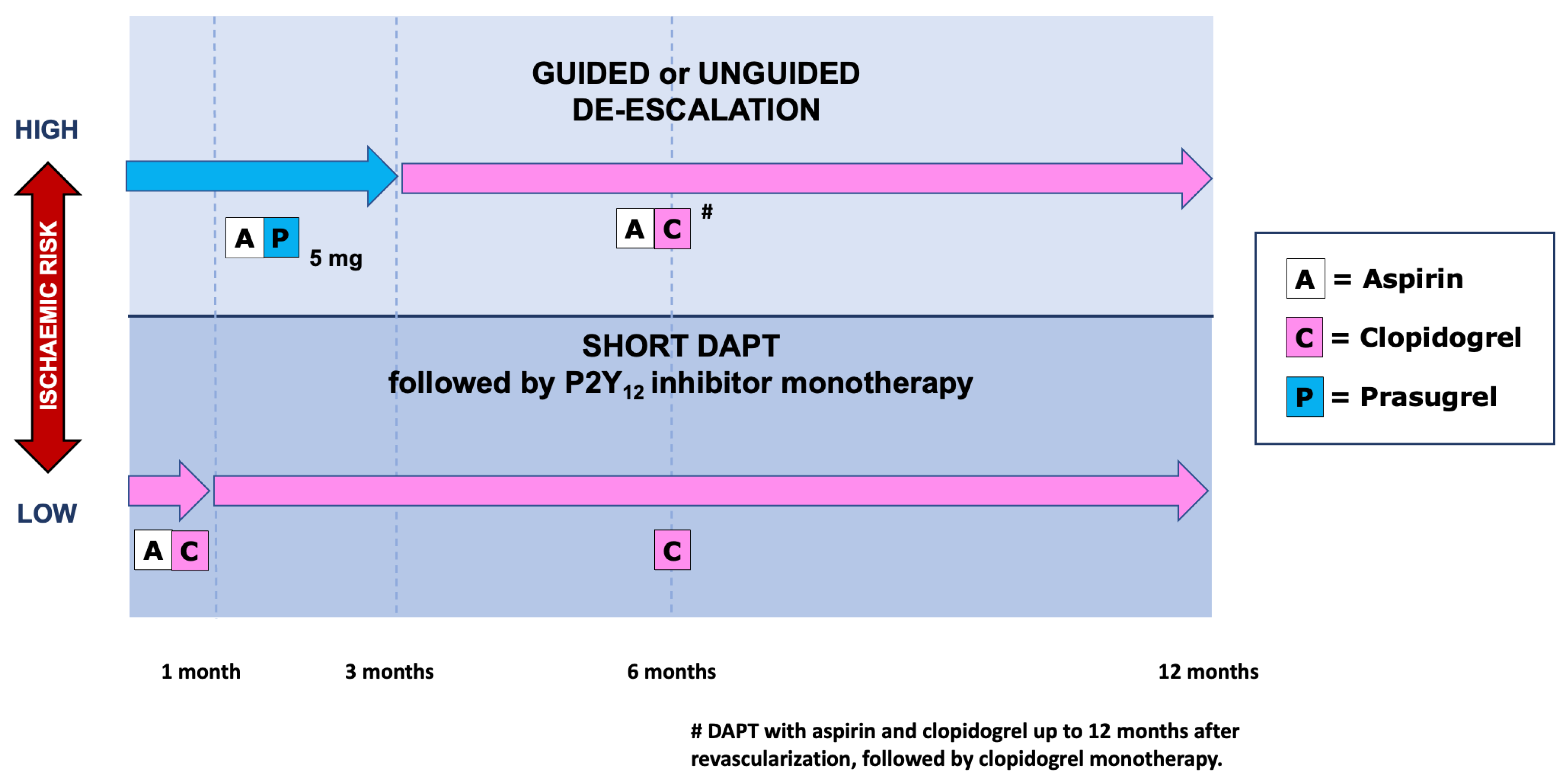
Patients ≥ 75 years of age account for about one third of hospitalizations for acute coronary syndromes (ACS). Since the European Society of Cardiology guidelines recommend that older ACS patients use the same diagnostic and interventional strategies used by the younger ones, most elderly patients are currently treated invasively. Therefore, an appropriate dual antiplatelet therapy (DAPT) is indicated as part of the secondary prevention strategy to be implemented in such patients. The choice of the composition and duration of DAPT should be tailored on an individual basis, after careful assessment of the thrombotic and bleeding risk of each patient. Advanced age is a main risk factor for bleeding. Data show that in patients of high bleeding risk short DAPT (1 to 3 months) is associated with decreased bleeding complications and similar thrombotic events, as compared to standard 12-month DAPT. Clopidogrel seems the preferable P2Y12 inhibitor, due to a better safety profile than ticagrelor. When the bleeding risk is associated with a high thrombotic risk (a circumstance present in about two thirds of older ACS patients) it is important to tailor the treatment by taking into account the fact that the thrombotic risk is high during the first months after the index event and then wanes gradually over time, whereas the bleeding risk remains constant.
