Iridoschisis is a rare condition defined as a separation of the anterior iris stroma from the posterior stroma and muscle layers. A variety of ocular pathologies can coexist with iridoschisis, but in most cases the causal relationship, if any, is unclear. Glaucoma, primarily angle-closure glaucoma, is the most often described condition concomitant to iridoschisis. Other ocular abnormalities found relatively often in iridoschisis patients include cataract, lens subluxation and corneal abnormalities. Iridoschisis is plausibly a multifactorial disease. A patient diagnosed with iridoschisis should be screened for potential glaucoma, corneal and lens abnormalities. Iridoschisis may pose a challenge for both an ophthalmologist in an outpatient setting and an ophthalmic surgeon.
- iridoschisis
- iris degeneration
- free-floating iris tissue
- rare ocular disease
- angle-closure glaucoma
1. Introduction
Iridoschisis is a rare condition defined as a separation of the anterior iris stroma from the posterior stroma and muscle layers. In iridoschisis patients, the iris strands float in the aqueous humor and create a “shredded wheat” appearance [1]. The term iridoschisis (iris splitting) was first introduced in 1945 by Lowenstein and Foster, who reported a deep, parallel split between the anterior and posterior stromal layers of the iris [2]. However, the condition was first described as early as in 1922 by Schmitt who reported on the detachment of the anterior iris layer [3]
2. Epidemiology, Inheritance and Pathophysiology
Only about 150 cases of iridoschisis have been reported to date, with a slight predominance of female patients over males [4]. Some authors speculated that iridoschisis might be inherited in an autosomal dominant manner, but these reports are scarce [4][5]. However, some researchers suggested that iridoschisis is not inherited but occurs sporadically, secondary to trauma, glaucoma or syphilis [2][6][7][8][9]. Other authors considered iridoschisis age-related atrophy, given that the condition is found predominantly in persons between 60 and 70 years of age [10] However, it needs to be stressed that iridoschisis has also been reported in youths [11][12]. A number of theories exist regarding the pathogenesis of iridoschisis, but the exact underlying mechanism of this condition is yet to be explained. For example senile changes, trauma and ischemia were suspected as predisposing factors [2][6][13][14][15][16]
3. Clinical Characteristics and Diagnostic Imaging
While iridoschisis may be unilateral at its early stages, it occurs bilaterally in most cases [11] and may have a progressive character [17]. The condition is most often found in the inferior irideal quadrants, but also other parts of the iris may be affected, and sometimes the pathological process is spread across the whole iris [1][4][18][19]. The anterior iris stroma splits from the posterior stroma and muscle layers, and the loose ends wave in the aqueous humor of the anterior chamber, giving the iris a “shredded” appearance (Figure 1).
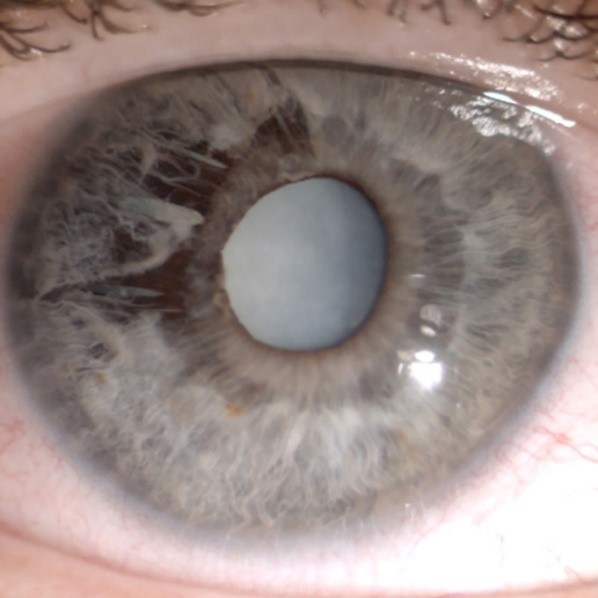
Figure 1. “Shredded” appearance of the iris: superotemporal iridoschisis and mature cataract. Adapted from “Iris-claw lens implantation in a patient with iridoschisis” by Pieklarz B, Grochowski E, Dmuchowska DA, Saeed E, Sidorczuk P, Mariak Z. Am J Case Rep, 2020; 21: e925234.
