Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Caridad López-Granero | -- | 1178 | 2024-01-16 17:28:41 | | | |
| 2 | Camila Xu | Meta information modification | 1178 | 2024-01-17 02:31:45 | | | | |
| 3 | Camila Xu | + 4 word(s) | 1182 | 2024-01-22 09:55:51 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
López-Granero, C.; Polyanskaya, L.; Ruiz-Sobremazas, D.; Barrasa, A.; Aschner, M.; Alique, M. Etiology and Route of Access of Particulate Matter. Encyclopedia. Available online: https://encyclopedia.pub/entry/53919 (accessed on 26 July 2026).
López-Granero C, Polyanskaya L, Ruiz-Sobremazas D, Barrasa A, Aschner M, Alique M. Etiology and Route of Access of Particulate Matter. Encyclopedia. Available at: https://encyclopedia.pub/entry/53919. Accessed July 26, 2026.
López-Granero, Caridad, Leona Polyanskaya, Diego Ruiz-Sobremazas, Angel Barrasa, Michael Aschner, Matilde Alique. "Etiology and Route of Access of Particulate Matter" Encyclopedia, https://encyclopedia.pub/entry/53919 (accessed July 26, 2026).
López-Granero, C., Polyanskaya, L., Ruiz-Sobremazas, D., Barrasa, A., Aschner, M., & Alique, M. (2024, January 16). Etiology and Route of Access of Particulate Matter. In Encyclopedia. https://encyclopedia.pub/entry/53919
López-Granero, Caridad, et al. "Etiology and Route of Access of Particulate Matter." Encyclopedia. Web. 16 January, 2024.
Copy Citation
The primary origin of particulate matter (PM) is from a combination of industrial activity, internal combustion engines, and geographic and meteorological conditions linked to the increased forest fires.
particulate matter
air quality
elderly
cognitive function
neurodegeneration
1. Introduction
The primary origin of particulate matter (PM) is from a combination of industrial activity, internal combustion engines, and geographic and meteorological conditions linked to the increased forest fires [1]. Specifically, smoke originating from forest fires is primarily responsible for ultrafine particles (UFPM ≤ 100 nm in diameter) [1]. Inspiring such particles increases the risk of developing respiratory diseases, such as tonsillitis, asthma, bronchitis, lung cancer, and cystic fibrosis pneumonia later in life [2].
2. Etiology of Particulate Matter
Air quality is determined by estimating the number of solid matter particles in the air [3]. These particles contribute to the air pollution level and are referred to as PM [4]. PM are partly formed in the atmosphere through chemical reactions that produce inorganic nitrates and sulfates, as well as organic compounds [3]. Inhalable particles are divided into four groups by diameter highlighting three of them: larger than 10 μm (μm), smaller than 10 μm (PM10), and smaller than 2.5 μm (PM2.5) [5]. In addition, a fourth group exists, referred to as ultrafine PM (UFPM or PM0.1, with diameter < 100 nm) [6]. PM2.5 are not visible by the naked eye, and levels of such particles (measured in μg/m3) are not distinguished without specialized equipment when kept at concentrations below 35 μg/m3 [7]. The US EPA, the European Environment Agency (EEA), and the WHO set a PM2.5 safety standard under 12 μg/m3 (annual average) and a 24 h average of 35 μg/m3. Nonetheless, this value is routinely exceeded worldwide (e.g., in large cities in India, China, or Mexico) [6]. Therefore, many countries have failed to keep urban PM pollution levels within WHO guidelines.
PM is mainly derived from road transport, agriculture, power plants, industry, and homes. Outdoor particles are primarily produced from traffic-related activities [6]. PM2.5 is a mixture of harmful chemicals, such as sulfur dioxide, nitrogen dioxide, organic phosphates, and chlorine, which are utilized in agriculture, bisphenol, etc., along with combustion particles, carbon particles, heavy metals, and pollutants from industrial sites and factories. In contrast, PM10 consists mainly of pollen, mold, and dust particles [8][9]. Hence, despite being less visible to the public, <PM2.5 poses much greater health risks than larger particles, and due to their size, with limited efficacy of protective gear, such as masks or respirators, in preventing exposure [3]. UFPM are mostly derived from wildfire smoke [1] (see Table 1). Indoor environmental particles are derived from combustion activities such as cooking, as well as heating with coal, wood or dung, candles, incense, kerosene lamps, and tobacco smoking. In addition, indoor pollution originates from non-combustion sources and volatile organic compounds such as cleaning and insecticide products, electric devices, and printers [3].
It is noteworthy that PM pollution also has important economic ramifications since it increases medical expenses, reduces worker productivity, and damages soil, crops, forests, lakes, and rivers [3].
