Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Enrique Soto-Pérez-De-Celis | -- | 1227 | 2023-08-02 03:05:16 | | | |
| 2 | Catherine Yang | Meta information modification | 1227 | 2023-08-02 03:08:48 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Castelo-Loureiro, A.; Perez-De-Acha, A.; Torres-Perez, A.C.; Cunha, V.; García-Valdés, P.; Cárdenas-Reyes, P.; Soto-Perez-De-Celis, E. Specific Symptoms in Older Adults with Cancer. Encyclopedia. Available online: https://encyclopedia.pub/entry/47522 (accessed on 28 July 2026).
Castelo-Loureiro A, Perez-De-Acha A, Torres-Perez AC, Cunha V, García-Valdés P, Cárdenas-Reyes P, et al. Specific Symptoms in Older Adults with Cancer. Encyclopedia. Available at: https://encyclopedia.pub/entry/47522. Accessed July 28, 2026.
Castelo-Loureiro, Alicia, Andrea Perez-De-Acha, Ana Cristina Torres-Perez, Vanessa Cunha, Paola García-Valdés, Paula Cárdenas-Reyes, Enrique Soto-Perez-De-Celis. "Specific Symptoms in Older Adults with Cancer" Encyclopedia, https://encyclopedia.pub/entry/47522 (accessed July 28, 2026).
Castelo-Loureiro, A., Perez-De-Acha, A., Torres-Perez, A.C., Cunha, V., García-Valdés, P., Cárdenas-Reyes, P., & Soto-Perez-De-Celis, E. (2023, August 02). Specific Symptoms in Older Adults with Cancer. In Encyclopedia. https://encyclopedia.pub/entry/47522
Castelo-Loureiro, Alicia, et al. "Specific Symptoms in Older Adults with Cancer." Encyclopedia. Web. 02 August, 2023.
Copy Citation
Advanced cancer represents the most common reason for needing palliative care among older adults worldwide. Palliative care is an essential component of cancer care with a direct impact on quality of life. The complex healthcare needs of older patients with cancer therefore require a comprehensive assessment, including a geriatric evaluation.
cancer
older adults
ageism
palliative care
pain
1. Pain
Between 25% and 40% of older patients with cancer experience pain daily [1]. Pain is associated with increased dependence on activities of daily living, risk of falls, malnutrition, limitation in social activity, and increased risk of depression [2][3][4]. Since the etiology of pain in older adults with cancer is multifactorial, they benefit from a multidisciplinary team approach, including a geriatrician, a palliative care physician, a physical medicine and rehabilitation physician, physical therapists, and a psychiatrist or psychologist when appropriate [2][3][4][5]. The evaluation of pain in older adults may be a challenge since some (with and without cognitive impairment) may have difficulty responding to numerical pain scales. Other verbal descriptor scales, pain thermometers, and facial pain scales may have greater validity in older populations [2][4][6].
Treatment plans for older patients with cancer should incorporate non-pharmacological interventions such as massage, relaxation techniques, exercise, and rehabilitation [3][7][8]. Acetaminophen should be considered as a first-line treatment for pain management due to its proven efficacy and good safety profile [7]. Non-steroidal anti-inflammatory drugs should be administered at the lowest dose, for the shortest possible time, while monitoring for possible adverse effects (AEs) [7]. Although older people are more sensitive to the analgesic properties of opioids, they are also at higher risk of toxicity, and require close monitoring for AEs and adequate laxative therapy [7]. A good strategy is to use low-dose drug combinations (in which each analgesic acts by a different mechanism) to improve analgesic efficacy [4][7]. Adjuvants are recommended in neuropathic pain and in patients with associated depression. Serotonin and norepinephrine reuptake inhibitors are a good option since they would have analgesic effects superior to those of traditional selective serotonin reuptake inhibitors [9].
2. Anorexia/Cachexia
Cancer cachexia is a multifactorial syndrome defined by an ongoing loss of skeletal muscle mass that cannot be reversed by conventional nutritional support and leads to progressive functional impairment [10]. It is associated with an increase in chemotherapy toxicity, increased mortality, and QoL impairment [10]. The presence of anorexia/loss of appetite is associated with an increased risk of malnutrition, sarcopenia, care requirements, hospitalization, falls, and impaired cognition [11]. Anorexia is difficult to control, with the first step being the identification and treatment of issues which may interfere with appetite, such as a dry mouth, pain, or nausea [8].
