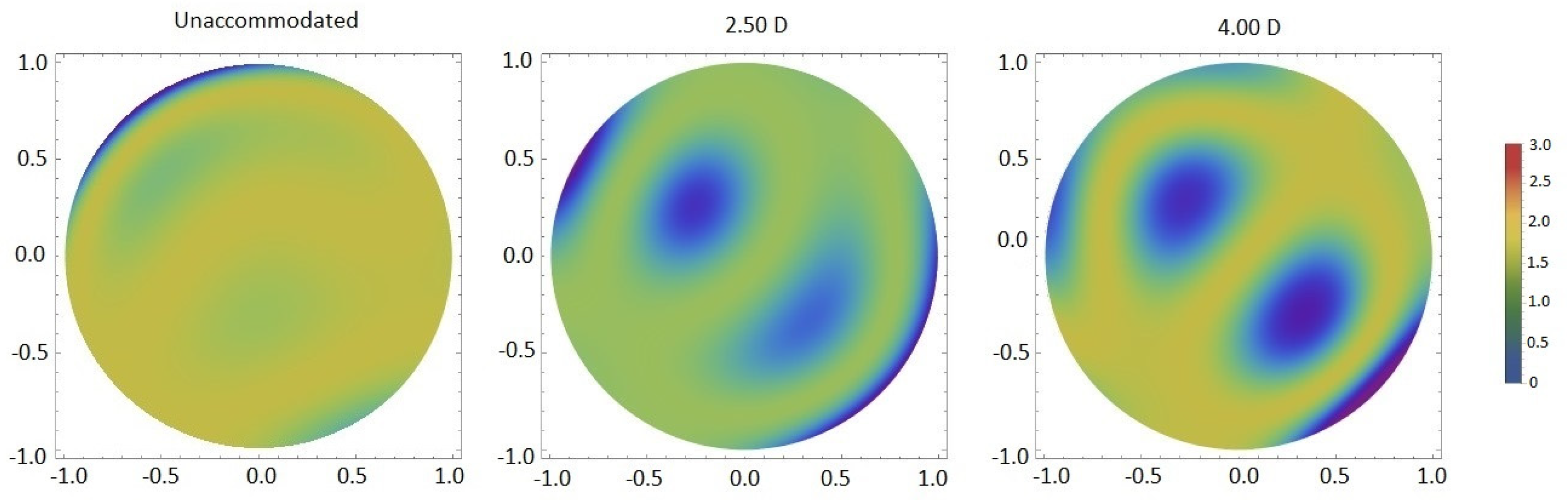
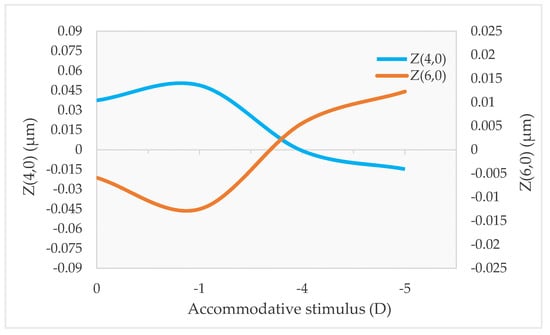
High-order aberrations (HOAs) are optical defects that degrade the image quality. They change with factors such as pupil diameter, age, and accommodation. The changes in optical aberrations during accommodation are mainly due to lens shape and position changes. Primary spherical aberration (Z(4.0)) is closely related to accommodation and some studies suggested that it plays an important role in the control of accommodation. Furthermore, central and peripheral HOAs vary with refractive error and seem to influence eye growth and the onset and progression of myopia. The variations of central and peripheral HOAs during accommodation also appear to be different depending on the refractive error. Central and peripheral high-order aberrations are closely related to accommodation and influence the accuracy of the accommodative response and the progression of refractive errors, especially myopia.
