Your browser does not fully support modern features. Please upgrade for a smoother experience.
Submitted Successfully!
 +1 credit
+1 credit
Thank you for your contribution! You can also upload a video entry or images related to this topic.
For video creation, please contact our Academic Video Service.
| Version | Summary | Created by | Modification | Content Size | Created at | Operation |
|---|---|---|---|---|---|---|
| 1 | Mohamed KSANTINI | -- | 1287 | 2023-05-24 12:07:22 | | | |
| 2 | Jessie Wu | + 1 word(s) | 1288 | 2023-05-25 03:29:36 | | |
Video Upload Options
We provide professional Academic Video Service to translate complex research into visually appealing presentations. Would you like to try it?
Cite
If you have any further questions, please contact Encyclopedia Editorial Office.
Obaid, A.M.; Turki, A.; Bellaaj, H.; Ksantini, M.; Altaee, A.; Alaerjan, A. Gallbladder Diseases. Encyclopedia. Available online: https://encyclopedia.pub/entry/44770 (accessed on 25 July 2026).
Obaid AM, Turki A, Bellaaj H, Ksantini M, Altaee A, Alaerjan A. Gallbladder Diseases. Encyclopedia. Available at: https://encyclopedia.pub/entry/44770. Accessed July 25, 2026.
Obaid, Ahmed Mahdi, Amina Turki, Hatem Bellaaj, Mohamed Ksantini, Abdulla Altaee, Alaa Alaerjan. "Gallbladder Diseases" Encyclopedia, https://encyclopedia.pub/entry/44770 (accessed July 25, 2026).
Obaid, A.M., Turki, A., Bellaaj, H., Ksantini, M., Altaee, A., & Alaerjan, A. (2023, May 24). Gallbladder Diseases. In Encyclopedia. https://encyclopedia.pub/entry/44770
Obaid, Ahmed Mahdi, et al. "Gallbladder Diseases." Encyclopedia. Web. 24 May, 2023.
Copy Citation
The gallbladder (GB) is a tiny pouch and a hollow organ located beneath the liver. Its primary role is to temporarily store bile. Bile is a fluid formed by the liver, which is used to aid digestion.
artificial intelligence
deep learning
deep neural network
ultrasound images
diagnosis
gallbladder
1. Introduction
There are different types of gallbladder (GB) disease. From gallstones to cancer, they all have similar symptoms, but they vary widely in severity [1]. All scientists confirm that although the exact causes of GB cancer are unknown, certain factors may increase a person’s risk of developing GB cancer. Frequently, these factors are related to the simple inflammation of the GB. According to the American Cancer Society (ACS) [2] and the American Society of Clinical Oncology (ASCO) [3], the risk of GB cancer is around five times higher in people who have a history of GB conditions, mainly gallstones, compared to those who do not. To this end, it is crucial to diagnose the type of GB disease and how serious it is at an early stage in order to prevent or reduce the wider spread of the disease.
Early detection and diagnosis are the primary sources of lifesaving and are among the most-challenging features of health surveillance. Indeed, according to the Canadian Cancer Society (CCS), about 19% of people diagnosed with GB cancer survive for at least 5 years. Unfortunately, only about 4% of those with stage 4 survive their cancer for 5 or more years, compared to 50% of those diagnosed with stage 1.
To perfectly diagnose GB diseases, ultrasound imaging, as one of the most frequently used imaging modalities, is recognized as a powerful and universal screening and diagnostic tool for physicians and radiologists [4]. After screening, an accurate diagnosis is necessary to identify an appropriate disease treatment plan. Typically, diagnostic information is collected from the patient’s history and clinical examination. Many indications and symptoms can be ambiguous, especially those related to GB diseases, which have similar symptoms. Therefore, ultrasound images (UI) have to be interpreted and understood by highly qualified medical professionals. Given that diagnosis via ultrasound imaging can be time- and labor-consuming, it can be difficult to fund and take advantage of this service in remote locations [5]. Regretfully, many analysts refuse to work in rural areas, and some hospitals do not have the resources to train existing medical professionals to provide this service. As a result, an informative method is needed to simplify the UI acquisition and evaluation process in order to recognize the organ-related pathologies and anomalies in a widely accessible and achievable manner. In rural locations, this informative method can be very useful in computerized healthcare structures, which is the prime motivation of the proposed study. Indeed, if any anomalies are discovered during the initial screening step, specialists and radiologists can detect intraabdominal organ issues and provide the exact treatment. Unskilled radiologists can also use the produced healthcare model to build relative research on scans for evaluating different solutions [6].