3. Route of Access and Biological Systems of Particulate Matter
PM can reach and accumulate throughout tissues and organs in humans, such as the gastrointestinal tract, skin, mucosae, placenta, and brain [1].
The cardiovascular system is affected by PM exposure [6][10]. The probability of heart attack due to coronary ischemia, coronary revascularization, ischemic heart disease, thrombosis, or stroke is also positively correlated with air pollution [11][12], especially among the older population [13][14][15], with evidence indicating a possible biological sex bias, where women are affected to a greater extent than men [14][15]. Notably, non-industrial fine airborne particles (e.g., dust particles from dry desert areas) contribute to the probability of developing cardiovascular diseases as much as anthropogenic PM2.5, e.g., emitted from industrial (e.g., metals) and agricultural (organic chemicals) sites [16]. While the impact of air pollution on respiratory health can manifest even after brief exposure to elevated levels of PM2.5, the effects on the cardiovascular system are best observed through longitudinal studies comparing populations exposed to long-term high levels of PM2.5 to those living in areas with PM2.5 levels within the safety limit of 10–12 μg/m3 [17].
The brain is especially vulnerable to air pollution. Inhalation is the main route of PM exposure [6][18][19]. Costa and collaborators characterized PM absorption into the brain [6]. PM enters the central nervous system (CNS) through the nose but follows different paths depending on the size and solubility. While PM10 is deposited in the upper airways, PM2.5 is deposited in the lungs and is also subject to olfactory transport and deposition in the olfactory cortex and other brain regions [6][19][20]. Furthermore, UFPM can be deposited in the cerebral cortex and cerebellum secondary to transport via the olfactory nerves [18]. Once reaching the lung, PM may also travel through the blood into the brain [6][20] (See Table 1). Understanding these pathways and how PM is capable of reaching the CNS underscores the urgent need for an in-depth analysis of its impact on cognitive function. In the brain, PM accumulation contributes to CNS diseases [2][21][22]. The impact on older people is such that there is even evidence of a greater accumulation of amyloid beta (a characteristic of Alzheimer’s disease, AD) in individuals exposed to higher levels of air pollution [21].
Overall, the decrease in PM2.5 concentration correlates with the reduction of hospitalization and early death rates [23], decreasing the burden on economic sectors and the health care system. Altogether, PM exposure affects the respiratory, cardiovascular, and autoimmune systems, potentially accelerating its adverse effects on cognitive functions (Figure 1).
Table 1. Summaries of etiology of particulate matter and pathways implicated until reaching the CNS in the brain.
| PM by Diameter | 1 Main Etiology | Deposited in: | References |
|---|---|---|---|
| PM0.1 or UFPM ≤100 nm |
Smoke from wildfire | Cerebral cortex and cerebellum secondary to transport via the olfactory nerves | [1][18] |
| PM2.5 ≤2.5 μm |
Traffic-related activities, industrial sites, factories, and agriculture | 2 Lungs and is also subject to olfactory transport and deposition in the olfactory cortex and other brain regions | [6][8][9][20] |
| PM10 ≤10 μm |
Pollen, mold, and dust particles | Filtered out by the nose and upper airways |
[6][8][9][19][20] |
UFPM: ultrafine particles; CNS: central nervous system. Notes: 1 Outdoor environmental particles are primarily produced from road transport, agriculture, power plants, industry, and forest fires [1][6]. Indoor environmental particles are derived from combustion activities such as cooking, as well as and heating with coal, wood or dung, candles, incense, kerosene lamps, tobacco smoking, non-combustion sources, and volatile organic compounds such as cleaning and insecticide products, electric devices, and printers [3]. 2 PM enters through the nose; once the lungs are reached, PM may also travel through the blood into the brain [6][20].
