The global internet (Internet of Things, IoT) and innovative information and communication technologies (IT/ICT) are already ubiquitous in the social and individual lives of people. Among them, a very significant role is played by Extended Reality (XR) and its classic components such as Virtual (VR), Augmented (AR) and Mixed (MR) Reality. There are many indications that these modern technologies (XR, i.e., VR/AR/MR, and 3D printing/scanning, holography, artificial intelligence and machine learning, robotics or online (VR) tele-medicine) will be the basis and determinants of the organization and functioning of contemporary and future generations.
- virtual reality
- virtual exercise and training
- cognitive and motor functions
- brain
- basic and clinical neuroscience
1. Introduction
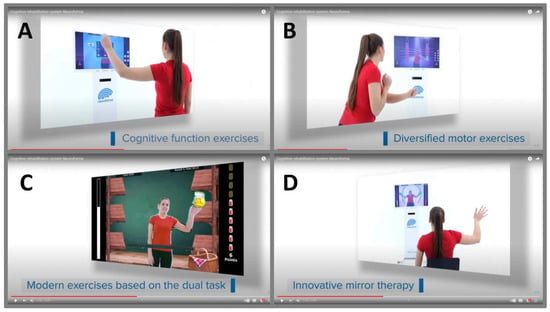
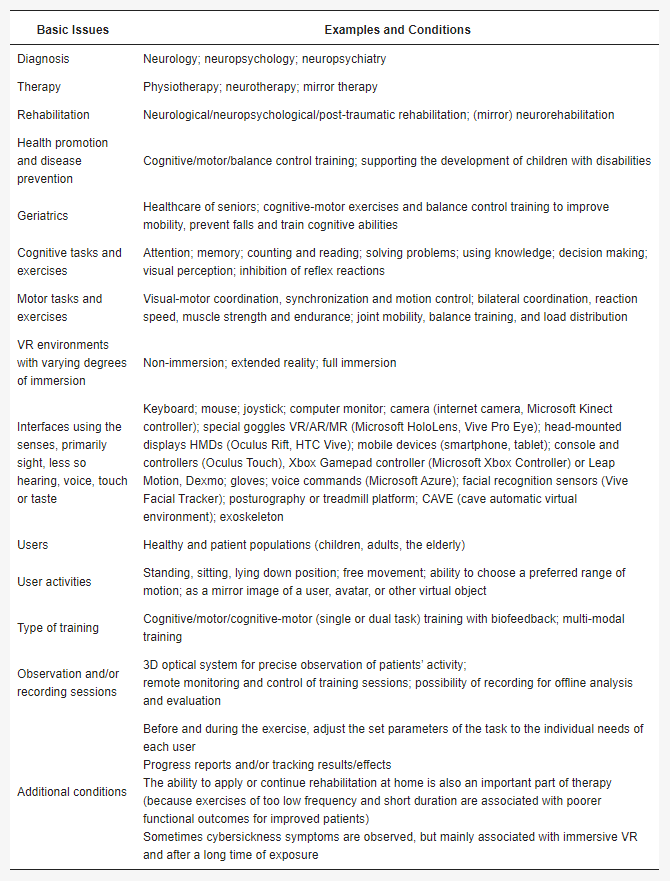
2. Basic Features, Importance and Possibilities of Virtual Exercise and Training

This entry is adapted from the peer-reviewed paper 10.3390/ijerph20054150
References
- Hennen, L.; Hahn, J.; Ladikas, M.; Lindner, R.; Peissl, W.; van Est, R. Technology Assessment in a Globalized World. Facing the Challenges of Transnational Technology Governance; Springer: Cham, Switzerland, 2023.
- Riva, C.G. Special Topics in Information Technology; Springer: Cham, Switzerland, 2023.
- Werthner, H.; Prem, E.; Lee, E.A.; Ghezzi, C. Perspectives on Digital Humanism; Springer Nature: Cham, Switzerland, 2022.