No widely approved drug for the treatment of cancer cachexia is available. Neither glucocorticoids nor megestrol acetate improve cancer anorexia-cachexia syndrome beyond a few weeks, and may cause AEs, particularly among older adults [12][13]. Promising drugs include ghrelin secretagogues, such as anamorelin, which significantly stimulate appetite in patients with cancer; however, in patients aged ≥65 years, the effects of these drugs are less significant, and their use does not lead to improved handgrip strength or decreased mortality and/or disability [14][15].
In older patients with cancer, the best strategy to ameliorate cachexia can be a multimodal approach including exercise, nutritional support and, in some cases, medications. While these recommendations are part of guidelines issued by the European Society of Medical Oncology (ESMO) and the American Society of Clinical Oncology (ASCO), there is limited evidence regarding their use in older individuals [16][17].
The single-arm NEXTAC-ONE trial examined a multimodal intervention (exercise and nutrition for eight weeks), in 30 patients aged ≥70 years with advanced lung or pancreatic cancer, demonstrating feasibility and low rate of adverse effects [18]. The NEXTAC-TWO study is underway, which is a randomized clinical trial aimed at determining the efficacy of this intervention [19]. In the ENeRgy clinical trial, 45 patients aged ≥65 years with advanced cancer were enrolled and randomized to a personalized program based on exercise and nutrition or standard care for eight weeks [20]. The trial demonstrated feasibility, but was not powered to assess effects on nutritional, functional or QoL outcomes. Qualitative findings demonstrated the positive impact of the intervention, so the ENeRgise study is under development and aims to improve statistical power by recruiting a larger number of patients [20].
3. Dyspnea
Dyspnea is a subjective experience of respiratory discomfort consisting of qualitatively distinct sensations that vary in intensity [21]. Patients with reversible causes of dyspnea, such as pleural effusion, infection, exacerbation of pulmonary disease, pulmonary embolism, or treatment-induced pneumonitis, should receive targeted treatments [22][23].
Systemic opioids should be offered when non-pharmacologic interventions fail to relieve dyspnea [22][23][24]. Although there is a lack of information on the use of opioids as a treatment for dyspnea in older adults, data suggest that doses required are usually lower than those for treating pain. Since dyspnea is associated with increased anxiety, relaxation techniques and breathing retraining should be performed [8]. If this is not enough, short-acting benzodiazepines can be offered in combination with opioids [25], bearing in mind that these drugs increase the risk of falls, contributing to mortality and morbidity [26]. Non-pharmacologic alternatives should always be considered, limiting opioid and benzodiazepine use to the lowest dose and shortest possible duration.
4. Delirium
Delirium is a fluctuating disturbance in attention and awareness that represents a decline from baseline status, accompanied by cognitive dysfunction [8]. Delirium incidence ranges from 3% to 45% among inpatients with cancer, increasing to 59% to 88% near the end-of-life [27]. The risk of delirium increases with age [28][29], and its presence is associated with increased morbidity, mortality, length of stay, and need for long-term care [30]. According to psychomotor characteristics and level of arousal, delirium is divided into three subtypes: hyperactive, hypoactive, and mixed type [31]. The most common type of delirium in patients with advanced cancer requiring hospitalization due to poor symptom control is hypoactive delirium, which is the most difficult to diagnose and the hardest to treat, with a mortality of up to 81% during hospitalization (compared with 14% for hyperactive delirium) [32]. The etiology of delirium is multifactorial, ranging from infections to medication-related AEs. In patients with cancer, the possibility of central nervous system metastases or AEs of cancer treatment, including immunotherapy, should always be considered [32][33].
Delirium may interfere with the diagnosis and management of other symptoms, such as pain, which in turn may worsen delirium [8]. It also interferes with the patient’s decision-making capacity, making shared decision-making significantly more complex [34]. The main treatment consists of non-pharmacological interventions focused on prevention [35][36]. However, when non-pharmacological interventions are insufficient, treatment with psychotropic drugs such as antipsychotics medications may be necessary [33].
5. Nausea
The etiology of nausea in patients with cancer is not limited to AEs of treatment, and other causes such as opioid toxicity, bowel obstruction, or constipation must be excluded [8]. Other causes of nausea may be particularly relevant in older adults, since data show they have a lower risk of chemotherapy-induced nausea and vomiting (CINV) than their younger counterparts [37]. In addition, older adults are more likely to receive reduced chemotherapy dosing, which may also lead to reduced risk of CINV.