- aberrations
- accommodation
- refractive error
1. Introduction
2. Central HOAs and Accommodation
| Author (Year) | Eyes | Age (Years) | Refractive State (D) | Accommodative Stimulus (D) | Accommodation Stimulation Method | Measurement Method |
|---|---|---|---|---|---|---|
| Atchison et al. (1995) [13] | 15 | 0D, 1.5D and 3.00D | Aberroscope | |||
| He et al. (2000) [8] | 8 | 24–38 | SEQ: −2.00D–−5.56D | Between 0 and 6.00D in steps of 1.00D | Spatially resolved refractometer | |
| Ninomiya et al. (2002) [14] | 33 | 28.7 ± 4.4 | 0 and 3.00D | TDV | S-H | |
| He et al. (2003) [15] | 12 | 23–32 | SEQ: 0–−3.00D; Cil ≤ 0.25D | 0.25D and 5.00D | TDV | CTS |
| Hazel et al. (2003) [16] | 30 | 18–27 | SEQ: +0.50D–−6.00D; Cil < 0.50D | Between 0 and 4.00D in steps of 1.00D | NSL | S-H |
| Cheng et al. (2004) [9] | 76 | 21–40 | Sphere: +1.25D–−8.25D; Cil: −0.25D–−2.75D | 0, 3.00D and 6.00D | TDV | S-H |
| Gicquel et al. (2005) [17] | 28 | 20–25 | SEQ: −2.00D–+1.00D | Between 1.00D and 5.00D in steps of 0.50D | TDV | S-H |
| Plainis et al. (2005) [6] | 7 | 23–33 | Emmetropes; Myopes with sphere: −2.00D–−2.50D | Between 0D and 8.00D in steps of 1.00D | TDV | S-H |
| Buehren et al. (2006) [10] | 10 | 22–36 | Sphere: emmetropes +0.05D ± 0.19D; myopes −2.25D ± 0.85D Cil for both: −0.30D ± 0.45D |
0.17D, 1.00D, 2.00D, 3.00D, 4.00D and 5.00D | TDV | S-H |
| Wang et. al (2007) [18] | 20 | 18–32 | Sphere: −6.00D–+3.00D | Between 0 and −4.00D in steps of 1.00D | TDV | S-H |
| López-Gil et al. (2008) [19] | 24 | 19–29 | Sphere: −3.00D–+3.00D; Cil <1.00D | Between 0 and 5.00D in steps of 0.50D | TDV | S-H |
| López-Gil et al. (2010) [20] | 15 | 20–38 | Sphere: 0.38D–−3.06D; Cil: −0.38D ± 0.25D | Between 0.50D and 9.50D in steps of 0.50D | Badal | S-H |
| Fritzsch et. al (2011) [21] | 25 | 15–27 | Emmetropes | 0.22D and 5.00D | TDV | S-H |
| Yuan et al. (2013) [22] | 35 | 20–33 | SEQ: +0.50D–−2.38D; Cil <0.75D | 0.25D and 3.00D | TDV | S-H |
| Zhou et al. (2015) [12] | 22 | 18–28 | Sphere: 0D–−1.00D; Cil: −0.75D and 0D | Between 1.00D and 6.00D in steps of 1.00D | NSL | S-H |
| Wang et al. (2015) [11] | 10 | 0 and 3.00D | TDV | S-H |
2.1. Z(4,0), Z(6,0) and Accommodation
2.2. Other Zernike Terms and Accommodation
2.3. Z(4,0), Z(6,0) and Accommodative Lag
2.4. Total, Corneal, and Internal HOAs during Accommodation
This entry is adapted from the peer-reviewed paper 10.3390/vision7010019
References
- Collins, M.J.; Wildsoet, C.F. Monochromatic aberrations and myopia. Vis. Res. 1995, 35, 1157–1163.
- Hiraoka, T.; Kakita, T.; Okamoto, F.; Oshika, T. Influence of ocular wavefront aberrations on axial length elongation in myopic children treated with overnight orthokeratology. Ophthalmology 2015, 122, 93–100.
- Osuagwu, U.L.; Suheimat, M.; Atchison, D.A. Peripheral aberrations in adult hyperopes, emmetropes and myopes. Ophthalmic Physiol. Opt. 2017, 37, 151–159.
- Valentina, B.S.; Ramona, B.; Speranta, S.; Calin, T. The influence of optical aberrations in refractive surgery. Rom. J. Ophthalmol. 2015, 59, 217–222.
- López-Gil, N.; Rucker, F.J.; Stark, L.R.; Badar, M.; Borgovan, T.; Burke, S. and Kruger, Effect of third order aberrations on dynamic accommodation. Vis. Res. 2007, 47, 755–765.
- Plainis, S.; Ginis, H.S.; Pallikaris, A. The effect of ocular aberrations on steady-state errors of accommodative response. J. Vis. 2005, 5, 7.
- Li, Y.J.; Choi, J.A.; Kim, H.; Yu, S.Y.; Joo, C.K. Changes in ocular wavefront aberrations and retinal image quality with objective accommodation. J. Cataract Refract. Surg. 2011, 37, 835–841.
- He, J.C.; Burns, S.A. Monochromatic aberrations in the accommodated human eye. Vis. Res. 2000, 40, 41–48.