- Li, H.; Zhang, X.; Wang, H.; Yang, Z.; Liu, H.; Cao, Y.; Zhang, G. Access to Nature via Virtual Reality: A Mini-Review. Front. Psychol. 2021, 12, 725288.
- Sharman, W.R.; Craig, W.R. Understanding Virtual Reality. Interface, Application, and Design, 2nd ed.; Elsevier Science Publisher: New York, NY, USA, 2018.
- Tripathy, B.K.; Anuradha, J. Internet of Things (IoT): Technologies, Applications, Challenges, and Solutions; Taylor & Francis Group: Boca Raton, FL, USA, 2018.
- Suzuki, K.; Mariola, A.; Schwartzman, D.J.; Seth, A.K. Using Extended Reality to Study the Experience of Presence. In Current Topics in Behavioral Neurosciences; Springer: Berlin/Heidelberg, Germany, 2023.
- Skarbez, R.; Smith, M.; Whitton, M.C. Revisiting Milgram and Kishino’s Reality-Virtuality Continuum. Front. Virtual. Real. 2021, 2, 647997.
- Grant, C.; Mairn, C. 3D, virtual, augmented, extended, mixed reality, and extended content forms: The technology and the challenges. Inf. Serv. Use. 2020, 40, 225–230.
- Hudson, S.; Matson-Barkat, S.; Pallamin, N.; Jegou, G. With or without you? Interaction and immersion in a virtual reality experience. J. Bus. Res. 2019, 100, 459–468.
- Milgram, P.; Takemura, H.; Utsumi, A.; Kishino, F. Augmented reality: A class of displays on the reality-virtuality continuum. SPIE Telemanipulator Telepresence Technol. 1995, 2351, 282–292.
- Guerrero, D.T.; Asaad, M.; Rajesh, A.; Hassan, A.; Butler, C.E. Advancing Surgical Education: The Use of Artificial Intelligence in Surgical Training. Am. Surg. 2023, 89, 49–54.
- Curry, E.; Auer, S.; Berre, A.J.; Metzger, A.; Perez, M.S.; Zillner, S. Technologies and Applications for Big Data Value; Springer Nature: Cham, Switzerland, 2022.
- Grassini, S. Virtual Reality Assisted Non-Pharmacological Treatments in Chronic Pain Management: A Systematic Review and Quantitative Meta-Analysis. Int. J. Environ. Res. Public. Health 2022, 19, 4071.
- Lai, B.; Davis, D.; Young, R.; Swanson-Kimani, E.; Wozow, C.; Chaviano, K.; Rimmer, J.H. Group Telegaming Through Immersive Virtual Reality to Improve Mental Health Among Adolescents with Physical Disabilities: Pre- and Posttrial Protocol. JMIR Res. Protoc. 2022, 11, e42651.
- Le Noury, P.; Polman, R.; Maloney, M.; Gorman, A. A Narrative Review of the Current State of Extended Reality Technology and How it can be Utilised in Sport. Sport. Med. 2022, 52, 1473–1489.
- Sugimoto, M. Extended Reality (XR:VR/AR/MR), 3D Printing, Holography, A.I., Radiomics, and Online VR Tele-Medicine for Precision Surgery. In Surgery and Operating Room Innovation; Takenoshita, S., Yasuhara, H., Eds.; Springer: Singapore, 2021.
- Palumbo, A. Microsoft HoloLens 2 in Medical and Healthcare Context: State of the Art and Future Prospects. Sensors 2022, 22, 7709.
- van der Putten, K.; Anderson, M.B.; van Geenen, R.C. Looking through the Lens: The Reality of Telesurgical Support with Interactive Technology Using Microsoft’s HoloLens 2. Case Rep. Orthop. 2022, 2022, 5766340.
- Salcedo, D.; Regan, J.; Aebersold, M.; Lee, D.; Darr, A.; Davis, K.; Berrocal, Y. Frequently Used Conceptual Frameworks and Design Principles for Extended Reality in Health Professions Education. Med. Sci. Educ. 2022, 32, 1587–1595.
