1. Cosmetic and Plastic Surgery
Cosmetic and plastic surgical procedures are performed on both healthy individuals and injured patients by using clinical interventions and artistic creativity to improve the patient’s appearance and body image
[1][2]. According to the 2020 American Society of Plastic Surgeons (ASPS) statistics report, 15.6 million cosmetic surgeries and about 13.2 million minimally-invasive surgeries are performed each year in the United States
[3]. Common cosmetic procedures include rhytidectomy (facelifts), strabismus surgery (correction of eye muscles and droopy eyelids or ptosis repair), rhinoplasty (nose correction), abdominoplasty (tummy-tucks), and breast augmentation and reduction procedures
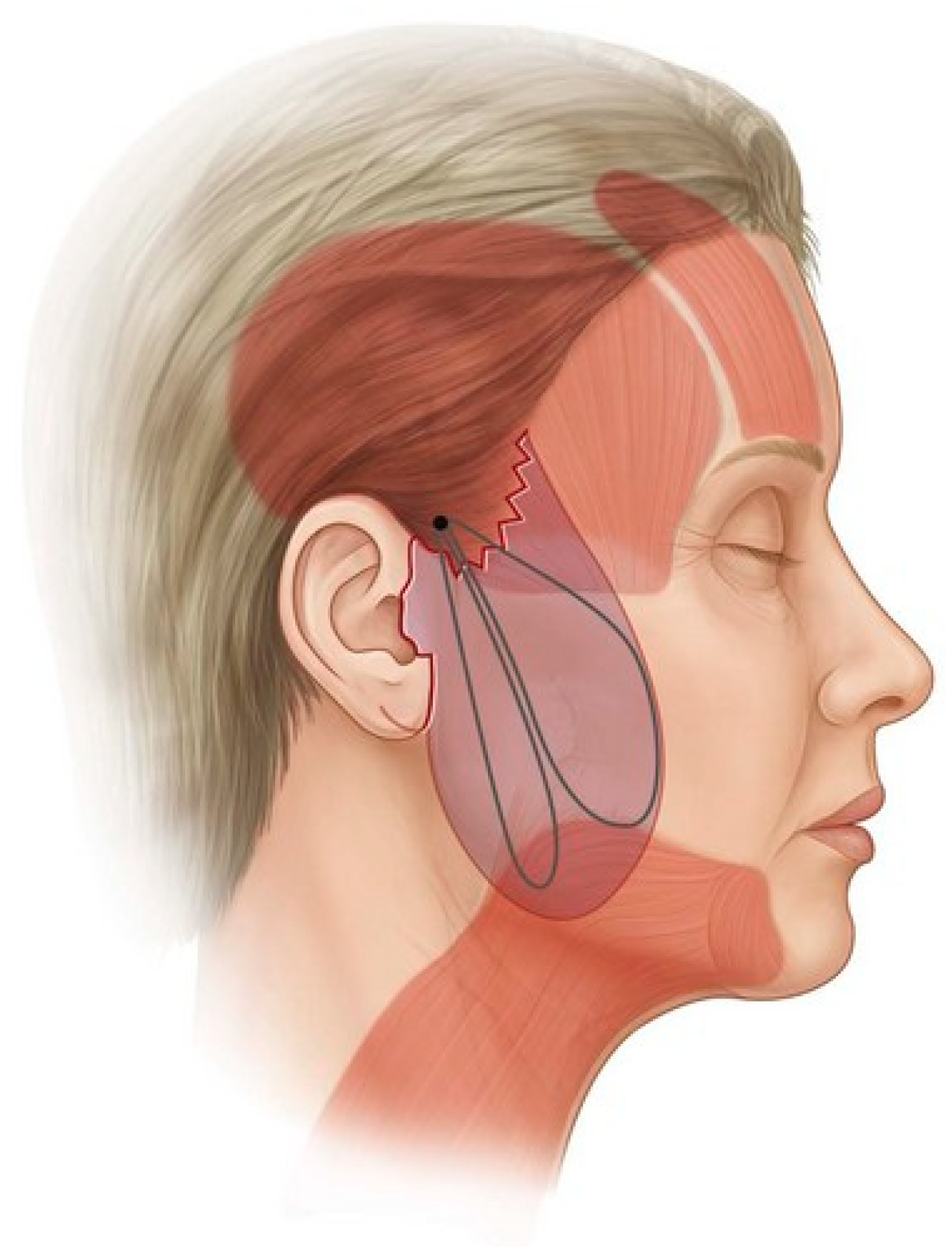
[4]. A suture suspension approach is the most commonly used technique to reconstruct loose and flabby tissue to a tighter and younger-looking appearance during cosmetic surgery. One of the classical suspension techniques is superficial muscle aponeurotic suspension (SMAS), which is also known as rhytidectomy. In this suspension approach, the face muscles are tightened by removing excess skin and fat. An alternative and less invasive technique is the minimal access cranial suspension (MACS), as presented in
Figure 1, where the suture is anchored in the deep temporal fascia, and suture loops are inserted to elevate the loose and sagging tissues. This technique involves much less skin excision and is less complicated when compared to the SMAS lift
[1][5][6]. Since the development of barbed sutures, these cosmetic surgical procedures have been performed using barbed sutures since they exhibit better surgical outcomes and less scarring compared to conventional sutures.
Table 1 lists the various modified sutures that are currently, or have previously been, used in cosmetic and plastic surgical operations.