Currently, artificial intelligence (AI) techniques, ranging from machine learning (ML) to deep learning (DL), are prevalent in healthcare for disease diagnosis, drug discovery, drug development, and patient risk identification [7]. The advances in DL and deep neural network (DNN)-based methods of research and development provide significant progress in the domain of medical image analysis and understanding [8]. Moreover, with the progress at the algorithmic level as well as the availability of high-performance computing machines and large quantities of data, DL-based methods have become increasingly popular [9]. They are now considered to be the most commonly used and most sophisticated algorithms for handling many computer vision tasks [10]. In addition, DL algorithms are capable of assisting analysts in the early identification, treatment, and recognition of diseases, and they, subsequently, provide efficient methods for medical diagnostics. Indeed, DL algorithms can directly process and automatically learn mid-level and high-level abstract features acquired from immense quantities of raw collected data, in which higher-level abstract features are defined by combining them with lower-level features, to achieve an acceptable level of accuracy and, eventually, to perform automatic UI analysis tasks, such as classification, organ segmentation, and object detection [9][11][12][13][14].
2. Overview of Gallbladder Diseases
The GB is located on the lower surface of the right side of the liver and has separate anatomic sections, including the neck, fundus, cystic duct, and infundibulum. The GB is divided into four layers: (1) the mucosa, (2) the muscularis, (3) the perimuscular layer, and (4) the serosa. The GB is also complicated, despite its small size [15]. In total, 10–15% of the adult population is affected by GB disorders, so it is comparably prevalent, with the most common pathology being cholelithiasis [16].
2.1. Gallstones
The components that make up bile are numerous, with the most important being cholesterol, bilirubin (a by-product of red blood cell degradation), and bile salts, all of which are dissolved in water. These components are often produced by the liver and stored in the GB.
Gallstones form as a result of an imbalance in those components, for example, increased cholesterol (due to high liver output) forms cholesterol gallstones in the GB (the most common form) (Figure 1). The exact cause of these derangements is multifactorial and is not the purpose of this research. Gallstones can remain asymptomatic until the duct that transports bile into the small intestine becomes blocked by a gallstone, which induces a variety of symptoms depending on the anatomical location and severity of the blockage. This often necessitates treatment, which can be in the form of elective surgical removal of the stone and GB [17].
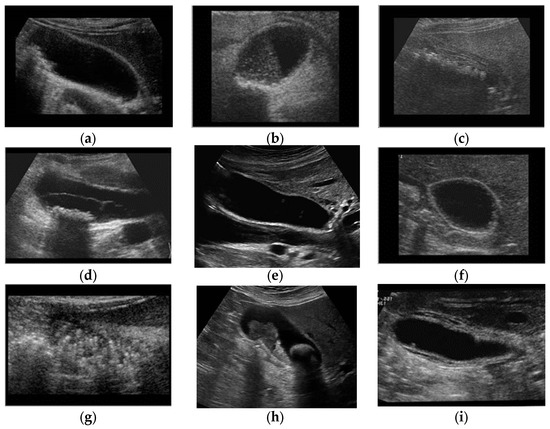
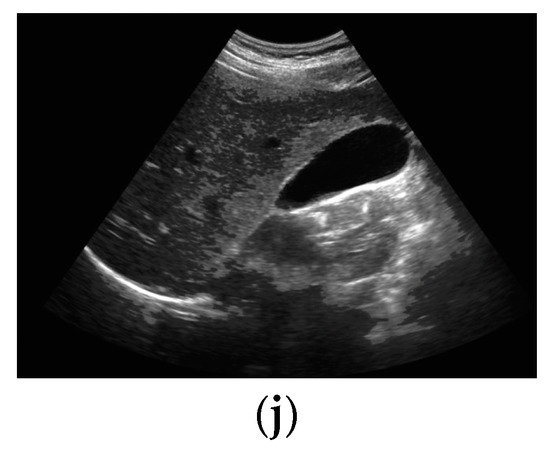
Figure 1. GB diseases (a–i): (a) gallstones, (b) abdomen and retroperitoneum, (c) cholecystitis, (d) gangrenous cholecystitis, (e) perforation, (f) polyps and cholesterol crystals, (g) adenomyomat osis, (h) carcinoma, (i) GB wall thickening, and (j) normal GB.
2.2. Biliary Colic and Calculous Cholecystitis
Temporary pain due to the obstruction of the cystic duct by a gallstone upon bile secretion is known as biliary colic. This pain usually quickly subsides, but, if the obstruction persists, it can lead to cholecystitis (as shown in Figure 1c) [18][19]. Prolonged blockage of the cystic duct can cause inflammation in the GB, leading to GB wall thickening (Figure 1i). This inflammation can result in fever, lethargy, and constant pain.