None of the current antiemetic guidelines include specific recommendations for older patients receiving chemotherapy, since there is little evidence for it’s use in older individuals [38][39][40]. It seems reasonable to deprescribe or adjust the dosing of antiemetics in older adults with cancer, although this needs to be investigated in controlled trials. Single-dose dexamethasone, for example, has the same efficacy as multiple doses in older adults (excluding cisplatin-containing schedules) [41][42]. Figure 1 illustrates recommendations for prescribing antiemetics in older patients with cancer [37].
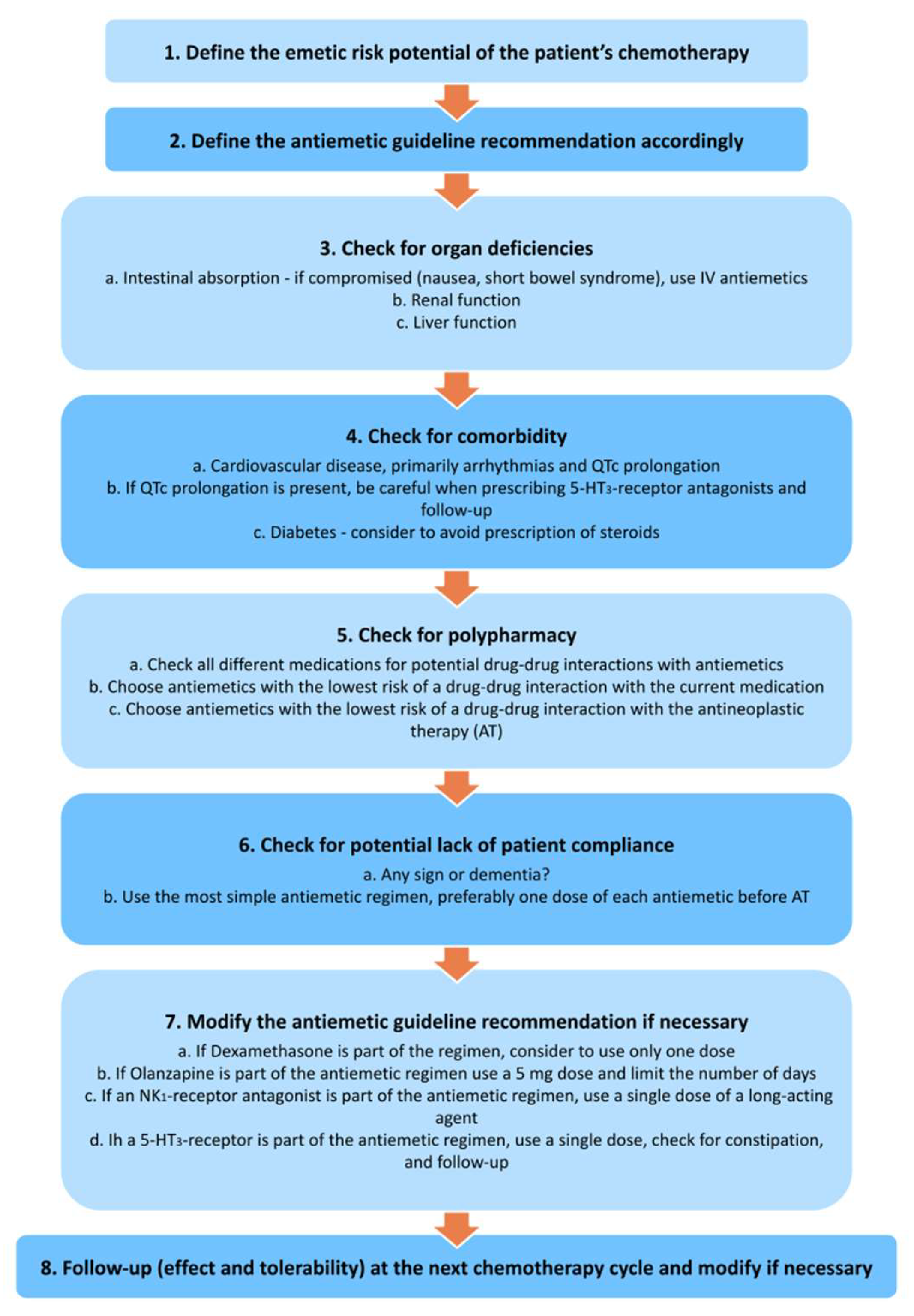
Figure 1. Recommendations for prescribing antiemetics in older patients with cancer [36].