- elderly patients
- acute coronary syndrome
- anti-platelet therapy
1. Introduction
2. Invasive versus Conservative Strategy
3. Dual Antiplatelet Therapy in Elderly ACS Patients: Comparative Efficacy and Safety among Different P2Y12 Inhibitors
4. Bleeding and Thrombotic Risk in Elderly ACS Patients
5. Antiplatelet Strategies in Elderly ACS Patients
6. Conclusions
This entry is adapted from the peer-reviewed paper 10.3390/jcm12052082
References
- Di Lorenzo, E.; Sauro, R.; Varricchio, A.; Capasso, M.; Lanzillo, T.; Manganelli, F.; Carbone, G.; Lanni, F.; Pagliuca, M.R.; Stanco, G.; et al. Randomized comparison of everolimus-eluting stents and sirolimus-eluting stents in patients with ST elevation myocardial infarction: RACES-MI trial. JACC Cardiovasc. Interv. 2014, 7, 849–856.
- De Luca, G.; Schaffer, A.; Wirianta, J.; Suryapranata, H. Comprehensive meta-analysis of radial vs femoral approach in primary angioplasty for STEMI. Int. J. Cardiol. 2013, 168, 2070–2081.
- De Luca, G.; Suryapranata, H.; Stone, G.W.; Antoniucci, D.; Tcheng, J.E.; Neumann, F.-J.; Bonizzoni, E.; Topol, E.J.; Chiariello, M. Relationship between patient’s risk profile and benefits in mortality from adjunctive abciximab to mechanical revascularization for ST-segment elevation myocardial infarction: A meta-regression analysis of randomized trials. J. Am. Coll. Cardiol. 2006, 47, 685–686.
- Verdoia, M.; Schaffer, A.; Barbieri, L.; Cassetti, E.; Piccolo, R.; Galasso, G.; Marino, P.; Sinigaglia, F.; De Luca, G. Benefits from new ADP antagonists as compared with clopidogrel in patients with stable angina or acute coronary syndrome undergoing invasive management: A meta-analysis of randomized trials. J. Cardiovasc. Pharmacol. 2014, 63, 339–350.
- Costa, F.; Montalto, C.; Branca, M.; Hong, S.J.; Watanabe, H.; Franzone, A.; Vranckx, P.; Hahn, J.Y.; Gwon, H.C.; Feres, F.; et al. Dual antiplatelet therapy duration after percutaneous coronary intervention in high bleeding risk: A meta-analysis of randomized trials. Eur. Heart J. 2022, 250, ehac706.
- Nichols, M.; Townsend, N.; Scarborough, P.; Rayner, M. Cardiovascular disease in Europe: Epidemiological update. Eur. Heart J. 2013, 34, 3028–3034.
- Silverio, A.; Cancro, F.P.; Di Maio, M.; Bellino, M.; Esposito, L.; Centore, M.; Carrizzo, A.; Di Pietro, P.; Borrelli, A.; De Luca, G.; et al. Lipoprotein(a) levels and risk of adverse events after myocardial infarction in patients with and without diabetes. J. Thromb. Thrombolysis 2022, 54, 382–392.