Figure 1. Basic MACS lift where the suture is anchored in deep temporal fascia and sutures are looped in a purse-string fashion
[6].
Table 1. Comparison of different available barbed suture devices (Highlighted rows: Currently used commercial barbed sutures available for different surgical procedures).
The use of bidirectional barbed sutures instead of conventional monofilament sutures has obvious advantages of increased speed of placement, easier handling and the freedom from tying knots, as seen in the purse-string effect. Several clinical studies were performed in order to understand the clinical significance and efficacy of barbed sutures, and it was reported by all the surgeons that the use of barbed sutures significantly reduced the closure time when compared to traditional sutures. Procedures such as abdominoplasty, brachioplasty (upper arm lift) and mastopexy (breast lift) require the approximation of three layers of tissue, namely the superficial fascia/deep tissue, deep dermis and superficial dermis. The approximation of these three layers using a traditional suturing technique with conventional sutures requires three separate sutures, but when using bidirectional barbed sutures, only two running sutures are required, and the closure time is reduced by approximately 50%.
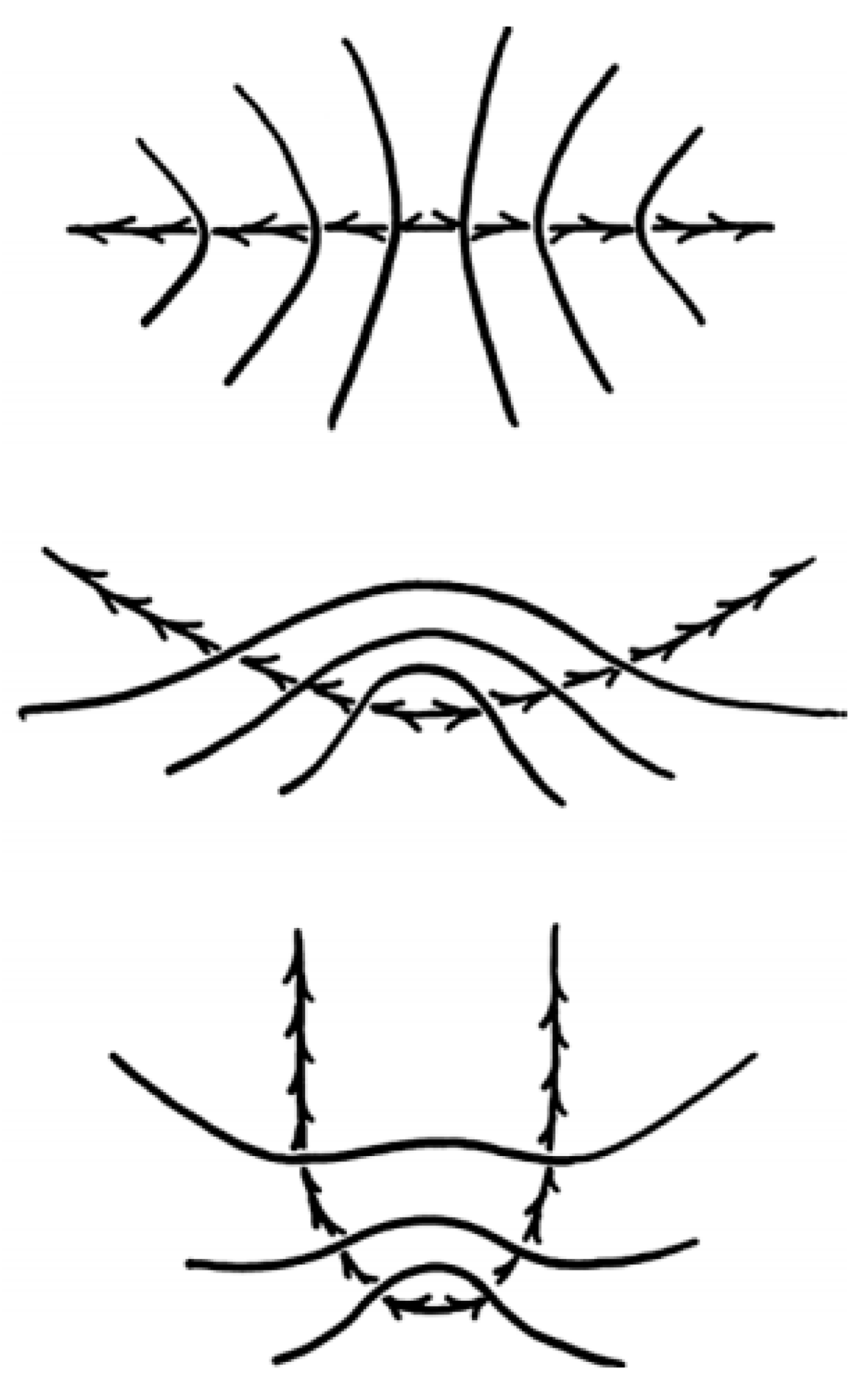
Figure 2 represents the gradients of tension experienced by the surrounding tissues when a bi-directional barbed suture is deployed during tissue approximation
[7].
Figure 2. Gradients of tension experienced by the surrounding tissues. Linear compression at the point where the barbs change direction (
top); Accurate placement imparts a mound by adding a vertical vector to the horizontal vector (
middle) and U-shaped deployment results in the forces on the barbs being opposed by the bend in the U, rather than by the opposing barbs (
bottom)
[5][7].
