2. Central HOAs and Accommodation
The quality of the retinal image change with accommodation has been already verified [
7,
8,
9,
10,
11,
12]. Atchison et al. [
13] investigated in detail the changes of ocular aberrations of the eye as a function of accommodation. Monochromatic aberrations were analyzed in 15 subjects in 3 different levels of accommodation (0D, 1.50D, and 3.00D). Although the spherical aberration (Z(4,0)) became more negative with accommodation in eight subjects, there was not a clear trend in the amount and direction of changes for other aberrations. The sample size and substantial variability in aberrations between individuals may influence the results.
Further studies were carried out and, although the variability between individuals was verified in several studies [
8,
9,
12,
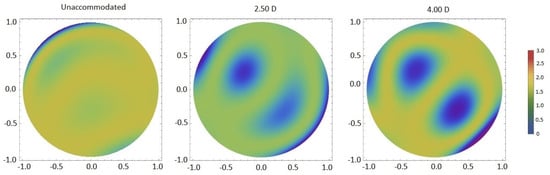
14], it was shown that aberrations tend to become larger for a high level of accommodation (
Figure 1) [
8,
9,
10,
11,
12]. Some studies analyzed these variations only between the relaxed state and for a given accommodative demand, whereas others investigated different accommodative levels (
Table 1). Root-mean-square (RMS) reaches a minimum close to a relaxed state, remaining constant from 0D to 3.00D of accommodation, and increases for high accommodative demands (
Figure 1) (
p < 0.05). [
6,
8,
9,
10,
12]. In the relaxed state, most wavefront aberrations are approximately 0, except Z(4,0) (which is usually positive), and increase gradually for higher accommodative levels (from 3.00D) [
6,
8,
9,
10,
12] with a relevant increase at 5.00D of accommodation (
Figure 1) [
10].
Figure 1. Wavefront aberration maps of total HOAs for three accommodative stimuli.
Table 1. Methodological characteristics of articles where wavefront aberrations were measured during accommodation.
All these findings were similar for different accommodative stimulation methods, i.e., when the target was approximated to stimulate accommodation or when negative lenses were used (Table 1).
According to all these studies, accommodation and the optical quality of the eye are closely related.
2.1. Z(4,0), Z(6,0) and Accommodation
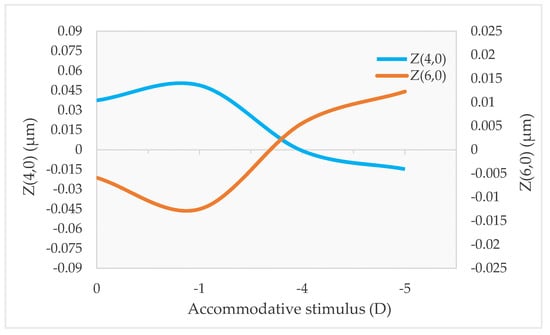
Z(4,0) is the aberration that shows the clearest trend with accommodation. When the accommodative system is relaxed, Z(4,0) is usually positive, and when accommodation is stimulated, it becomes less positive or more negative (
Figure 2) [
6,
7,
8,
9,
10,
12,
14,
19,
20]. However, the change from positive to negative values is not observed in every subject, because some individuals already present negative Z(4,0) in the relaxed state [
6,
8]. Moreover, the amount of this change varies between individuals [
6,
8,
9,
12,
14,
20]. The reason for these differences has not been explored but is likely due to the lens’s natural shape, which may not be the same for all subjects. Age also affects this tendency of Z(4,0) to become more negative with accommodation, being more evident in older subjects [
19].
Figure 2. Change of Z(4,0) and Z(6,0) with accommodation for different accommodative demands.
There is evidence that secondary-spherical aberration (Z(6,0)) is also correlated with accommodation, but unlike Z(4,0), Z(6,0) tends to become more positive with accommodation (
Figure 2) [
12,
14,
20]. However, this effect is usually smaller than in Z(4,0), and it is not present in all subjects [
20]. Nevertheless, one study found a negatively shift in Z(6,0) with accommodation [
1], and others did not find a clear trend [
8,
9]. Again, it may depend on the shape of the lens.
It has been reported that spherical aberrations play an important role in the control of the accommodative response [
10,
20]. Therefore, it would be interesting to investigate how these aberrations behave in subjects with inaccurate accommodative responses, such as insufficiency, infacility, or excess accommodation. If the natural shape of the lens in some subjects leads to changes in spherical aberrations in a different direction than expected during accommodation, this could lead to inaccurate accommodative responses. It would also be important to understand the relationship between changes in the optical quality of the eye during accommodation and the occurrence of symptoms during near tasks.