References
- Bernabei, R.; Gambassi, G.; Lapane, K.; Landi, F.; Gatsonis, C.; Dunlop, R.; Lipsitz, L.; Steel, K.; Mor, V. Management of pain in elderly patients with cancer. SAGE Study Group. Systematic Assessment of Geriatric Drug Use via Epidemiology. Jama 1998, 279, 1877–1882.
- Hadjistavropoulos, T.; Herr, K.; Turk, D.C.; Fine, P.G.; Dworkin, R.H.; Helme, R.; Jackson, K.; Parmelee, P.A.; Rudy, T.E.; Lynn Beattie, B.; et al. An interdisciplinary expert consensus statement on assessment of pain in older persons. Clin. J. Pain 2007, 23, S1–S43.
- Makris, U.E.; Abrams, R.C.; Gurland, B.; Reid, M.C. Management of persistent pain in the older patient: A clinical review. Jama 2014, 312, 825–836.
- Rodriguez, C.S. The management of persistent pain in older persons. J. Am. Geriatr. Soc. 2002, 50, S205–S224.
- Rittberg, R.; Sutherland, J.; Huynh, E.; Green, S.; Wiens, A.; Stirling, M.; Dawe, D.E. Assessing the learning needs of the multidisciplinary team on geriatric oncology and frailty. J. Geriatr. Oncol. 2019, 10, 829–831.
- Herr, K.; Bjoro, K.; Decker, S. Tools for assessment of pain in nonverbal older adults with dementia: A state-of-the-science review. J. Pain Symptom Manag. 2006, 31, 170–192.
- Abdulla, A.; Adams, N.; Bone, M.; Elliott, A.M.; Gaffin, J.; Jones, D.; Knaggs, R.; Martin, D.; Sampson, L.; Schofield, P. Guidance on the management of pain in older people. Age Ageing 2013, 42 (Suppl. S1), i1-57.
- Alexander, K.; Goldberg, J.; Korc-Grodzicki, B. Palliative Care and Symptom Management in Older Patients with Cancer. Clin. Geriatr. Med. 2016, 32, 45–62.
- Trivedi, M.H. The link between depression and physical symptoms. Prim. Care Companion J. Clin. Psychiatry 2004, 6, 12–16.
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet. Oncol. 2011, 12, 489–495.
- Fielding, R.A.; Landi, F.; Smoyer, K.E.; Tarasenko, L.; Groarke, J. Association of anorexia/appetite loss with malnutrition and mortality in older populations: A systematic literature review. J. Cachexia Sarcopenia Muscle 2023, 14, 706–729.
- Lim, Y.L.; Teoh, S.E.; Yaow, C.Y.L.; Lin, D.J.; Masuda, Y.; Han, M.X.; Yeo, W.S.; Ng, Q.X. A Systematic Review and Meta-Analysis of the Clinical Use of Megestrol Acetate for Cancer-Related Anorexia/Cachexia. J. Clin. Med. 2022, 11, 3756.
- Currow, D.C.; Glare, P.; Louw, S.; Martin, P.; Clark, K.; Fazekas, B.; Agar, M.R. A randomised, double blind, placebo-controlled trial of megestrol acetate or dexamethasone in treating symptomatic anorexia in people with advanced cancer. Sci. Rep. 2021, 11, 2421.
- Currow, D.; Temel, J.S.; Abernethy, A.; Milanowski, J.; Friend, J.; Fearon, K.C. ROMANA 3: A phase 3 safety extension study of anamorelin in advanced non-small-cell lung cancer (NSCLC) patients with cachexia. Ann. Oncol. 2017, 28, 1949–1956.
- Temel, J.S.; Abernethy, A.P.; Currow, D.C.; Friend, J.; Duus, E.M.; Yan, Y.; Fearon, K.C. Anamorelin in patients with non-small-cell lung cancer and cachexia (ROMANA 1 and ROMANA 2): Results from two randomised, double-blind, phase 3 trials. Lancet Oncol. 2016, 17, 519–531.
- Arends, J.; Strasser, F.; Gonella, S.; Solheim, T.S.; Madeddu, C.; Ravasco, P.; Buonaccorso, L.; de van der Schueren, M.A.E.; Baldwin, C.; Chasen, M.; et al. Cancer cachexia in adult patients: ESMO Clinical Practice Guidelines(☆). ESMO Open 2021, 6, 100092.
