin, D.B. Statistical Analysis with Missing Data; John Wiley & Sons.: Hoboken, NJ, USA, 2019; pp. 1–449.
- Jakobsen, J.C.; Gluud, C.; Wetterslev, J.; Winkel, P. When and how should multiple imputation be used for handling missing data in randomised clinical trials—A practical guide with flowcharts. BMC Med. Res. Methodol. 2017, 17, 162.
- Darji, J.; Biswas, N.; Jones, L.D.; Ashili, S. Handling missing data in the time-series data from wearables. In Time Series Analysis—Recent Advances, New Perspectives and Applications ; IntechOpen: London, UK, 2023.
- Tackney, M.S.; Cook, D.G.; Stahl, D.; Ismail, K.; Williamson, E.; Carpenter, J. A framework for handling missing accelerometer outcome data in trials. Trials 2021, 22, 379.
- Sun, V.; Dumitra, S.; Ruel, N.; Lee, B.; Melstrom, L.; Melstrom, K.; Woo, Y.; Sentovich, S.; Singh, G.; Fong, Y. Wireless Monitoring Program of Patient-Centered Outcomes and Recovery Before and after Major Abdominal Cancer Surgery. JAMA Surg. 2017, 152, 852–859.
- Billé, A.; Buxton, J.; Viviano, A.; Gammon, D.; Veres, L.; Routledge, T.; Harrison-Phipps, K.; Dixon, A.; Minetto, M.A. Preoperative Physical Activity Predicts Surgical Outcomes Following Lung Cancer Resection. Integr. Cancer Ther. 2021, 20, 1534735420975853.
- Richards, S.J.G.; Jerram, P.M.; Brett, C.; Falloon, M.; Frizelle, F.A. The association between low pre-operative step count and adverse post-operative outcomes in older patients undergoing colorectal cancer surgery. Perioper. Med. 2020, 9, 20.
- Haveman, M.E.; van Melzen, R.; Moumni, M.E.; Schuurmann, R.C.L.; Hermens, H.J.; Tabak, M.; de Vries, J.P.P.M. Determining the Reliable Measurement Period for Preoperative Baseline Values With Telemonitoring Before Major Abdominal Surgery: Pilot Cohort Study. Jmir Perioper. Med. 2022, 5, e40815.
- Lin, S.; Wu, X.; Martinez, G.; Chawla, N.V. Filling missing values on wearable-sensory time series data. In Proceedings of the 2020 SIAM International Conference on Data Mining, Cincinnati, OH, USA, 7–9 May 2020; pp. 46–54.
- Lin, J.Y.; Lu, Y.; Tu, X. How to avoid missing data and the problems they pose: Design considerations. Shanghai Arch. Psychiatry 2012, 24, 181.
- Hallgrímsson, H.T.; Jankovic, F.; Althoff, T.; Allen, P.G.; Foschini, L. Learning Individualized Cardiovascular Responses from Large-scale Wearable Sensors Data. arXiv 2018, arXiv:1812.01696.
- Angelucci, A.; Greco, M.; Canali, S.; Marelli, G.; Avidano, G.; Goretti, G.; Cecconi, M.; Aliverti, A. Fitbit Data to Assess Functional Capacity in Patients Before Elective Surgery: Pilot Prospective Observational Study. J. Med. Internet Res. 2023, 25, e42815.
- Meesad, P.; Hengpraprohm, K. Combination of KNN-based feature selection and KNN-based missing-value imputation of microarray data. In Proceedings of the 3rd International Conference on Innovative Computing Information and Control, ICICIC’08, Dalian, China, 18–20 June 2008.
- Commons, C. CC BY 4.0 Deed. Available online: https://creativecommons.org/licenses/by/4.0/ (accessed on 24 November 2023).
- Chakrabarti, S.; Biswas, N.; Karnani, K.; Padul, V.; Jones, L.D.; Kesari, S.; Ashili, S. Binned Data Provide Better Imputation of Missing Time Series Data from Wearables. Sensors 2023, 23, 1454.
- Bashar, S.K.; Ding, E.; Walkey, A.J.; McManus, D.D.; Chon, K.H. Noise Detection in Electrocardiogram Signals for Intensive Care Unit Patients. IEEE Access Pract. Innov. Open Solut. 2019, 7, 88357.
- Kang, S.; Paul, A.; Jeon, G. Reduction of mixed noise from wearable sensors in human-motion estimation. Comput. Electr. Eng. 2017, 61, 287–296.
- Stegle, O.; Fallert, S.V.; MacKay, D.J.; Brage, S. Gaussian process robust regression for noisy heart rate data. IEEE Trans. Bio-Med. Eng. 2008, 55, 2143–2151.
- Wu, Y.; Spathis, D.; Jia, H.; Perez-Pozuelo, I.; Gonzales, T.I.; Brage, S.; Wareham, N.; Mascolo, C. Turning Silver into Gold: Domain Adaptation with Noisy Labels for Wearable Cardio-Respiratory Fitness Prediction. arXiv 2022, arXiv:2211.10475.
- Altini, M.; Casale, P.; Penders, J.; Amft, O. Cardiorespiratory fitness estimation in free-living using wearable sensors. Artif. Intell. Med. 2016, 68, 37–46.
- Beltrame, T.; Amelard, R.; Wong, A.; Hughson, R.L. Prediction of oxygen uptake dynamics by machine learning analysis of wearable sensors during activities of daily living. Sci. Rep. 2017, 7, 45738.
- Cui, H.W.; Kirby, G.S.; Surmacz, K.; Hargrove, C.; Griffiths, J.; Turney, B.W. The association of pre-operative home accelerometry with cardiopulmonary exercise variables. Anaesthesia 2018, 73, 738–745.
- Dunn, J.; Kidzinski, L.; Runge, R.; Witt, D.; Hicks, J.L.; Rose, S.M.S.F.; Li, X.; Bahmani, A.; Delp, S.L.; Hastie, T.; et al. Wearable sensors enable personalized predictions of clinical laboratory measurements. Nat. Med. 2021, 27, 1105–1112.
- Spathis, D.; Perez-Pozuelo, I.; Gonzales, T.I.; Wu, Y.; Brage, S.; Wareham, N.; Mascolo, C. Longitudinal cardio-respiratory fitness prediction through wearables in free-living environments. npj Digit. Med. 2022, 5, 176.
More
Information
Subjects:
Engineering, Electrical & Electronic; Surgery
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
696
Revisions:
3 times
(View History)
Update Date:
24 Jan 2024
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No