Innovative barbed surgical sutures play an important role in “lunch-time” facelift procedures since patients prefer the least invasive or non-invasive surgeries. Facial rejuvenation for transforming facial aging has evolved from tension-based procedures such as mini facelifts to various subcutaneous, sub-SMAS and sub-periosteal planes of dissection. Atiyeh et al. investigated the efficacy of barbed sutures used for “lunch-time” facelift surgeries. The “lunch-time” facelift surgery is a procedure that avoids large incisions, significant undermining or substantial recovery time. The study was focused on the different variations of barbed sutures, namely short Aptos
TM threads (Tbilisi, Georgia) for Aptos
TM lift or Feather lift procedures, long Woffles threads (Kolster Methods Inc., Corona, CA, USA) that were preferred for suspension of sagging tissues and Contour
TM threads with unidirectional barbs and an anchor loop on one end, which are known as Feather lift extended Aptos
TM length threads, that were used in different facial rejuvenation surgeries in earlier days when barbed sutures were introduced as an alternative to conventional filaments. It was mentioned that barbed sutures are used in facial aesthetic surgeries, which involve the lifting of brows, midface, lower face and neck. The minor complications that were reported due to the use of barbed sutures were mild facial asymmetry, swelling, erythema, hematoma, slight discomfort and scar formation at the entry and exit sites. When Contour
TM threads were used for the facelift procedures, there were noticeable ecchymosis and swelling, which persisted for many days, if not weeks. The study concluded that the use of barbed sutures could be an alternative tool for lifting ptosis tissues, but the preferred use is in open surgical procedures. The choice of barbed sutures requires careful evaluation and acceptance during open rather than laparoscopic procedures
[8].