2.3. Gangrenous Cholecystitis
Cholecystitis that remains untreated eventually causes the GB to turn gangrenous (Figure 1d) [20]. This occurs as a result of edema, which induces vascular insufficiency to the GB, leading to ischemia of the GB tissue. It is a life-threatening condition due to the high risk of perforation (Figure 1e) [21], which may lead to hemodynamic instability [22][23].
2.4. Polyps and Cholesterol Polyps
Polyps are uncommon, with a 9–26% frequency range based on surgery and autopsy sequencing data. The most common are cholesterol polyps. They occur as a result of a buildup of lipid within the macrophages in the lamina propria projecting into the inner lumen of the GB; this process is known as cholesterolosis. These are benign growths (Figure 1f), as they are made from cholesterol deposition rather than neoplastic growths [24].
2.5. Adenomyomatosis of the GB
Adenomyomatosis of the GB is an illness characterized by aberrant mucosal epithelial hypertrophy, resulting in the pathognomonic epithelial invaginations known as Luschka’s crypts in the GB [25]. These crypts often house cholesterol crystals that aid in forming a distinct appearance upon imaging (Figure 1h). They have a frequency rate of between 1% and 9% in cholecystectomy specimens, with a steady sex proportion. They become more common after the age of 50, supporting the hypothesis that chronic inflammation is a cause.
2.6. Carcinoma
GB cancer [26] is a very rare tumor occurring in 1:100,000 of cases, mainly in those aged over 70. It is more common in females than males (2:1). Chronic inflammation is the most important risk factor for developing carcinoma, which is why it occurs in those with a history of gallstones (Figure 1g) [27][28] Carcinomas can metastasize to other parts of the body or remain confined to a specific area [29].
References
- Gallbladder Disease. Available online: https://englewoodgi.com/conditions-and-diseases/gallbladder-disease/ (accessed on 13 April 2023).
- American Cancer Society. Gallbladder Cancer Risk Factors. 29 March 2021. Available online: https://www.cancer.org/cancer/gallbladder-cancer/causes-risks-prevention/risk-factors.html (accessed on 4 October 2021).
- American Society of Clinical Oncology. Gallbladder Cancer: Risk Factors and Prevention. Available online: https://www.cancer.net/cancer-types/gallbladder-cancer/risk-factors-and-prevention (accessed on 4 October 2021).
- Okaniwa, S. Everything you need to know about ultrasound for diagnosis of gallbladder diseases. J. Med. Ultrason. 2021, 48, 145–147.
- Ogiela, M.; Bodzioch, S. Computer analysis of gallbladder ultrasonic images towards recognition of pathological lesions. Opto-Electron. Rev. 2011, 19, 155–168.
- Selvathi, D.; Chandralekha, R. Fetal biometric based abnormality detection during prenatal development using deep learning techniques. Multidimens. Syst. Signal Process. 2022, 33, 1–15.
- Li, B.-H.; Hou, B.-C.; Yu, W.-T.; Lu, X.-B.; Yang, C.-W. Applications of artificial intelligence in intelligent manufacturing: A review. Front. Inf. Technol. Electron. Eng. 2017, 18, 86–96.
- Liu, X.; Gao, K.; Liu, B.; Pan, C.; Liang, K.; Yan, L.; Ma, J.; He, F.; Zhang, S.; Pan, S.; et al. Advances in Deep Learning-Based Medical Image Analysis. Health Data Sci. 2021, 2021, 8786793.
- Wang, J.; Zhu, H.; Wang, S.-H. A review of deep learning on medical image analysis. Mob. Netw. Appl. 2021, 26, 351–380.
- Litjens, G.; Kooi, T.; Bejnordi, B.E.; Setio, A.A.A.; Ciompi, F.; Ghafoorian, M.; van der Laak, J.A.W.M.; van Ginneken, B.; Sánchez, C.I. A survey on deep learning in medical image analysis. Med. Image Anal. 2017, 42, 60–88.
- Shen, D.; Wu, G.; Suk, H.-I. Deep learning in medical image analysis. Annu. Rev. Biomed. Eng. 2017, 19, 221–248.
- Zhou, S.K.; Greenspan, H.; Davatzikos, C.; Duncan, J.S.; Van Ginneken, B.; Madabhushi, A.; Prince, J.L.; Rueckert, D.; Summers, R.M. A review of deep learning in medical imaging: Imaging traits, technology trends, case studies with progress highlights, and future promises. Proc. IEEE 2021, 109, 820–838.
- Esteva, A.; Kuprel, B.; Novoa, R.A.; Ko, J.; Swetter, S.M.; Blau, H.M.; Thrun, S. Dermatologist-level classification of skin cancer with deep neural networks. Nature 2017, 542, 115–118.