- Verdoia, M.; Schaffer, A.; Barbieri, L.; Bellomo, G.; Marino, P.; Sinigaglia, F.; Suryapranata, H.; De Luca, G. Impact of age on mean platelet volume and its relationship with coronary artery disease: A single-centre cohort study. Exp. Gerontol. 2015, 62, 32–36.
- De Luca, G.; Verdoia, M.; Cassetti, E.; Schaffer, A.; Cavallino, C.; Bolzani, V.; Marino, P. High fibrinogen level is an independent predictor of presence and extent of coronary artery disease among Italian population. J. Thromb. Thrombolysis 2011, 31, 458–463.
- Verdoia, M.; Barbieri, L.; Di Giovine, G.; Marino, P.; Suryapranata, H.; De Luca, G. Neutrophil to Lymphocyte Ratio and the Extent of Coronary Artery Disease: Results from a Large Cohort Study. Angiology 2016, 67, 75–82.
- De Luca, L.; Marini, M.; Gonzini, L.; Boccanelli, A.; Casella, G.; Chiarella, F.; De Servi, S.; Di Chiara, A.; Di Pasquale, G.; Olivari, Z.; et al. Contemporary trends and age-specific sex differences in management and outcome for patients with ST-segment elevation myocardial infarction. J. Am. Heart Assoc. 2016, 5, e004202.
- Leonardi, S.; Montalto, C.; Carrara, G.; Casella, G.; Grosseto, D.; Galazzi, M.; Repetto, A.; Tua, L.; Portolan, M.; Ottani, F.; et al. Clinical governance of patients with acute coronary syndromes. Eur. Heart J. Acute Cardiovasc. Care 2022, 11, 797–805.
- Savonitto, S.; Cavallini, C.; Petronio, A.S.; Murena, E.; Antonicelli, R.; Sacco, A.; Steffenino, G.; Bonechi, F.; Mossuti, E.; Manari, A.; et al. Early aggressive versus initially conservative treatment in elderly patients with non-ST-segment elevation acute coronary syndrome: A randomized controlled trial. JACC Cardiovasc. Interv. 2012, 5, 906–916.
- Morici, N.; Savonitto, S.; Murena, E.; Antonicelli, R.; Piovaccari, G.; Tucci, D.; Tamburino, C.; Fontanelli, A.; Bolognese, L.; Menozzi, M.; et al. Causes of death in patients ≥75 years of age with non-ST-segment elevation acute coronary syndrome. Am. J. Cardiol. 2013, 112, 1–7.
- Morici, N.; De Servi, S.; De Luca, L.; Crimi, G.; Montalto, C.; De Rosa, R.; De Luca, G.; Rubboli, A.; Valgimigli, M.; Savonitto, S. Management of acute coronary syndromes in older adults. Eur. Heart J. 2022, 43, 1542–1553.
- Ekerstad, N.; Swahn, E.; Janzon, M.; Alfredsson, J.; Löfmark, R.; Lindenberger, M.; Carlsson, P. Frailty is independently associated with short-term outcomes for elderly patients with non-ST-segment elevation myocardial infarction. Circulation 2011, 124, 2397–2404.
- Dodson, J.A.; Hochman, J.S.; Roe, M.T.; Chen, A.Y.; Chaudhry, S.I.; Katz, S.; Zhong, H.; Radford, M.J.; Udell, J.A.; Bagai, A.; et al. The association of frailty with in-hospital bleeding among older adults with acute myocardial infarction: Insights from the ACTION Registry. JACC Cardiovasc. Interv. 2018, 11, 2287–2296.
- Damluji, A.A.; Forman, D.E.; Wang, T.Y.; Chikwe, J.; Kunadian, V.; Rich, M.W.; Young, B.A.; Page, R.L., 2nd; DeVon, H.A.; Alexander, K.P.; et al. Management of Acute Coronary Syndrome in the Older Adult Population: A Scientific Statement From the American Heart Association. Circulation 2022, 147, e32–e62.
- De Luca, G.; Dirksen, M.T.; Spaulding, C.; Kelbæk, H.; Schalij, M.; Thuesen, L.; van der Hoeven, B.; Vink, M.A.; Kaiser, C.; Musto, C.; et al. Impact of diabetes on long-term outcome after primary angioplasty: Insights from the DESERT cooperation. Diabetes Care 2013, 36, 1020–1025.