Kaminer et al. investigated the long-term efficacy of barbed sutures for minimally invasive thread-lift procedures. They studied the efficacy of Aptos
TM threads and the modified Aptos
TM threads (Isse Endo Progressive Face Lift Suture
®) (Tbilisi, Georgia), which are unidirectional polypropylene sutures used in facelift surgical procedures. It was found in this research that patients prefer surgeries that have high-quality results, as found in facelifts, which have less risk and downtime. The study was conducted to understand if the unidirectional and anchored sutures had a long-lasting lifetime in order to support the aging of the skin. The results were in favor of the barbed sutures, as they provide support for a period of 16 months with higher patient satisfaction in contrast to monofilament or braided sutures
[9].
Cortez et al. reported a study that investigated complications following the use of barbed sutures for wound closure during plastic surgeries or other cosmetic reconstructions. In their study, they compared the two major commercial barbed sutures available at the time of their study, which were the Quill
TM (Corza Medical Inc., Westwood, MA, USA) barbed suture and the V-Loc
TM (Medtronic, New Haven, CT, USA) suture. The study involved patients who had undergone breast reconstruction, body contouring and complex free-flap surgical procedures. The study involved both 1-layer closure and 2-layer closure using barbed sutures, which were compared with the same procedure performed using conventional sutures. They reported that the use of barbed sutures reduced the risk of surgical site infections since conventional sutures lead to wound dehiscence, secondary to knot failure and slippage. In this research, they also observed that conventional sutures (mainly braided sutures) have a greater affinity for bacterial adhesion in the interstices resulting in an inflammatory response from the host immune system, unlike the barbed sutures, where there is no specific location along the suture line, which acts like a bacterial attachment site. They summarized that the use of barbed sutures in cosmetic surgeries was advantageous over conventional sutures in terms of surgical risks and outcomes
[10].
Barbed sutures are used in reconstructive and plastic surgeries since they help surgeons with effective and faster dermal approximation and enable better tissue adherence and support both during and after the procedure. While using barbed sutures, surgeons also found that less suture material was required while closing the dermal tissues, and less operative time was involved in contrast to traditional sutures.
2. Obstetric and Gynecological Procedures and Gastrointestinal Surgeries
Barbed sutures have an interesting application in laparoscopic and plastic surgery due to their handling properties. They have been proven effective for performing end-to-end anastomosis ex vivo procedures
[11]. One of the most common gynecological procedures where barbed sutures are used is cesarean surgery or the C-section procedure. One other type of procedure which has been gaining attention recently is the laparoscopic procedure with suturing using a laparoscope. While using a laparoscope, the requirement of tying knots would increase the operative time since it is difficult to place knots while performing laparoscopic procedures. The introduction of barbed sutures has improved laparoscopic procedures as they do not require knots to be placed in order to engage with the surrounding tissues. Some surgeries, such as closing the vaginal cuff during total hysterectomy, have benefitted from the use of barbed sutures, where the closure time is reduced by approximately 40–50% when compared to closing the cuff using traditional monofilament or braided sutures
[7].