- Wei, W.; Qin, Z.; Yan, B.; Wang, Q. Application Effect of Motion Capture Technology in Basketball Resistance Training and Shooting Hit Rate in Immersive Virtual Reality Environment. Comput. Intell. Neurosci. 2022, 2022, 4584980.
- Barteit, S.; Lanfermann, L.; Bärnighausen, T.; Neuhann, F.; Beiersmann, C. Augmented, Mixed, and Virtual Reality-Based Head-Mounted Devices for Medical Education: Systematic Review. JMIR Serious Games 2021, 9, e29080.
- Ibrahim, Z.; Money, A.G. Computer mediated reality technologies: A conceptual framework and survey of the state of the art in healthcare intervention systems. J. Biomed. Inform. 2019, 90, 103102.
- Pennefather, P.; Krebs, C. Exploring the Role of xR in Visualisations for Use in Medical Education. Adv. Exp. Med. Biol. 2019, 1171, 15–23.
- Jackson, K.M.; Shaw, T.H.; Helton, W.S. Evaluating the dual-task decrement within a simulated environment: Word recall and visual search. Appl. Ergon. 2023, 106, 103861.
- Bonkhoff, A.K.; Grefkes, C. Precision medicine in stroke: Towards personalized outcome predictions using artificial intelligence. Brain 2022, 145, 457–475.
- Lyu, L.Q.; Cui, H.Y.; Shao, M.Y.; Fu, Y.; Zhao, R.X.; Chen, Q.P. Computational Medicine: Past, Present and Future. Chin. J. Integr. Med. 2021, 28, 453–462.
- Coscia, M.; Wessel, M.J.; Chaudary, U.; Millán, J.D.R.; Micera, S.; Guggisberg, A.; Vuadens, P.; Donoghue, J.; Birbaumer, N.; Hummel, F.C. Neurotechnology-aided interventions for upper limb motor rehabilitation in severe chronic stroke. Brain 2019, 142, 2182–2197.
- Keawtep, P.; Wichayanrat, W.; Boripuntakul, S.; Chattipakorn, S.C.; Sungkarat, S. Cognitive Benefits of Physical Exercise, Physical–Cognitive Training, and Technology-Based Intervention in Obese Individuals with and without Postmenopausal Condition: A Narrative Review. Int. J. Environ. Res. Public Health 2022, 19, 13364.
- Kyaw, B.M.; Saxena, N.; Posadzki, P.; Vseteckova, J.; Nikolaou, C.K.; George, P.P.; Divakar, U.; Masiello, I.; Kononowicz, A.A.; Zary, N.; et al. Virtual Reality for Health Professions Education: Systematic Review and Meta-Analysis by the Digital Health Education Collaboration. J. Med. Internet Res. 2019, 21, e12959.
- Palacios-Navarro, G.; Hogan, N. Head-Mounted Display-Based Therapies for Adults Post-Stroke: A Systematic Review and Meta-Analysis. Sensors 2021, 21, 1111.
- Parr, T.; Limanowski, J.; Rawji, V.; Friston, K. The computational neurology of movement under active inference. Brain 2021, 144, 1799–1818.
- Slutzky, M.W. Brain-Machine Interfaces: Powerful Tools for Clinical Treatment and Neuroscientific Investigations. Neuroscentist 2019, 25, 139–154.
- Diemer, J.; Alpers, G.W.; Peperkorn, H.M.; Shiban, Y.; Mühlberger, A. The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 2015, 6, 26.
- Burns, A.; Adeli, H.; Buford, J.A. Brain-computer interface after nervous system injury. Neuroscientist 2014, 20, 639–651.
- Khan, A.; Podlasek, A.; Somaa, F. Virtual reality in post-stroke neurorehabilitation—A systematic review and meta-analysis. Top. Stroke Rehabil. 2023, 30, 53–72.