- Roeland, E.J.; Bohlke, K.; Baracos, V.E.; Bruera, E.; Del Fabbro, E.; Dixon, S.; Fallon, M.; Herrstedt, J.; Lau, H.; Platek, M.; et al. Management of Cancer Cachexia: ASCO Guideline. J. Clin. Oncol. 2020, 38, 2438–2453.
- Naito, T.; Mitsunaga, S.; Miura, S.; Tatematsu, N.; Inano, T.; Mouri, T.; Tsuji, T.; Higashiguchi, T.; Inui, A.; Okayama, T.; et al. Feasibility of early multimodal interventions for elderly patients with advanced pancreatic and non-small-cell lung cancer. J. Cachexia Sarcopenia Muscle 2019, 10, 73–83.
- Miura, S.; Naito, T.; Mitsunaga, S.; Omae, K.; Mori, K.; Inano, T.; Yamaguchi, T.; Tatematsu, N.; Okayama, T.; Morikawa, A.; et al. A randomized phase II study of nutritional and exercise treatment for elderly patients with advanced non-small cell lung or pancreatic cancer: The NEXTAC-TWO study protocol. BMC Cancer 2019, 19, 528.
- Hall, C.C.; Skipworth, R.J.E.; Blackwood, H.; Brown, D.; Cook, J.; Diernberger, K.; Dixon, E.; Gibson, V.; Graham, C.; Hall, P.; et al. A randomized, feasibility trial of an exercise and nutrition-based rehabilitation programme (ENeRgy) in people with cancer. J. Cachexia Sarcopenia Muscle 2021, 12, 2034–2044.
- Parshall, M.B.; Schwartzstein, R.M.; Adams, L.; Banzett, R.B.; Manning, H.L.; Bourbeau, J.; Calverley, P.M.; Gift, A.G.; Harver, A.; Lareau, S.C.; et al. An official American Thoracic Society statement: Update on the mechanisms, assessment, and management of dyspnea. Am. J. Respir. Crit. Care Med. 2012, 185, 435–452.
- Hui, D.; Bohlke, K.; Bao, T.; Campbell, T.C.; Coyne, P.J.; Currow, D.C.; Gupta, A.; Leiser, A.L.; Mori, M.; Nava, S.; et al. Management of Dyspnea in Advanced Cancer: ASCO Guideline. J. Clin. Oncol. 2021, 39, 1389–1411.
- Hui, D.; Maddocks, M.; Johnson, M.J.; Ekström, M.; Simon, S.T.; Ogliari, A.C.; Booth, S.; Ripamonti, C. Management of breathlessness in patients with cancer: ESMO Clinical Practice Guidelines. ESMO Open 2020, 5, e001038.
- Yamaguchi, T.; Matsunuma, R.; Matsuda, Y.; Tasaki, J.; Ikari, T.; Miwa, S.; Aiki, S.; Takagi, Y.; Kiuchi, D.; Suzuki, K.; et al. Systemic Opioids for Dyspnea in Cancer Patients: A Real-world Observational Study. J. Pain Symptom Manag. 2023, 65, 400–408.
- Yasuda, S.; Sugano, K.; Matsuda, Y.; Kako, J.; Takagi, Y.; Watanabe, H.; Kasahara, Y.; Goya, S.; Kohara, H.; Mori, M.; et al. Systematic review and meta-analysis of the efficacy of benzodiazepines for dyspnea in patients with cancer. Jpn. J. Clin. Oncol. 2023, 53, 327–334.
- Capiau, A.; Huys, L.; van Poelgeest, E.; van der Velde, N.; Petrovic, M.; Somers, A. Therapeutic dilemmas with benzodiazepines and Z-drugs: Insomnia and anxiety disorders versus increased fall risk: A clinical review. Eur. Geriatr. Med. 2022, 1–12.
- Hosie, A.; Davidson, P.M.; Agar, M.; Sanderson, C.R.; Phillips, J. Delirium prevalence, incidence, and implications for screening in specialist palliative care inpatient settings: A systematic review. Palliat. Med. 2013, 27, 486–498.
- Seiler, A.; Schubert, M.; Hertler, C.; Schettle, M.; Blum, D.; Guckenberger, M.; Weller, M.; Ernst, J.; von Känel, R.; Boettger, S. Predisposing and precipitating risk factors for delirium in palliative care patients. Palliat. Support. Care 2020, 18, 437–446.