Guisto et al. conducted an analysis to compare the suturing techniques and surgical outcomes of two different barbed sutures, namely the unidirectional versus the bidirectional barbed suture, which were, in turn, compared to the traditional monofilament suture. Investigators reviewed earlier studies to find that the use of unidirectional barbed sutures had a higher risk of inflammatory response and were more susceptible to complications than bidirectional barbed sutures. The complications were due to the extended suture with barbs visible and present at the end of the suture point. The researchers mentioned that barbed sutures were safe and effective to be used for end-to-end anastomoses, and the results were coincidental with a lot of other results published by surgeons and researchers on barbed suture efficacy and safety to be used in different clinical applications. Similar to the results published by surgeons previously, investigators of this research also reported that the use of bidirectional barbed sutures was easier, provided less drag and significantly reduced the operating time. In conclusion, they mentioned that barbed sutures could be used in appositional, extra mucosal anastomoses since they promoted anastomotic healing and suture anchoring capacity together with a reduction in surgical operating time
[11].
Greenberg and Einarsson reported that the use of bidirectional barbed sutures in laparoscopic and gynecological procedures was beneficial to both surgeons and patients. Barbed sutures help in tissue approximation during laparoscopic surgeries since, during these procedures, tissue approximation is difficult, and the tying of knots is arduous and cumbersome. Even though these surgeries have relied for many years on the tying of traditional suture knots, the introduction of the barbed sutures was ground-breaking and created significantly improved surgical results compared to conventional monofilament sutures. When the post-surgical outcomes associated with clinical ligations were evaluated, both surgeons and patients recognized the benefits of using barbed sutures initially in terms of excellent hemostasis. The use of barbed sutures also reduced tissue trauma since tension is evenly distributed throughout the suture line in contrast to conventional sutures, where the tension is primarily confined to the knots. It was also reported that the bidirectional barbed sutures outshone the same size conventional suture materials in both tensile strength and wound holding capacity as measured in terms of anchoring with the surrounding tissue. Greenberg and Einarsson envisioned that, because of the advantages for both surgeons and patients, the clinical applications for barbed sutures would increase for total laparoscopic hysterectomies, myomectomies and other gynecological procedures
[12][13]. Selvest et al. compared the surgical outcomes of vaginal cuff closure during total laparoscopic hysterectomies while using both conventional and barbed sutures. At the end of the comparative study, they concluded that barbed sutures exhibited superior surgical outcomes and performance in comparison to conventional sutures
[14].
Demyttenaere et al. studied the advantages and complications of V-Loc
TM advanced wound closure devices (Medtronic, New Haven, CT) when used in laparoscopic surgery. In their study, the researchers investigated the post-surgical outcomes of using V-Loc
TM sutures in gastrointestinal enterotomy closures. As mentioned earlier, laparoscopic surgery is a surgical technique that involves suturing with limited visualization and thereby requires wound closure devices or sutures that are easier to tie knots both at the incision and at the exit of the suture line. These V-Loc
TM sutures are unidirectional barbed sutures that can be utilized for enterotomy closure during different laparoscopic surgeries. It was found that the enterotomy closure time, or anastomotic time, was significantly reduced and faster when V-Loc
TM sutures were used for suturing the jejunum, colon and stomach. In conclusion, Demyttenaere et al. reported that barbed sutures provide an efficient and effective alternative to conventional sutures for gastrointestinal surgical procedures
[15]. Huang et al. predicted the surgical outcomes of laparoscopic myomectomy when using two commercial sutures, QuillTM (Corza Medical Inc., Westwood, MA, USA) barbed suture and the V-LocTM (Medtronic, New Haven, CT) suture. The authors mentioned that the use of barbed sutures reduced the surgical time and also improved the surgical outcomes of the procedure
[16].
Giampaolino et al. studied the outcomes of laparoscopic myomectomy when performed using conventional sutures and the commercial bidirectional barbed sutures STRATAFIX
TM (Ethicon Inc., Somerville, NJ, USA). In this research, they compared the surgical outcomes of different types of sutures used during laparoscopic posterior myomectomy. Similar to the other studies, the researchers in this research concluded that the use of barbed sutures reduced the operating time, suturing time and blood loss, and there was no significant difference in postoperative adhesions between the two types of sutures
[17].