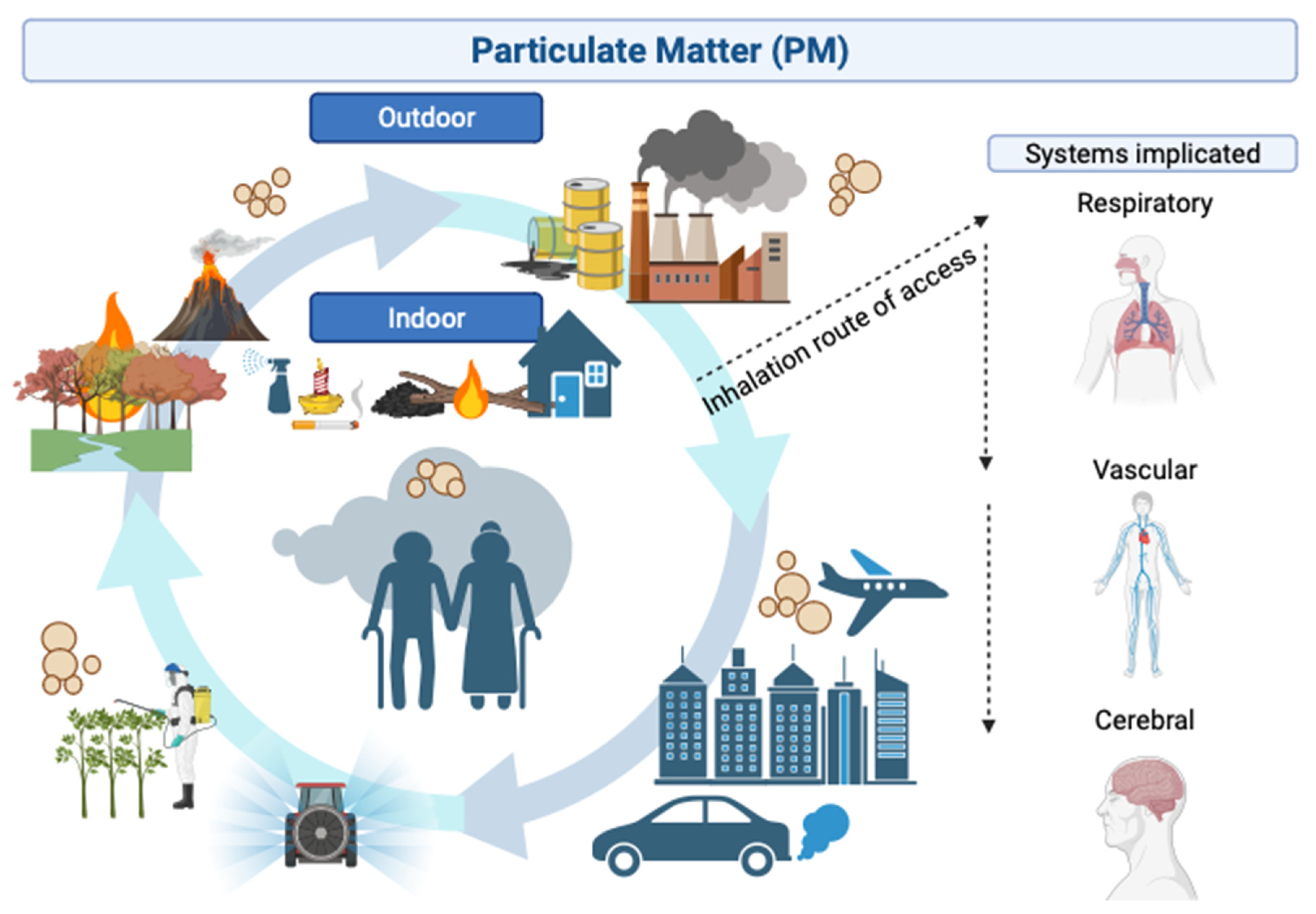
Figure 1. Overview of indoor and outdoor air pollution sources and their consequences to the human body. The main origin of outdoor PM is from a combination of industrial activity, internal combustion engines, traffic-related and geographic and meteorological conditions linked to increased forest fires and practices derived from agricultural activities. On the other hand, indoor environment particles originate from combustion, encompassing activities such as cooking and heating with coal, wood or dung, candles, incense, kerosene lamps, tobacco smoking, and non-combustion sources, such as cleaning and insecticide products, electric devices, and printers. PM enters the body via inhalation through the nose, increasing the risk of respiratory, cardiovascular, and cerebrovascular disease, therefore affecting the CNS. Figure created with BioRender.com (accessed on 10 October 2023).
References
- Calderón-Garcidueñas, L.; Ayala, A. Air Pollution, Ultrafine Particles, and Your Brain: Are Combustion Nanoparticle Emissions and Engineered Nanoparticles Causing Preventable Fatal Neurodegenerative Diseases and Common Neuropsychiatric Outcomes? Environ. Sci. Technol. 2022, 56, 6847–6856.
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.; Coburn, J. Effects of Air Pollution on the Nervous System and Its Possible Role in Neurodevelopmental and Neurodegenerative Disorders. Pharmacol. Ther. 2020, 210, 107523.
- World Health Organization. WHO Global Air Quality Guidelines; World Health Organization: Geneva, Switzerland, 2021.
- Brugha, R.; Grigg, J. Urban Air Pollution and Respiratory Infections. Paediatr. Respir. Rev. 2014, 15, 194–199.
- Anderson, J.O.; Thundiyil, J.G.; Stolbach, A. Clearing the Air: A Review of the Effects of Particulate Matter Air Pollution on Human Health. J. Med. Toxicol. 2012, 8, 166–175.