- Cheng, H.; Barnett, J.K.; Vilupuru, A.S.; Marsck, J.D.; Kasthurirangan, S.; Applegate, R.A.; Roorda, A. A population study on changes in wave aberrations with accomodation. J. Vis. 2004, 4, 272–280.
- Buehren, T.; Collins, M.J. Accommodation stimulus-response function and retinal image quality. Vis. Res. 2006, 46, 1633–1645.
- Wang, Y.; Shao, Y.; Yuan, Y. Simultaneously measuring ocular aberration and anterior segment biometry during accommodation. J. Innov. Opt. Health Sci. 2015, 8, 1550005.
- Zhou, X.Y.; Wang, L.; Zhou, X.T.; Yu, Z.Q. Wavefront aberration changes caused by a gradient of increasing accommodation stimuli. Eye 2015, 29, 115–121.
- Atchison, D.A.; Collins, M.J.; Wildsoet, C.F.; Christensen, J.; Waterworth, M.D. Measurement of monochromatic ocular aberrations of human eyes as a function of accommodation by the howland aberroscope technique. Vis. Res. 1995, 35, 313–323.
- Ninomiya, S.; Fujikado, T.; Kuroda, T.; Maeda, N.; Tano, Y.; Oshika, T.; Hirohara, Y.; Mihashi, T. Changes of ocular aberration with accommodation. Am. J. Ophthalmol. 2002, 134, 924–926.
- He, J.C.; Gwiazda, J.; Thorn, F.; Held, R.; Huang, W. Change in corneal shape and corneal wave-front aberrations with accommodation. J. Vis. 2003, 3, 456–463.
- Hazel, C.A.; Cox, M.J.; Strang, N.C. Wavefront aberration and its relationship to the accommodative stimulus-response function in myopic subjects. Optom. Vis. Sci. 2003, 80, 151–158.
- Gicquel, J.J.; Nguyen-Khoa, J.L.; Lopez-Gil, N.; Legras, R.; Dighiero, P.; Lebuisson, D.A.; Gargasson, J.F. Optical Aberrations Variations of the Human Eye During Accommodation. Investig. Ophthalmol. Vis. Sci. 2005, 46, 1993.
- Wang, Y.; Wang, Z.Q.; Guo, H.Q.; Wang, Y.; Zuo, T. Wavefront aberrations in the accommodated human eye based on individual eye model. Optik 2007, 118, 271–277.
- López-Gil, N.; Fernández-Sánchez, V.; Legras, R.; Montés-Micó, R.; Lara, F.; Nguyen-Khoa, J.L. Accommodation-related changes in monochromatic aberrations of the human eye as a function of age. Investig. Ophthalmol. Vis. Sci. 2008, 49, 1736–1743.
- López-Gil, N.; Fernández-Sánchez, V. The change of spherical aberration during accommodation and its effect on the accommodation response. J. Vis. 2010, 10, 12.
- Fritzsch, M.; Dawczynski, J.; Vollandt, R.; Strobel, J. Aberrationen höherer Ordnung bei Akkommodation. Ophthalmologe 2011, 108, 553–560.
- Yuan, Y.; Shao, Y.; Tao, A.; Shen, M.; Wang, J.; Shi, G.; Chen, Q.; Zhu, D.; Lian, Y.; Qu, J.; et al. Ocular Anterior Segment Biometry and High-Order Wavefront Aberrations During Accommodation. Investig. Ophthalmol. Vis. Sci. 2013, 54, 10.
- Moreno-Barriuso, E.; Merayo Lloves, J.; Marcos, S.; Navarro, R.; Llorente, L.; Barbero, S. Ocular aberrations before and after myopic corneal refractive surgery: LASIK-induced changes measured with laser ray tracing. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1396–1403.
- Theagarayan, B.; Radhakrishnan, H.; Allen, P.M.; Calver, R.I.; Rae, S.M.; O’Leary, D.J. The effect of altering spherical aberration on the static accommodative response. Ophthalmic Physiol. Opt. 2009, 29, 65–71.
- Shi, G.; Wang, Y.; Yuan, Y.; Wei, L.; Lv, F.; Zhang, Y. Measurement of ocular anterior segment dimension and wavefront aberration simultaneously during accommodation. J. Biomed. Opt. 2012, 17, 120501.
- Tabernero, J.; Benito, A.; Alcón, A.; Artal, P. Mechanism of compensation of aberrations in the human eye. J. Opt. Soc. Am. A 2007, 24, 3274.
- Franco, S.; Gomes, J.; Gonçalves, A. Compensation effect between corneal and internal ocular aberrations during a computer task. In Proceedings of the Fourth International Conference on Applications of Optics and Photonics, Lisbon, Portugal, 31 May–4 June 2019; p. 11207.