Barbed sutures are ideal for use during abdominoplasty because progressive tension sutures (PTS) are required to accommodate a drainage catheter. Gutowski et al. studied the safety and efficacy of incorporating barbed sutures during abdominoplasties. In their report, they compared the effects of Quill
TM sutures and V-Loc
TM sutures against nonabsorbable non-barbed sutures for their biomechanical performance, safety and effective use in different procedures involving abdominoplasties. In the discussion of the biomechanical performance of barbed sutures, they reported that there was no significant difference in the host tissue response, and barbed sutures were able to support the wound healing process by offering strength to the wound during the first post-surgical week when there are greater mechanical forces exerted on the wound. Along with the various advantages of barbed sutures that were reported in a number of clinical reviews, the investigators noted that suture placement of barbed sutures was easily understood and learned by surgeons during their training. Along with body contouring in abdominoplastic surgeries, barbed sutures are also used in arm-lift and thigh-lift procedures. The investigators concluded that barbed sutures are safe and effective to be used for both standard and circumferential abdominoplasty procedures and that they have a similar or superior biomechanical performance when compared with monofilament or braided sutures
[18].
Based on the reviews and studies published by surgeons following a number of clinical trials, it is now accepted that barbed sutures are safe, effective and efficient for use in different obstetric and gynecological procedures with acceptable patient comfort and surgeon satisfaction.
3. Orthopedic Procedures
Orthopedic arthroplasty involving barbed sutures has consistently shown reduced operating times, faster wound closure times and better surgical and postoperative outcomes when compared to conventional sutures
[7][19]. Barbed sutures are increasingly being used in orthopedic procedures since they have obvious advantages, including faster tying, more even distribution of retention forces throughout the suture line, and there is no need for complex instruments
[7].
Johnston et al. studied and reported on the advantages of barbed sutures over conventional sutures for spinal surgical procedures. There is limited evidence reporting the use of barbed sutures for closing incisions during spinal surgeries, but in those few cases, it has been reported that barbed sutures result in faster closure times and improved postoperative outcomes in comparison to using conventional sutures. Barbed sutures have shown promising outcomes when used to treat spine-related disorders such as spinal deformities, spinal infections, trauma, spinal tumors and degenerative spine conditions, such as stenosis and herniated disks. These latter conditions are some of the most prevalent musculoskeletal disorders which definitely require surgical intervention since non-invasive treatments have been reported to have no beneficial effects.
Johnston’s research group compared the results of surgery using conventional suture materials for suture line closures against the STRATAFIX
TM (Ethicon Inc., Somerville, NJ, USA) knotless tissue control device. The post-surgical performance was measured in terms of operating time, duration of postoperative stay, wound complications and readmissions in the unlikely case of any post-surgical incidents. In their study, they emphasized that successful suture line closure is an important factor regarding the postoperative outcome of spinal surgery because it influences healing, surgical-site infections (SSIs), the ability of patients to perform self-care and post-acute care follow up. Johnson et al. reported that barbed sutures had proven efficient for subcutaneous wound closure in spinal surgical interventions. The researchers reported that the STRATAFIX
TM knotless barbed suture provided superior performance compared to conventional sutures in terms of operating room time and postoperative outcomes. Having said that, they found no significant difference in suture line complications or readmissions after surgery
[19].
More recently, Shah et al. reported on the use of barbed sutures in tenorrhaphy and surgical procedures that repair injured tendons. The use of barbed sutures in tendon repair has been reported to have comparable outcomes with regard to appearance, reduced wound scarring, tissue approximation and the risk of dehiscence. The use of barbed sutures reduced localized tissue trauma with respect to the distribution of retention forces along the entire length of the implanted suture. In this research, the authors reviewed the use of barbed sutures (Quill
TM and V-Loc
TM) in tenorrhaphy compared to conventional non-barbed sutures. Their report was based on the following criteria: maximum load to failure, mode of failure, load to 2 mm gap formation, type of repair, changes in the cross-sectional shape, and the type of repair involved. It was explained that the use of non-barbed sutures that require knots for device placement led to the generation of high stresses at the knots themselves. The presence of knots increases the cross-sectional area of the tendon and increases the frictional resistance within the surrounding tissue. The investigators also performed a maximum pull-out force test on barbed and non-barbed sutures for tendon repair and determined that due to a more uniform distribution of anchoring force throughout the suture line, the barbed sutures exhibited a higher maximum pull-out load compared to traditional sutures. So even though the concept of using barbed sutures for tenorrhaphy is not widely accepted, the authors believe that due to their superior performance, barbed sutures can be used successfully to replace traditional non-barbed sutures for tendon repair
[20][21].