- Chatelain, L.S.; Khalifé, M.; Riouallon, G.; Guigui, P.; Ferrero, E. Pedagogy in spine surgery: Developing a free and open-access virtual simulator for lumbar pedicle screws placement. Eur. Spine J. 2022, 32, 712–717.
- Chaudhary, U.; Mrachacz-Kersting, N.; Birbaumer, N. Neuropsychological and neurophysiological aspects of brain-computer-interface (BCI) control in paralysis. J. Physiol. 2021, 599, 2351–2359.
- Yang, S.; Li, R.; Li, H.; Xu, K.; Shi, Y.; Wang, Q.; Yang, T.; Sun, X. Exploring the Use of Brain-Computer Interfaces in Stroke Neurorehabilitation. Biomed. Res. Int. 2021, 2021, 9967348.
- Rizzo, A.; Bouchard, S. Virtual Reality for Psychological and Neurocognitive Interventions; Springer Science + Business Media: New York, NY, USA, 2019.
- Bassett, D.S.; Gazzaniga, M.S. Understanding complexity in the human brain. Trends Cogn. Sci. 2011, 15, 200–209.
- Website of the ISVR. Available online: https://isvr.org/ (accessed on 24 January 2023).
- Bisiacchi, P.; Cainelli, E. Structural and functional brain asymmetries in the early phases of life: A scoping review. Brain Struct. Funct. 2022, 227, 479–496.
- Bonini, L.; Rotunno, C.; Arcuri, E.; Gallese, V. Mirror neurons 30 years later: Implications and applications. Trends Cogn. Sci. 2022, 26, 767–781.
- Lahuerta-Martín, S.; Llamas-Ramos, R.; Llamas-Ramos, I. Effectiveness of Therapies Based on Mirror Neuron System to Treat Gait in Patients with Parkinson’s Disease-A Systematic Review. J. Clin. Med. 2022, 11, 4236.
- Shimada, S. Multisensory and Sensorimotor Integration in the Embodied Self: Relationship between Self-Body Recognition and the Mirror Neuron System. Sensors 2022, 22, 5059.
- Thiebaut de Schotten, M.; Beckmann, C.F. Asymmetry of brain structure and function: 40 years after Sperry’s Nobel Prize. Brain Struct. Funct. 2022, 227, 421–424.
- Esteves, M.; Ganz, E.; Sousa, N.; Leite-Almeida, H. Asymmetrical Brain Plasticity: Physiology and Pathology. Neuroscience 2021, 454, 3–14.
- Alqadah, A.; Hsieh, Y.W.; Morrissey, Z.D.; Chuang, C.F. Asymmetric development of the nervous system. Dev. Dyn. 2018, 247, 124–137.
- Thieme, H.; Morkisch, N.; Mehrholz, J.; Pohl, M.; Behrens, J.; Borgetto, B.; Dohle, C. Mirror therapy for improving motor function after stroke. CDSR 2018, 7, CD008449.
- Lucena-Anton, D.; Fernandez-Lopez, J.C.; Pacheco-Serrano, A.I.; Garcia-Munoz, C.; Moral-Munoz, J.A. Virtual and Augmented Reality versus Traditional Methods for Teaching Physiotherapy: A Systematic Review. Eur. J. Investig. Health Psychol. Educ. 2022, 12, 1780–1792.
- Keshner, E.A.; Fung, J. The quest to apply VR technology to rehabilitation: Tribulations and treasures. J. Vestib. Res. 2017, 27, 1–5.
- Levin, M.F.; Weiss, P.L.; Keshner, E.A. Emergence of virtual reality as a tool for upper limb rehabilitation: Incorporation of motor control and motor learning principles. Phys. Ther. 2015, 95, 415–425.
- Lee, H.K.; Jin, J. The effect of a virtual reality exergame on motor skills and physical activity levels of children with a developmental disability. Res. Dev. Disabil. 2023, 132, 104386.