- Shinde, S.; Kulkarni, U.; Mane, D.; Sapkal, A. Deep learning. In Health Informatics: A Computational Perspective in Healthcare; Studies in Computational Intelligence; Springer: Singapore, 2021; pp. 19–42.
- Maurer, K.J.; Carey, M.C.; Fox, J.G. Roles of Infection, Inflammation, and the Immune System in Cholesterol Gallstone Formation. Gastroenterology 2009, 136, 425–440.
- Stinton, L.M.; Shaffer, E.A. Epidemiology of Gallbladder Disease: Cholelithiasis and Cancer. Gut Liver 2012, 6, 172–187.
- Lammert, F.; Gurusamy, K.; Ko, C.W.; Miquel, J.-F.; Méndez-Sánchez, N.; Portincasa, P.; van Erpecum, K.J.; van Laarhoven, C.J.; Wang, D.Q.H. Gallstones. Nat. Rev. Dis. Prim. 2016, 2, 16024.
- Doherty, G.; Manktelow, M.; Skelly, B.; Gillespie, P.; Bjourson, A.J.; Watterson, S. The Need for Standardizing Diagnosis, Treatment and Clinical Care of Cholecystitis and Biliary Colic in Gallbladder Disease. Medicina 2022, 58, 388.
- Gallaher, J.R.; Charles, A. Acute cholecystitis: A review. JAMA 2022, 327, 965–975.
- Jones, M.W.; Genova, R.; O’Rourke, M.C. Acute cholecystitis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK459171/ (accessed on 24 October 2022).
- Derici, H.; Kara, C.; Bozdag, A.D.; Nazli, O.; Tansug, T.; Akca, E. Diagnosis and treatment of gallbladder perforation. World J. Gastroenterol. 2006, 12, 7832–7836.
- Mishal, S.; Penny, S.M. Emphysematous cholecystitis: A deadly twist to a common disease. J. Diagn. Med. Sonogr. 2016, 32, 131–137.
- Zafar, S.N.; Cornwell, E.E. Cholecystitis. Geriatr. Trauma Acute Care Surg. 2018, 9, 307–311.
- Dilek, O.N.; Karasu, S.; Dilek, F.H. Diagnosis and Treatment of Gallbladder Polyps: Current Perspectives. Euroasian J. Hepato-Gastroenterol. 2019, 9, 40–48.
- Golse, N.; Lewin, M.; Rode, A.; Sebagh, M.; Mabrut, J.-Y. Gallbladder adenomyomatosis: Diagnosis and management. J. Visc. Surg. 2017, 154, 345–353.
- Dutta, U. Gallbladder cancer: Can newer insights improve the outcome? J. Gastroenterol. Hepatol. 2012, 27, 642–653.
- Kee, K.-M.; Lu, S.-N. Diagnostic efficacy of ultrasound in hepatocellular carcinoma diagnosis. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 277–279.
- Tanaka, H. Current role of ultrasound in the diagnosis of hepatocellular carcinoma. J. Med. Ultrason. 2020, 47, 239–255.
- Wennmacker, S.Z.; Lamberts, M.P.; Drenth, J.P.; Gurusamy, K.S.; van Laarhoven, C.J. Transabdominal ultrasound or endoscopic ultrasound for diagnosis of gallbladder polyps. Cochrane Database Syst. Rev. 2016, 8, CD012233.
More
Information
Contributors
MDPI registered users' name will be linked to their SciProfiles pages. To register with us, please refer to https://encyclopedia.pub/register
:
View Times:
838
Revisions:
2 times
(View History)
Update Date:
25 May 2023
Table of Contents


Notice
You are not a member of the advisory board for this topic. If you want to update advisory board member profile, please contact office@encyclopedia.pub.
OK
Confirm
Only members of the Encyclopedia advisory board for this topic are allowed to note entries. Would you like to become an advisory board member of the Encyclopedia?
Yes
No
${ textCharacter }/${ maxCharacter }
Submit
Cancel
Back
Comments
${ item }
|
${ item.createdUser.fullName }
${ item.createdAt }
${ item.vote }
${ item.reply }
Delete
${ reply.createdUser.fullName }
${ reply.createdAt }
${ reply.vote }
Delete
There is no reply to this comment~
${ item.replyTextCharacter }/${ item.replyMaxCharacter }
Submit
Cancel
More
No more~
There is no comment~
${ textCharacter }/${ maxCharacter }
Submit
Cancel
${ selectedItem.replyTextCharacter }/${ selectedItem.replyMaxCharacter }
Submit
Cancel
Confirm
Are you sure to Delete?
Yes
No