Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Pavani Rangachari and Version 6 by Bruce Ren.
This paper leverages the Macro-Meso-Micro (three-layer) conceptual framework to characterize the factors influencing telehealth use within a medical specialty. Based on this framework, three levels of factors, including, macro (societal or policy-level), meso (group or organizational-level), and micro (individual-level) factors can help to explain behavior, e.g., telehealth use within a medical specialty.
- telehealth use
- telehealth sustainability
- telemedicine policy
- medical specialties
- hospital organizations
- specialty societies
- patient-centered care
- provider culture
1. Existing Literature on Telehealth Use
The exisDevelopment of the Macro-Meso-Micro Framework on Factors Influencing Telehealth Use within a Medical Specialty
The macro level incorporates policy-level factors, legal-ethical factors, and other societal-level structural factors (e.g., growing healthcare costs and anticipated workforce shortages) influencing telehealth use within a medical specialty. For example, in the US, reimbursement and coverage for telehealth services are not regulated at a national level, which in turn has served as a barrier to telehealth use across nearly all medical specialties. Although Medicare coverage for telehealth has increased during the pandemic, the US continues to lack a standardized set of telehealth reimbursement policies.
At the meso level, emphasis is placed on the role of historical rationale for telehealth use, hospital/health system organizational factors, professional-society factors, technology factors, treatment factors, research factors and cultural factors within a medical specialty. For example, the historical rationale for using telemedicine in allergy-immunology, was to ‘improve access to care’ for underserved populations. In other words, in this specialty, telehealth was not perceived as having the potential to (1) ‘improve patient experience’ (e.g., through patient empowerment for asthma control), (2) ‘reduce healthcare costs; (e.g., by decreasing hospitalizations for asthma), or (3) ‘promote population health’ (e.g., by making self-management of asthma more effective).
Ating telehealthhe literature hasmicro consistently emphasized the importance of recognizing the complexity in implementing telehealth services for successful and sustainable use [1][2]. By definition, telehealth services are delivered over a distance and often span evel emultiple organizational entities with varying cultures, practices, and business models. There are also multiple interdependent dimensions of telehealth to consider, including processes, user-experience, and sustainability. Correspondingly, the design and implementation of telehealth services often involves engagement of stakeholders from a variety of disciplines from both inner and outer settings of the organization, including healthcare hasis is placed on the role of individual providers, managers, administrators, patients, information and communication technologists, economists, and policy makers [1][2]. In -leview of this complexity, a considerable portion of the telehealth literature has paid attention to determinants of failure or success of telehealth initiatives, includingl and patient-level factors (barriers or facilitators) iinfluencing telehealth use and implementation [3][4][5][6][7][2][8][9][10][11][12][13][14][15][16][17][18][19][20][21][22][23].
In 2005, Yellowlees defWined seven core principles for success with telehealth implementation: (1) telehealth applications should be selected pragmatically rather than philosophically, (2) clinician drivers and telehealth users must own the systems, (3) telehealthcare management and support should be from the bottom up rather than top down, (4) the technology should be user-friendly, (5) telehealthcare users must be well-trained and supported, (6) telehealthcare applications should be evaluated in a clinically appropriate and user-friendly manner, and (7) information about the development of telehealth must be shared [3]. This simple yet influential set of printh respect to provider-level faciples touches upon key organizational (meso) and individual-level (micro) factorrs influencing telehealth use, including organizational leadership, change management, technological, and individual pprovider level factors.
Withins the last decade, van Dyk (2014) conducted a comprehensive review to identify and compare existing frameworks on telehealth use and implementation, to identify common themes and areas for future development [2]. A total of nn specine frameworks related to telehealth use and implementation were reviewed, including: (1) barriers to the diffusion of telemedicine, which emphasize technical, behavioral, economic, and organizational barriers; (2) lties with higher telehealth readiness assessment tools, which emphasize core (planning), technological, learning, societal, and policy readiness; (3) telehealth applications of the Unified Theory of Acceptance and Use of Technology (UTAUT), which describe the interaction among several variables influencing technology acceptance, including the perceived importance of standardization; (4) the seven core principles for the successful implementation of telemedicine (discussed earlier); (5) lessons in telemedicine service innovation, which identify factors contributing to telehealth success, including the policy context, evidence gathering, outcomes monitoring, perceived benefit, reconfiguring services, professional roles, and willingness to cross boundaries; (6) a framework for assessing health system challenges to scaling up for telehealth, which includes consideration for policy, organizational, technological, and financial challenges; (7) a comprehensive model for evaluation of telemedicine, which considers several issues related to telehealth implementation, including cost of education, quality of clinical services, and community access to services, among others; (8) a layered telemedicine implementation model, which identifies determinants of success associated with each lifecycle phase use are reported to have made proactive efforts to partner with and engage patients in use of telemedicine; and (9) the Khoja–Durrani–Scott (KDS) Evaluation Framework, which also considers telehealth lifecycle stages and incorporates various themes of evaluation, including readiness and change, policy, technological, behavioral, economic, and ethical. Overall, the review by van Dyk (2014) concluded that a holistic approach is needed to telehealth implementation, which includes consideration for organizational structures, change management, technology, economic feasibility, societal impacts, perceptions, user-friendliness, evidence and evaluation, and policy and legislation [3][2][8][9][10][11][12][13][14][15][16][17].