- Ferrero, L.; Ortiz, M.; Quiles, V.; Iáñez, E.; Flores, J.A.; Azorín, J.M. Brain Symmetry Analysis during the Use of a BCI Based on Motor Imagery for the Control of a Lower-Limb Exoskeleton. Symmetry 2021, 13, 1746.
- Cano Porras, D.; Siemonsma, P.; Inzelberg, R.; Zeilig, G.; Plotnik, M. Advantages of virtual reality in the rehabilitation of balance and gait. Systematic review. Neurology 2018, 90, 1017–1025.
- Brunner, I.; Skouen, J.S.; Hofstad, H.; Aßmuss, J.; Becker, F.; Pallesen, H.; Thijs, L.; Verheyden, G. Is upper limb virtual reality training more intensive than conventional training for patients in the subacute phase after stroke? An analysis of treatment intensity and content. BMC Neurol. 2016, 16, 219.
- Negut, A.; Jurma, A.M.; David, D. Virtual-reality-based attention assessment of ADHD: ClinicaVR: Classroom-CPT versus a traditional continuous performance test. Child Neuropsychol. 2017, 23, 692–712.
- Buxbaum, L.J.; Dawson, A.M.; Linsley, D. Reliability and validity of the Virtual Reality Lateralized Attention Test in assessing hemispatial neglect in right-hemisphere stroke. Neuropsychology 2012, 26, 430–441.
- Allain, P.; Foloppe, D.A.; Besnard, J.; Yamaguchi, T.; Etcharry-Bouyx, F.; Le Gall, D.; Nolin, P.; Richard, P. Detecting everyday action deficits in Alzheimer’s disease using a nonimmersive virtual reality kitchen. J. Int. Neuropsychol. Soc. 2014, 20, 468–477.
- Sokołowska, B. A Novel Perspective for Examining and Comparing Real and Virtual Test Tasks Performed by the Dominant and Non-Dominant Hand in Healthy Adults. Symmetry 2021, 13, 1810.
- Sokołowska, B. A novel virtual reality approach for functional lateralization in healthy adults. Brain Res. 2021, 1766, 147537.
- Sokołowska, B.; Sokołowska, E. An Example of the Assessment of Human Laterality Using Virtual Reality. IJIRCCE 2019, 7, 3555–3562. Available online: http://ijircce.com/admin/main/storage/app/pdf/KdxZlKhLTCPJ5Fekz5R9wfuhT7qtfDYfS9dn2Atb.pdf (accessed on 24 February 2023).
- Sokołowska, B.; Sokołowska, E. Machine Learning algorithms to study of laterality in Virtual Reality. In Proceedings of the annual INCF Congress of NeuroInformatics 2019, Warsaw, Poland, 1–2 September 2019.
- Msika, E.F.; Ehrlé, N.; Gaston-Bellegarde, A.; Orriols, E.; Piolino, P.; Narme, P. Using a Computer-Based Virtual Environment to Assess Social Cognition in Aging: An Exploratory Study of the REALSoCog Task. Front. Psychol. 2022, 13, 882165.
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Everyday Assessment Lab (VR-EAL): An Immersive Virtual Reality Neuropsychological Battery with Enhanced Ecological Validity. J. Int. Neuropsychol. Soc. 2021, 27, 181–196.
- Kourtesis, P.; MacPherson, S.E. An ecologically valid examination of event-based and time-based prospective memory using immersive virtual reality: The influence of attention, memory, and executive function processes on real-world prospective memory. Neuropsychol. Rehabil. 2021, 29, 486–506.
- Aubin, G.; Béliveau, M.F.; Klinger, E. An exploration of the ecological validity of the Virtual Action Planning-Supermarket (VAP-S) with people with schizophrenia. Neuropsychol. Rehabil. 2018, 28, 689–708.
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest-posttest design pilot study. BMC Res. Notes 2019, 12, 776.
- Stryla, W.; Banas, A. The Use of Virtual Reality Technologies during Physiotherapy of the Paretic Upper Limb in Patients after Ischemic Stroke. J. Neurol. Neurosci. 2015, 6, 33.