Wang et al. studied barbed sutures with a symmetric anchoring design and conventional interrupted sutures for total knee arthroplasty (TKA). In particular, they compared the wound closure efficacy and safety of the symmetric anchoring suture (STRATAFIX
TM Symmetric PDS
TM Plus, Ethicon Inc., Somerville, NJ) with conventional sutures when used in a TKA procedure. From previous meta-analyses, barbed sutures resulted in shorter operating times and improved cost-effectiveness even when there were similar rates of wound complications as with conventional sutures. When interrupted sutures were used for TKA procedures, there was relatively low suture efficacy reported. The use of barbed sutures diminished the risk of complications at the incision, reduced wound dehiscence and lowered the risk of local tissue ischemia and hematomas. Researchers in this research determined the efficacy and safety of barbed sutures using primary and secondary endpoints, which included surgical incision closure time, operating time, total operating room time, length of post-surgical stay, as well as the level of pain and range of motion of the post-surgical knee joint. The symmetrically anchored design of barbed sutures eliminated the need to tie knots at the end of the suture line. These barbed sutures reduced surgical incision closure time and achieved faster arthrotomy closure times as well as fewer complications compared to conventional sutures. These advantages made the use of barbed sutures a desirable option for TKA since TKA procedures require surgeons to quickly close the wound so as to decrease the risk of infections at the surgical site. It was also evident that the use of barbed sutures increased the blood flow since they can achieve a more even distribution of stress which reduces tissue trauma during the surgery and facilitates easier and more extensive joint motion after the surgery
[22][23].
Mayet et al. studied the use of barbed sutures in foot and ankle procedures. More specifically, the researchers evaluated the use of the Quill
TM (Corza Medical Inc., Westwood, MA, USA) barbed suture as a locking suture for these repair surgeries. In a previous clinical study, Chowdry et al. reported poor wound closure and severe scar formation involved in foot surgery when using the V-Loc 180
TM barbed suture (Medtronic, New Haven, CT, USA)
[24]. In contrast, Mayet et al. reported that Quill
TM barbed sutures in foot surgery achieved better surgical outcomes and lower wound complications. V-Loc
TM sutures are unidirectional barbed sutures with a loop at one end and barbs all unidirectionally aligned, whereas the Quill
TM sutures are bidirectional barbed sutures. Post-surgical complications have been reported, which include suture extrusion, suture visibility, a severe inflammatory response and infection. These complications are thought to depend on the suture material and its chemical composition. In the case of barbed sutures, such complications are also influenced by the barb geometry as well as the frequency and alignment of the barbs. The limitation of this research is that the barbed sutures were made from different materials, which behaved differently in terms of their degradation and absorption rates within the surrounding host tissue. For this reason, the clinical observations of these barbed sutures cannot be directly compared to other studies. In conclusion, the authors reported that these Quill
TM sutures are safe and effective to use in foot and ankle surgeries resulting in both higher patient and surgeon satisfaction
[25].
Even though barbed sutures have various advantages over conventional sutures in orthopedic surgeries, the mechanical properties of barbed sutures are lower than conventional sutures. In the case of orthopedic surgeries, the sutures should have higher breaking strength since the stresses applied in these joint locations are higher compared to other locations of the body. Although barbed sutures do not possess the required mechanical strength, they are still being used in joint replacement surgeries as they are easily deployed in intricate areas without the requirement of knots during placement.
This entry is adapted from the peer-reviewed paper 10.3390/bioengineering10040419