- De Luca, G.; Verdoia, M.; Savonitto, S.; Piatti, L.; Grosseto, D.; Morici, N.; Bossi, I.; Sganzerla, P.; Tortorella, G.; Cacucci, M.; et al. Impact of diabetes on clinical outcome among elderly patients with acute coronary syndrome treated with percutaneous coronary intervention: Insights from the ELDERLY ACS 2 trial. J. Cardiovasc. Med. 2020, 21, 453–459.
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with STsegment elevation. Eur. Heart J. 2018, 39, 119–177.
- Bueno, H.; Betriu, A.; Heras, M.; Alonso, J.J.; Cequier, A.; Garcia, E.J.; Lopez-Sendon, J.L.; Macaya, C.; Hernandez-Antolin, R.; Bueno, H.; et al. Primary angioplasty vs. fibrinolysis in very old patients with acute myocardial infarction: TRIANA (TRatamiento del Infarto Agudo de miocardio eN Ancianos) randomized trial and pooled analysis with previous studies. Eur. Heart J. 2011, 32, 51–60.
- de Boer, M.J.; Ottervanger, J.P.; van’t Hof, A.W.J.; Hoornethe, A.; Suryapranata, H.; Zijlstra, F.; on behalf of the Zwolle Myocardial Infarction Study Group. Reperfusion therapy in elderly patients with acute myocardial infarction. A randomized comparison of primary angioplasty and thrombolytic therapy. J. Am. Coll. Cardiol. 2002, 39, 1723–1728.
- Grines, C. SENIOR PAMI: A prospective randomized trial of primary angioplasty and thrombolytic therapy in elderly patients with acute myocardial infarction. Presented at the Transcatheter Cardiovascular Therapeutics, Washington, DC, USA; 2005. Available online: https://www.acc.org (accessed on 2 February 2023).
- Galasso, G.; De Servi, S.; Savonitto, S.; Strisciuglio, T.; Piccolo, R.; Morici, N.; Murena, E.; Cavallini, C.; Petronio, A.S.; Piscione, F. Effect of an invasive strategy on outcome in patients ≥75 years of age with non-ST-elevation acute coronary syndrome. Am. J. Cardiol. 2015, 115, 576–580.
- Tegn, N.; Abdelnoor, M.; Aaberge, L.; Endresen, K.; Smith, P.; Aakhus, S.; Gjertsen, E.; Dahl-Hofseth, O.; Ranhoff, A.H.; Gullestad, L.; et al. Invasive versus conservative strategy in patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris (After Eighty study): An open-label randomised controlled trial. Lancet 2016, 387, 1057–1065.
- de Belder, A.; Myat, A.; Blaxill, J.; Haworth, P.; O’Kane, P.; Hatrick, R.; Aggarwal, R.K.; Davie, A.; Smith, W.; Gerber, R.; et al. Revascularisation or medical therapy in elderly patients with acute anginal syndromes: The RINCAL randomised trial. EuroIntervention 2021, 17, 67–74.
- Garg, A.; Garg, L.; Agarwal, M.; Rout, A.; Raheja, H.; Agrawal, S.; Rao, S.V.; Cohen, M. Routine invasive versus selective invasive strategy in elderly patients older than 75 years with Non-ST elevation acute coronary syndrome: A systematic review and meta-analysis. Mayo Clin. Proc. 2018, 93, 436–444.
- Kaura, A.; Sterne, J.A.C.; Trickey, A.; Abbott, S.; Mulla, A.; Glampson, B.; Panoulas, V.; Davies, J.; Woods, K.; Mayet, J.; et al. Invasive versus non-invasive management of older patients with non-ST elevation myocardial infarction (SENIOR-NSTEMI): A cohort study based on routine clinical data. Lancet 2020, 396, 623–634.
- The British Heart Foundation SENIOR-RITA Trial (SENIOR-RITA). Available online: https://clinicaltrials.gov/ct2/show/NCT03052036 (accessed on 7 December 2022).