In moehealth services. For example, in psychiatry, divere recent years, the Consolidated Framework for Implementation Research (CFIR) has been leveraged to guide telehealth service implementation initiatives [18][19][20][21]. Since its introde patient grouction in 2009, the CFIR has gained considerable popularity and recognition as an influential theoretical framework to inform both ‘implementation science’ and ‘implementation strategy’ [18]. The CFIR comprises five major s have reportedomains: (1) Intervention characteristics, (2) Outer setting (3) Inner setting (4) Characteristics of individuals and (5) Process. Each domain, in turn, is mapped to an array of constructs informed by existing implementation theories and conceptual models. For example, the domain of inner setting is mapped to the following constructs: structural characteristics, networks and communication, culture (including norms and values of the organization), and implementation climate or the absorptive capacity for change. The five domains (and constructs) in the CFIR in turn interact in rich and complex ways to influence implementation effectiveness. The CFIR is a pragmatic meta-theoretical framework with a comprehensive taxonomy, which could be used to guide formative evaluation of implementation, including the identification of potential barriers and facilitators from the perspective of the individuals and organizations involved in the implementation [18].
2. Developing a Macro-Meso-Micro Conceptual Framework on Factors Influencing Telehealth Use within a Medical Specialty
Taken togetherthat they are comfortable using telepsychiatry. In cardiology, the substantial existing literature on telehealth use and implementation frameworks, helps to identify a comprehensive set of macro-meso-micro level factors (barriers or facilitators) influeemote monitorincing telehealth use to guide the narrative review of the literature across six medical specialties. To begin with, at the macro level, the frameworks ohas been telehealth readiness assessment, lessons in telemedicine service innovation, framework for assessing health system challenges, the KDS framework, and the CFIR all point to the importance of consideration for policy-level factors, legal-ethical factors, and other societal-level structural factors (e.g., growing healthcare costs and anticipated workforce shortages) influencing telehealth use. Likewise, at the meso level, emphasis ound to improve confidence on the perceived importance in the UTAUT and the perceived benefit in lessons from telemedicine innovation points to the importance of considering the role of the historical perceived importance or rationale for telehealth use as a factor influencing telehealth use within the specialty. Similarly, the emphasis on organizational leadership and change management in the seven core principles, the KDS framework, and the CFIR highlight the importance of considering the influence of both hospital/health system organizational factors and specialty professional-society organizational factors on telehealth use within the medical specialty. It would be relevant to note that financial factors influencing telehealth use would be subsumed within health system organizational factors, since economic feasibility and impact consideration of telehealth investments are expected to arise at a provider organizational level, rather than at a specialty level. Next, the domain of intervention characteristics in the CF older patients in managing heart failure symptoms.IR and the emphasis on technology across all frameworks calls for the consideration of the influence of technological factors [3][8][18]. Si summilarly, the emphasis on reconfiguring services from lessons in telemedicine innovation, and quality of clinical services in the comprehensive model for telemedicine evaluation, call for the consideration of the influence of treatment factors on telehealth use within the specialty. Likewise, the emphasis on evidence gathering and outcomes monitoring in lessons on telemedicine service innovation, and on intervention characteristics in the CFIR, calls for the consideration of the influence of research factors, and the emphasis on organizational culture in the CFIR calls for the consideration of the influence of cultural factors on telehealth use in the medical specialtyy, a review of the existing literature helped [18].
At the micro level, the emphasis on the individual (clinicians and users) in the seven core principles, Unified Theory of Acceptance and Use, and the CFIR, points to the importance of considering individual provider-level factors and patient-level dentify a total of 12 factors influencing telehealth use [3][8][10][11][13][15][17][18]. In summary, the review of existing literature on factors influencing telehealth use and implementation helped to identify a total of 12 factors acrthin a medical specialty across allmacro-meso-micro 3 levels, including 3 at the macro level, 7 at the meso level and 2 at the micro level. The final conceptual framework used to guide the review iis summarized in Figure 1.
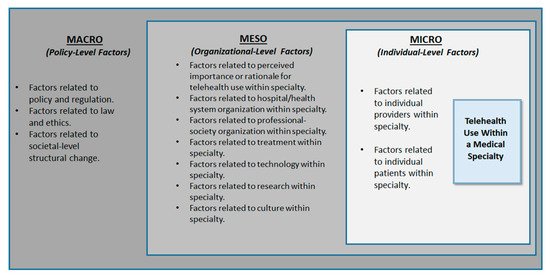
Figure 1. Conceptual Framework on Factors Influencing Telehealth Use Within a Medical Specialty.