- Costa, L.G.; Cole, T.B.; Dao, K.; Chang, Y.C.; Garrick, J.M. Developmental Impact of Air Pollution on Brain Function. Neurochem. Int. 2019, 131, 104580.
- Thangavel, P.; Park, D.; Lee, Y.C. Recent Insights into Particulate Matter (PM2.5)-Mediated Toxicity in Humans: An Overview. Int. J. Environ. Res. Public Health 2022, 19, 7511.
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14.
- Kim, K.-H.; Kabir, E.; Kabir, S. A Review on the Human Health Impact of Airborne Particulate Matter. Environ. Int. 2015, 74, 136–143.
- Robert, D.; Brook, S.R. Air Pollution and Cardiovascular Events. N. Engl. J. Med. 2007, 356, 2104–2106.
- Hayes, R.B.; Lim, C.; Zhang, Y.; Cromar, K.; Shao, Y.; Reynolds, H.R.; Silverman, D.T.; Jones, R.R.; Park, Y.; Jerrett, M.; et al. PM2.5 Air Pollution and Cause-Specific Cardiovascular Disease Mortality. Int. J. Epidemiol. 2020, 49, 25–35.
- Thurston, G.D.; Ahn, J.; Cromar, K.R.; Shao, Y.; Reynolds, H.R.; Jerrett, M.; Lim, C.C.; Shanley, R.; Park, Y.; Hayes, R.B. Ambient Particulate Matter Air Pollution Exposure and Mortality in the NIH-AARP Diet and Health Cohort. Environ. Health Perspect. 2016, 124, 484–490.
- Kim, S.; Bae, H.; Lim, Y. Estimating the Health Burden of Ambient Fine Particulate Matter in Korea. In Proceedings of the ISEE 2022: 34th Annual Conference of the International Society of Environmental Epidemiology, Megaron, Athens, 18–21 September 2022; Volume 2022.
- Miller, K.A.; Siscovick, D.S.; Sheppard, L.; Shepherd, K.; Sullivan, J.H.; Anderson, G.L.; Kaufman, J.D. Long-Term Exposure to Air Pollution and Incidence of Cardiovascular Events in Women. N. Engl. J. Med. 2007, 356, 447–458.
- Seaton, A.; Godden, D.; MacNee, W.; Donaldson, K. Particulate Air Pollution and Acute Health Effects. Lancet 1995, 345, 176–178.
- Jalali, S.; Karbakhsh, M.; Momeni, M.; Taheri, M.; Amini, S.; Mansourian, M.; Sarrafzadegan, N. Long-Term Exposure to PM2.5 and Cardiovascular Disease Incidence and Mortality in an Eastern Mediterranean Country: Findings Based on a 15-Year Cohort Study. Environ. Health 2021, 20, 112.
- Alexeeff, S.E.; Liao, N.S.; Liu, X.; Van Den Eeden, S.K.; Sidney, S. Long-Term PM2.5 Exposure and Risks of Ischemic Heart Disease and Stroke Events: Review and Meta-Analysis. J. Am. Heart Assoc. 2021, 10, e016890.
- Oberdörster, G.; Sharp, Z.; Atudorei, V.; Elder, A.; Gelein, R.; Kreyling, W.; Cox, C. Translocation of Inhaled Ultrafine Particles to the Brain. Inhal. Toxicol. 2004, 16, 437–445.
- Ajmani, G.S.; Suh, H.H.; Pinto, J.M. Effects of Ambient Air Pollution Exposure on Olfaction: A Review. Environ. Health Perspect. 2016, 124, 1683–1693.
- Forman, H.J.; Finch, C.E. A Critical Review of Assays for Hazardous Components of Air Pollution. Free Radic. Biol. Med. 2018, 117, 202–217.
- Calderón-Garcidueñas, L.; Reed, W.; Maronpot, R.R.; Henríquez-Roldán, C.; Delgado-Chavez, R.; Calderón-Garcidueñas, A.; Dragustinovis, I.; Franco-Lira, M.; Aragón-Flores, M.; Solt, A.C.; et al. Brain Inflammation and Alzheimer’s-like Pathology in Individuals Exposed to Severe Air Pollution. Toxicol. Pathol. 2004, 32, 650–658.
- Block, M.L.; Calderón-Garcidueñas, L. Air Pollution: Mechanisms of Neuroinflammation and CNS Disease. Trends Neurosci. 2009, 32, 506–516.
- Fann, N.; Risley, D. The Public Health Context for PM2.5 and Ozone Air Quality Trends. Air Qual. Atmos. Health 2013, 6, 1–11.
More
Information
Subjects:
Toxicology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
482
Revisions:
3 times
(View History)
Update Date:
22 Jan 2024
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No