- Verdoia, M.; Pergolini, P.; Rolla, R.; Nardin, M.; Schaffer, A.; Barbieri, L.; Marino, P.; Bellomo, G.; Suryapranata, H.; De Luca, G. Advanced age and high-residual platelet reactivity in patients receiving dual antiplatelet therapy with clopidogrel or ticagrelor. J. Thromb. Haemost. 2016, 14, 57–64.
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2007, 357, 2001–2015.
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus clopidogrel in patients with acute coronary syndromes. N. Engl. J. Med. 2009, 361, 1045–1057.
- De Servi, S.; Goedicke, J.; Schirmer, A.; Widimsky, P. Clinical outcomes for prasugrel versus clopidogrel in patients with unstable angina or non-ST-elevation myocardial infarction: An analysis from the TRITON-TIMI 38 trial. Eur. Heart J. Acute Cardiovasc. Care 2014, 4, 363–372.
- Husted, S.; James, S.; Becker, R.C.; Horrow, J.; Katus, H.; Storey, R.F.; Cannon, C.P.; Heras, M.; Lopes, R.D.; Morais, J.; et al. Ticagrelor versus clopidogrel in elderly patients with acute coronary syndromes: A substudy from the prospective randomized PLATelet inhibition and patient Outcomes (PLATO) trial. Circ. Cardiovasc. Qual. Outcomes 2012, 5, 680–688.
- Savonitto, S.; Ferri, L.A.; Piatti, L.; Grosseto, D.; Piovaccari, G.; Morici, N.; Bossi, I.; Sganzerla, P.; Tortorella, G.; Cacucci, M.; et al. Comparison of reduced-dose prasugrel and standard-dose clopidogrel in elderly patients with acute coronary syndromes undergoing early percutaneous revascularization. Circulation 2018, 137, 2435–2445.
- Crimi, G.; Morici, N.; Ferrario, M.; Ferri, L.A.; Piatti, L.; Grosseto, D.; Cacucci, M.; Mandurino Mirizzi, A.; Toso, A.; Piscione, F.; et al. Time course of ischemic and bleeding burden in elderly patients with acute coronary syndromes randomized to low-dose prasugrel or clopidogrel. J. Am. Heart Assoc. 2019, 8, e010956.
- Roe, M.T.; Goodman, S.G.; Ohman, E.M.; Stevens, S.R.; Hochman, J.S.; Gottlieb, S.; Martinez, F.; Dalby, A.J.; Boden, W.E.; White, H.D.; et al. Elderly patients with acute coronary syndromes managed without revascularization: Insights into the safety of long-term dual antiplatelet therapy with reduced-dose prasugrel versus standard-dose clopidogrel. Circulation 2013, 128, 823–833.
- Gimbel, M.; Qaderdan, K.; Willemsen, L.; Hermanides, R.; Bergmeijer, T.; de Vrey, E.; Heestermans, T.; Tjon Joe Gin, M.; Waalewijn, R.; Hofma, S.; et al. Clopidogrel versus ticagrelor or prasugrel in patients aged 70 years or older with non-STelevation acute coronary syndrome (POPular AGE): The randomised, open label, non-inferiority trial. Lancet 2020, 395, 1374–1381.
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260.
- De Luca, G.; Damen, S.A.; Camaro, C.; Benit, E.; Verdoia, M.; Rasoul, S.; Liew, H.B.; Polad, J.; Ahmad, W.A.; Zambahari, R.; et al. Final results of the randomised evaluation of short-term dual antiplatelet therapy in patients with acute coronary syndrome treated with a new-generation stent (REDUCE trial). EuroIntervention 2019, 15, e990–e998.
- Kedhi, E.; Verdoia, M.; Suryapranata, H.; Damen, S.; Camaro, C.; Benit, E.; Barbieri, L.; Rasoul, S.; Liew, H.B.; Polad, J.; et al. Impact of age on the comparison between short-term vs 12-month dual antiplatelet therapy in patients with acute coronary syndrome treated with the COMBO dual therapy stent: 2-Year follow-up results of the REDUCE trial. Atherosclerosis 2021, 321, 39–44.