The posterior layer of the iris usually remains intact with the retained function of the sphincter and dilator fibers [13] Visual deterioration may be caused by glaucoma, cataract or corneal decompensation secondary to iridocorneal touch [20]Anterior segment optical coherence tomography (AS-OCT), ultrasound biomicroscopy (UBM) and Scheimpflug imaging are complementary diagnostic options in patients with suspected iridoschisis (Figure 2) [10][21][22]
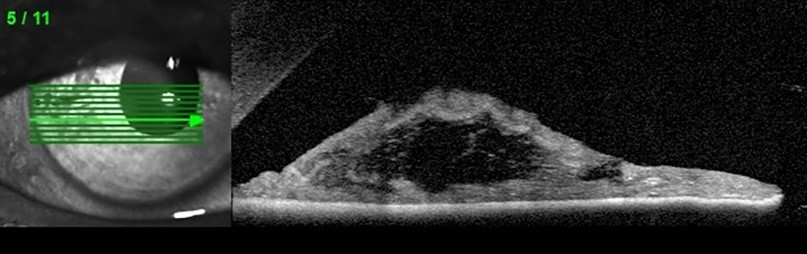
Figure 2. Anterior segment optical coherence tomography (AS-OCT): disorganization of the iris stroma corresponding to iridoschisis.
4. Associated Ocular Pathologies
Iridoschisis may coexist with an array of other ocular pathologies as reviewed by Pieklarz et al. [23], and in most of the cases, it is unclear whether it occurs as a cause or effect or just by coincidence. Glaucoma, primarily angle-closure glaucoma, is found in more than two-thirds of patients with iridoschisis [1]. A coexistence of iridoschisis with chronic open-angle glaucoma or angle recession glaucoma has been reported as well [9][19][24]. Some published evidence suggests that iridoschisis may coexist with presenile cataract and mature cataract [1][12][25][26][27]. While rarely, iridoschisis may also be found concomitantly to lens subluxation [7][19][25][28][29][30]. Corneal changes are uncommon and, if present, the degenerated corneal endothelial cells are mostly localized above the area of iridoschisis [31][32][33][34][35]. Total endothelial decompensation has been reported as well [36]. A rare combination of iridoschisis with keratoconus has been also reported [37][38].
5. Summary
The prevalence of iridoschisis is difficult to estimate. It is probably underreported as no dedicated registry for this condition exists. Iridoschisis is plausibly a multifactorial disease that requires particular attention from ophthalmologists and ophthalmic surgeons. A patient diagnosed with iridoschisis should also be screened for potential glaucoma, corneal and lens abnormalities. If not yet present, one of these conditions may subsequently develop, and hence iridoschisis patients should be followed-up on a regular basis.
This entry is adapted from the peer-reviewed paper 10.3390/jcm9103324
References
- Eleni Gogaki; Fani Tsolaki; Sotiria Tiganita; Christina Skatharoudi; Demetrios Balatsoukas; Iridoschisis: case report and review of the literature. Clinical Ophthalmology (Auckland, N.Z.) 2011, 5, 381-384, 10.2147/OPTH.S17269.
- Arnold Loewenstein; John Foster; IRIDOSCHISIS WITH MULTIPLE RUPTURE OF STROMAL THREADS. British Journal of Ophthalmology 1945, 29, 277-282, 10.1136/bjo.29.6.277.
- Shmitt A; Detachment of the anterior half of the iris plane. Klin Monatsbl Angenheilkd 1922, 68, 214-215, .
- Ahmad M. Mansour; A family with iridoschisis, narrow anterior chamber angle, and presenile cataract. Ophthalmic Paediatrics and Genetics 1986, 7, 145-149, 10.3109/13816818609004131.
- J Danias; I M Aslanides; J W Eichenbaum; R H Silverman; D Z Reinstein; D J Coleman; Iridoschisis: high frequency ultrasound imaging. Evidence for a genetic defect?. British Journal of Ophthalmology 1996, 80, 1063-1067, 10.1136/bjo.80.12.1063.
- Arnold Loewenstein; John Foster; S. K. Sledge; A FURTHER CASE OF IRIDOSCHISIS. British Journal of Ophthalmology 1948, 32, 129-134, 10.1136/bjo.32.3.129.