Another area of clinical relevance is refractive surgery. Since the aberration profile changes with accommodation, the preoperative assessment for refractive surgery should be individualized and include aberrometry not only in the relaxed state but also during accommodation to ensure the optimal treatment profile, i.e., a balance between both states. According to previous studies [
4,
23], spherical aberration is the aberration that increases the most after refractive surgery due to the change in corneal asphericity induced by corneal ablation. Therefore, the analysis of spherical aberration in all accommodative states in the preoperative assessment is essential to optimize the far and near vision of subjects undergoing this treatment. Its impact on near vision must be simulated in patients and considered before surgery.
2.2. Other Zernike Terms and Accommodation
Other Zernike terms may change with accommodation and affect vision during near tasks and influence the accuracy of the accommodative response. Although the variability of aberrations among individuals is large, studies have shown that some Zernike terms also have a trend. Vertical and horizontal coma (Z(3,−1) and Z(3,1), respectively) seem to change to more positive values with accommodation, with Z(3,1) being more evident [
6]. Vertical secondary astigmatism (Z(4,2)) and Z(7,−7) also showed a tendency to more negative values with increasing accommodative demand [
12].
On the other hand, other studies found significant changes in oblique and vertical astigmatism (Z(2,−2) and Z(2,2), respectively), Z(3,−1), Z(3,1), vertical and oblique trefoil (Z(3,−3) and Z(3,3), respectively), vertical-pentafoil (Z(5,−5)), Z(6,−4), vertical-secondary-coma (Z(5,−1)), Z(7,−5), Z(7,−3), Z(7,3), and Z(7,5) with accommodation. However, since they change in different directions, there is no clear trend [
7,
8,
9,
12].
It appears that some other Zernike terms do undergo changes with accommodation, but the direction of these changes is not the same in all subjects.
2.3. Z(4,0), Z(6,0) and Accommodative Lag
An interesting aspect is the relationship between spherical aberration and accommodative lag. A positive Z(4,0) causes a lead for far targets, while a negative Z(4,0) causes a lag for near targets [
6]. On the other hand, Z(6,0) tends to increase the accommodative response regardless of whether it is positive or negative. The effect of Z(4,0) is greater than the effect of Z(6,0) [
20].
A previous study [
24] examined the effect of changing Z(4,0) on the accommodative response using contact lenses with controlled amounts of Z(4,0). When positive Z(4,0) was added, the slope of the accommodative stimulus–response function decreased, increasing the accommodative lag, whereas when negative Z(4,0) was added, the slope of the accommodative stimulus–response function increased, decreasing the accommodative lag. However, the same authors did not observe a relationship between RMS and accommodative lag.
According to some authors [
10,
20], Z(4,0) is responsible for the most accommodative leads and lags. When it is present, some amount of defocus (lead/lag) could be helpful in improving retinal image quality. Therefore, lead/lag during the accommodative response may be a method to reduce the effects caused by changes in Z(4,0) and Z(6,0) during accommodation. As mentioned earlier, since Z(4,0) is responsible for most of the accommodative leads and lags, a different tendency of Z(4,0) during accommodation due to the shape of the lens could result in excess or insufficiency of accommodation. This may explain why, under the same conditions (e.g., visual ergonomics and hours of near viewing), some subjects develop accommodative dysfunction and others do not.
2.4. Total, Corneal, and Internal HOAs during Accommodation
As previously noted, the shape and position of the crystalline lens change during ocular accommodation. The changes in ocular aberrations observed during accommodation are a result of these changes in the crystalline lens. Corneal wavefront aberrations do not change during accommodation [
7].
Shi et al. [
25] combined ultra-long-scan-depth spectral-domain optical coherence tomography (UL-SDOCT) and a Shack–Hartmann wavefront sensor to simultaneously analyze wavefront aberrations and anterior segment parameters, such as lens thickness and anterior and posterior lens curvature radii, during accommodation. Changes in lens dimensions occurred with changes in wavefront aberrations. It is the anterior surface of the lens that is most responsible for the variations in ocular aberrations during accommodation [
11]. According to Norberto López-Gil and Vicente Fernández-Sánchez [
20], 86% of the changes in wavefront aberrations with accommodation are due to the alterations in the anterior surface of the lens and 14% in its posterior surface.
Another study [
12] suggested that the changes in central Z(4,0) with accommodation are caused by the flattening of the peripheral portion of the lens, and other aberrations around this region are also changed.
In the relaxed state, there is a balance between corneal and internal aberrations [
26]. One partially compensates for the aberrations of the other, and this decreases with accommodation [
27]. The loss of this compensation during accommodation, i.e., during near vision tasks [
27], could lead to symptoms. The impact of this loss on the development of near-related problems should be investigated. In addition, refractive surgery must preserve this compensation as much as possible to improve visual quality for both distance and near vision.