- Costa, F.; van Klaveren, D.; James, S.; Heg, D.; Räber, L.; Feres, F.; Pilgrim, T.; Hong, M.K.; Kim, H.S.; Colombo, A.; et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: A pooled analysis of individual-patient datasets from clinical trials. Lancet 2017, 389, 1025–1034.
- Urban, P.; Mehran, R.; Colleran, R.; Angiolillo, D.J.; Byrne, R.A.; Capodanno, D.; Cuisset, T.; Cutlip, D.; Eerdmans, P.; Eikelboom, J.; et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 2019, 40, 2632–2653.
- Fortuni, F.; Crimi, G.; Morici, N.; De Luca, G.; Alberti, L.P.; Savonitto, S.; De Servi, S. Assessing bleeding risk in acute coronary syndrome using the Bleeding Academic Research Consortium definition. J. Cardiovasc. Med. 2019, 20, 818–824.
- Gragnano, F.; Heg, D.; Franzone, A.; McFadden, E.P.; Leonardi, S.; Piccolo, R.; Vranckx, P.; Branca, M.; Serruys, P.W.; Benit, E.; et al. PRECISE-DAPT score for bleeding risk prediction in patients on dual or single antiplatelet regimens: Insights from the GLOBAL LEADERS/and GLASSY. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 28–38.
- Urban, P.; Gregson, J.; Owen, R.; Mehran, R.; Windecker, S.; Valgimigli, M.; Varenne, O.; Krucoff, M.; Saito, S.; Baber, U.; et al. Assessing the risks of bleeding vs thrombotic events in patients at high bleeding risk after coronary stent implantation: The ARC–High Bleeding Risk Trade-off Model. JAMA Cardiol. 2021, 6, 410–419.
- Morici, N.; Savonitto, S.; Ferri, L.A.; Grosseto, D.; Bossi, I.; Sganzerla, P.; Tortorella, G.; Cacucci, M.; Ferrario, M.; Crimi, G.; et al. Outcomes of Elderly Patients with ST-Elevation or Non-ST-Elevation Acute Coronary Syndrome Undergoing Percutaneous Coronary Intervention. Am. J. Med. 2019, 132, 209–216.
- De Servi, S.; Landi, A.; Savonitto, S.; De Luca, L.; De Luca, G.; Morici, N.; Montalto, C.; Crimi, G.; Cattaneo, M. Tailoring oral antiplatelet therapy in acute coronary syndromes: From guidelines to clinical practice. J. Cardiovasc. Med. 2023, 24, 77–86.
- Valgimigli, M.; Frigoli, E.; Heg, D.; Tijssen, J.; Jüni, P.; Vranckx, P.; Ozaki, Y.; Morice, M.C.; Chevalier, B.; Onuma, Y.; et al. Dual antiplatelet therapy after PCI in patients at high bleeding risk. N. Engl. J. Med. 2021, 385, 1643–1655.
- Hong, S.J.; Kim, J.S.; Hong, S.J.; Lim, D.S.; Lee, S.Y.; Yun, K.H.; Park, J.K.; Kang, W.C.; Kim, Y.H.; Yoon, H.J.; et al. 1-Month dual-antiplatelet therapy followed by aspirin monotherapy after polymer-free drug-coated stent implantation. JACC Cardiovasc. Interv. 2021, 14, 1801–1811.
- Capranzano, P. One-month DAPT after acute coronary syndrome: Too short or not too short? EuroIntervention 2022, 18, 443–445.
- De Luca, L.; De Servi, S.; Musumeci, G.; Bolognese, L. Is ticagrelor safe in octogenarian patients with non-ST elevation acute coronary syndromes? Eur. Heart J. Cardiovasc. Pharmacother. 2018, 4, 12–14.
- Montalto, C.; Morici, N.; Munafò, A.R.; Mangieri, A.; Mandurino-Mirizzi, A.; D’Ascenzo, F.; Oreglia, J.; Latib, A.; Porto, I.; Colombo, A.; et al. Optimal P2Y12 inhibition in older adults with acute coronary syndromes: A network meta-analysis of randomized controlled trials. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 20–27.