- Bush, S.H.; Tierney, S.; Lawlor, P.G. Clinical Assessment and Management of Delirium in the Palliative Care Setting. Drugs 2017, 77, 1623–1643.
- Seiler, A.; Blum, D.; Deuel, J.W.; Hertler, C.; Schettle, M.; Zipser, C.M.; Ernst, J.; Schubert, M.; von Känel, R.; Boettger, S. Delirium is associated with an increased morbidity and in-hospital mortality in cancer patients: Results from a prospective cohort study. Palliat. Support. Care 2021, 19, 294–303.
- Meagher, D. Motor subtypes of delirium: Past, present and future. Int. Rev. Psychiatry 2009, 21, 59–73.
- Chishi, K.V.; Patel, B.C.; Umrania, R.A.; Sanghavi, P.R.; Yadav, V.S.; Raval, L.V. Prevalence of Delirium in Advance Cancer Patients Admitted in Hospice Centre and Outcome after Palliative Intervention. Indian J. Palliat. Care 2023, 29, 82–88.
- Breitbart, W.; Alici, Y. Evidence-based treatment of delirium in patients with cancer. J. Clin. Oncol. 2012, 30, 1206–1214.
- García Ortiz de Uriarte, L.; Galán Molina, V.; Gómez Pardo, P.; Inzitari, M. . Rev. Esp. Geriatr. Gerontol. 2022, 57, 244–245.
- Hshieh, T.T.; Yue, J.; Oh, E.; Puelle, M.; Dowal, S.; Travison, T.; Inouye, S.K. Effectiveness of multicomponent nonpharmacological delirium interventions: A meta-analysis. JAMA Intern. Med. 2015, 175, 512–520.
- Louro, L.A.V.; Possari, J.F.; Lima, A.F.C. Pharmacological and non-pharmacological treatment of delirium in an oncological hospital service: An integrative review. Rev. Bras. Enferm. 2021, 74, e20200200.
- Herrstedt, J.; Lindberg, S.; Petersen, P.C. Prevention of Chemotherapy-Induced Nausea and Vomiting in the Older Patient: Optimizing Outcomes. Drugs Aging 2022, 39, 1–21.
- Hesketh, P.J.; Kris, M.G.; Basch, E.; Bohlke, K.; Barbour, S.Y.; Clark-Snow, R.A.; Danso, M.A.; Dennis, K.; Dupuis, L.L.; Dusetzina, S.B.; et al. Antiemetics: ASCO Guideline Update. J. Clin. Oncol. 2020, 38, 2782–2797.
- Roila, F.; Molassiotis, A.; Herrstedt, J.; Aapro, M.; Gralla, R.J.; Bruera, E.; Clark-Snow, R.A.; Dupuis, L.L.; Einhorn, L.H.; Feyer, P.; et al. 2016 MASCC and ESMO guideline update for the prevention of chemotherapy- and radiotherapy-induced nausea and vomiting and of nausea and vomiting in advanced cancer patients. Ann. Oncol. 2016, 27, v119–v133.
- Berger, M.J.; Ettinger, D.S.; Aston, J.; Barbour, S.; Bergsbaken, J.; Bierman, P.J.; Brandt, D.; Dolan, D.E.; Ellis, G.; Kim, E.J.; et al. NCCN Guidelines Insights: Antiemesis, Version 2.2017. J. Natl. Compr. Cancer Netw. JNCCN 2017, 15, 883–893.
- Ito, Y.; Tsuda, T.; Minatogawa, H.; Kano, S.; Sakamaki, K.; Ando, M.; Tsugawa, K.; Kojima, Y.; Furuya, N.; Matsuzaki, K.; et al. Placebo-Controlled, Double-Blinded Phase III Study Comparing Dexamethasone on Day 1 With Dexamethasone on Days 1 to 3 With Combined Neurokinin-1 Receptor Antagonist and Palonosetron in High-Emetogenic Chemotherapy. J. Clin. Oncol. 2018, 36, 1000–1006.
- Celio, L.; Bonizzoni, E.; Bajetta, E.; Sebastiani, S.; Perrone, T.; Aapro, M.S. Palonosetron plus single-dose dexamethasone for the prevention of nausea and vomiting in women receiving anthracycline/cyclophosphamide-containing chemotherapy: Meta-analysis of individual patient data examining the effect of age on outcome in two phase III trials. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2013, 21, 565–573.
More
Information
Subjects:
Oncology
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
747
Revisions:
2 times
(View History)
Update Date:
02 Aug 2023
Table of Contents



Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No