- Zhang, Y.; Xing, Y.; Li, C.; Hua, Y.; Hu, J.; Wang, Y.; Ya, R.; Meng, Q.; Bai, Y. Mirror therapy for unilateral neglect after stroke: A systematic review. Eur. J. Neurol. 2022, 29, 358–371.
- Porffy, L.A.; Mehta, M.A.; Patchitt, J.; Boussebaa, C.; Brett, J.; D’Oliveira, T.; Mouchlianitis, E.; Shergill, S.S. A Novel Virtual Reality Assessment of Functional Cognition: Validation Study. J. Med. Internet Res. 2022, 24, e27641.
- Kourtesis, P.; MacPherson, S.E. How immersive virtual reality methods may meet the criteria of the National Academy of Neuropsychology and American Academy of Clinical Neuropsychology: A software review of the Virtual Reality Everyday Assessment Lab (VR-EAL). Comput. Hum. Behav. Rep. 2021, 4, 100151.
- Nath, D.; Singh, N.; Saini, M.; Srivastava, M.V.P.; Mehndiratta, A. Design and Validation of Virtual Reality Task for Neuro-Rehabilitation of Distal Upper Extremities. Int. J. Environ. Res. Public Health 2022, 19, 1442.
- Rey, B.; Oliver, A.; Monzo, J.M.; Riquelme, I. Development and Testing of a Portable Virtual Reality-Based Mirror Visual Feedback System with Behavioral Measures Monitoring. Int. J. Environ. Res. Public Health 2022, 19, 2276.
- Brassel, S.; Power, E.; Campbell, A.; Brunner, M.; Togher, L. Recommendations for the Design and Implementation of Virtual Reality for Acquired Brain Injury Rehabilitation: Systematic Review. J. Med. Internet Res. 2021, 23, e26344.
- Bell, I.H.; Nicholas, J.; Alvarez-Jimenez, M.; Thompson, A.; Valmaggia, L. Virtual reality as a clinical tool in mental health research and practice. Dialogues Clin. Neurosci. 2020, 22, 169–177.
- Kourtesis, P.; Korre, D.; Collina, S.; Doumas, L.A.; Macpherson, S.E. Guidelines for the Development of Immersive Virtual Reality Software for Cognitive Neuroscience and Neuropsychology: The Development of Virtual Reality Everyday Assessment Lab (VR-EAL), a Neuropsychological Test Battery in Immersive Virtual Reality. Front. Comput. Sci. 2020, 1, 12.
- Cavedoni, S.; Cipresso, P.; Mancuso, V.; Bruni, F.; Pedroli, E. Virtual reality for the assessment and rehabilitation of neglect: Where are we now? A 6-year review update. Virtual Real. 2022, 30, 1663–1704.
- Giannakou, I.; Lin, D.; Punt, D. Computer-based assessment of unilateral spatial neglect: A systematic review. Front. Neurosci. 2022, 16, 912626.
- Cogné, M.; Taillade, M.; N’Kaoua, B.; Tarruella, A.; Klinger, E.; Larrue, F.; Sauzéon, H.; Joseph, P.A.; Sorita, E. The contribution of virtual reality to the diagnosis of spatial navigation disorders and to the study of the role of navigational aids: A systematic literature review. Ann. Phys. Rehabil. Med. 2017, 60, 164–176.
- Jonson, M.; Avramescu, S.; Chen, D.; Alam, F. The Role of Virtual Reality in Screening, Diagnosing, and Rehabilitating Spatial Memory Deficits. Front. Hum. Neurosci. 2021, 15, 628818.
- Kaplan, A.D.; Cruit, J.; Endsley, M.; Beers, S.M.; Sawyer, B.D.; Hancock, P.A. The Effects of Virtual Reality, Augmented Reality, and Mixed Reality as Training Enhancement Methods: A Meta-Analysis. Hum. Factors 2021, 63, 706–726.