- Llaó, I.; Ariza-Solé, A.; Sanchis, J.; Alegre, O.; López-Palop, R.; Formiga, F.; Marín, F.; Vidán, M.T.; Martínez-Sellés, M.; Sionis, A.; et al. Invasive strategy and frailty in very elderly patients with acute coronary syndromes. EuroIntervention 2018, 14, e336–e342.
- Andò, G.; De Santis, G.A.; Greco, A.; Pistelli, L.; Francaviglia, B.; Capodanno, D.; De Caterina, R.; Capranzano, P. P2Y12 Inhibitor or Aspirin Following Dual Antiplatelet Therapy After Percutaneous Coronary Intervention: A Network Meta-Analysis. JACC Cardiovasc. Interv. 2022, 15, 2239–2249.
- Lin, K.J.; De Caterina, R.; Rodriguez, L.A.G. Low-dose aspirin and upper gastrointestinal bleeding in primary versus secondary cardiovascular prevention: A population-based, nested case-control study. Circ. Cardiovasc. Qual. Outcomes 2014, 7, 70–77.
- Sundstrom, J.; Hedberg, J.; Thuresson, M.; Aarskog, P.; Johannesen, K.M.; Oldgren, J. Low-Dose Aspirin Discontinuation and Risk of Cardiovascular Events: A Swedish Nationwide, Population-Based Cohort Study. Circulation 2017, 136, 1183–1192.
- Koo, B.K.; Kang, J.; Park, K.W.; Rhee, T.M.; Yang, H.M.; Won, K.B.; Rha, S.W.; Bae, J.W.; Lee, N.H.; Hur, S.H.; et al. Aspirin versus clopidogrel for chronic maintenance monotherapy after percutaneous coronary intervention (HOST-EXAM): An investigator-initiated, prospective, randomized, open-label, multicenter trial. Lancet 2021, 397, 2487–2496.
- Kang, J.; Park, K.W.; Lee, H.; Hwang, D.; Yang, H.M.; Rha, S.W.; Bae, J.W.; Lee, N.H.; Hur, S.H.; Han, J.K.; et al. Aspirin vs. Clopidogrel for Chronic Maintenance Monotherapy after Percutaneous Coronary Intervention: The HOST-EXAM Extended Study. Circulation 2023, 147, 108–117.
- Nelson, T.A.; Parker, W.A.E.; Ghukasyan Lakic, T.; Westerbergh, J.; James, S.K.; Siegbahn, A.; Becker, R.C.; Himmelmann, A.; Wallentin, L.; Storey, R.F. Differential effect of clopidogrel and ticagrelor on leukocyte count in relation to patient characteristics, biomarkers and genotype: A PLATO substudy. Platelets 2022, 33, 425–431.
- Palmerini, T.; Barozzi, C.; Tomasi, L.; Sangiorgi, D.; Marzocchi, A.; De Servi, S.; Ortolani, P.; Reggiani, L.B.; Alessi, L.; Lauria, G.; et al. A randomised study comparing the antiplatelet and antinflammatory effect of clopidogrel 150 mg/day versus 75 mg/day in patients with ST-segment elevation acute myocardial infarction and poor responsiveness to clopidogrel: Results from the DOUBLE study. Thromb. Res. 2010, 125, 309–314.
- Ferrucci, L.; Fabbri, E. Inflammageing: Chronic inflammation in ageing, cardiovascular disease, and frailty. Nat. Rev. Cardiol. 2018, 15, 505–522.
- Laudani, C.; Greco, A.; Occhipinti, G.; Ingala, S.; Calderone, D.; Scalia, L.; Agnello, F.; Legnazzi, M.; Mauro, M.S.; Rochira, C.; et al. Short duration of DAPT versus de-escalation after percutaneous coronary intervention for acute coronary syndromes. JACC Cardiovasc. Interv. 2022, 15, 268–277.
- Montalto, C.; Crimi, G.; Morici, N.; Savonitto, S.; De Servi, S. Use of clinical risk score in an elderly population: Need for ad hoc validation and calibration. J. Am. Coll. Cardiol. 2019, 74, 161–162.