- A. Romano; G. Treister; R. Barishak; R. Stein; Iridoschisis and Angle-Closure Glaucoma. Ophthalmologica 1972, 164, 199-207, 10.1159/000306752.
- Pérez-Carro, G, Vilanova, M Antuña, M.G. Cárcaba, V Junceda-Moreno; Iridoschisis associated to congenital syphilis: Serological confirmation at the 80’s. Arch. Soc. Esp. Oftalmol 2009, 84, 353–358, .
- A J Foss; P G Hykin; L Benjamin; Interstitial keratitis and iridoschisis in congenital syphilis.. Journal of clinical neuro-ophthalmology 1992, 12, 167-170, .
- Yiyi Chen; Yiyong Qian; Peirong Lu; Iridoschisis: a case report and literature review. BMC Ophthalmology 2017, 17, 1-6, 10.1186/s12886-017-0418-2.
- Paul Gregory Schoneveld; Konrad Pesudovs; Iridoschisis. Clinical and Experimental Optometry 1999, 82, 29-33, 10.1111/j.1444-0938.1999.tb06784.x.
- Thomas M. Aaberg; Matthew Patrick Nelson; Thomas M. Aaberg Jr.; Iridoschisis and cataract in a juvenile patient with periocular eczema. JCRS Online Case Reports 2017, 5, 54-57, 10.1016/j.jcro.2017.06.001.
- E C Albers; B A Klien; Iridoschisis; a clinical and histopathologic study.. American Journal of Ophthalmology 1958, 46, 794-802, .
- Carnevalini A, Menchini U, Bandello F, Scialdone A, Brancarto R; Aspects fluoroiridographiques de L ‘Iridoschisis. J. Fr. Ophthalmol 1988, 11, 329–332, .
- Jørgen Bøjer; IRIDOSCHISIS - ESSENTIAL IRIS ATROPHY. Acta Ophthalmologica 2009, 31, 253-264, 10.1111/j.1755-3768.1953.tb03292.x.
- T D Payne; R P Thomas; Iridoschisis. A case report.. American Journal of Ophthalmology 1966, 62, 966–967, .
- É. Agard; A. Malclès; Hussam El Chehab; G. Ract-Madoux; B. Swalduz; F. Aptel; Philippe Denis; C. Dot; L’iridoschisis, une forme particulière d’atrophie irienne. Journal Français d'Ophtalmologie 2013, 36, 368-371, 10.1016/j.jfo.2012.10.004.
- Eun Ji Lee; Jin Hak Lee; Joon Young Hyon; Mee Kum Kim; Won Ryang Wee; A Case of Cataract Surgery without Pupillary Device in the Eye with Iridoschisis. Korean Journal of Ophthalmology 2008, 22, 58-62, 10.3341/kjo.2008.22.1.58.
- J F Salmon; A D N Murray; The association of iridoschisis and primary angle-closure glaucoma. Eye 1992, 6, 267-272, 10.1038/eye.1992.50.
- André A. M. Torricelli; Alexandre Soares Castro Reis; Julio Zaki Abucham; Ricardo Suzuki; Roberto Freire Santiago Malta; Mário Luiz R. Monteiro; Bilateral nonarteritic anterior ischemic neuropathy following acute angle-closure glaucoma in a patient with iridoschisis: case report.. Arquivos Brasileiros de Oftalmologia 2011, 74, 61-63, 10.1590/S0004-27492011000100015.
- Laura Paniagua; Manuel Bande; Maria Teresa Rodríguez-Ares; Antonio Piñeiro; A presentation of iridoschisis with plateau iris: an imaging study. Clinical and Experimental Optometry 2015, 98, 290-291, 10.1111/cxo.12250.
- Chiharu Shima; Yasumasa Otori; Atsuya Miki; Yasuo Tano; A Case of Iridoschisis Associated with Plateau Iris Configuration. Japanese Journal of Ophthalmology 2007, 51, 390-391, 10.1007/s10384-007-0454-1.
- Barbara Pieklarz; Emil Tomasz Grochowski; Emil Saeed; Patryk Sidorczuk; Zofia Mariak; Diana Anna Dmuchowska; Iridoschisis—A Systematic Review. Journal of Clinical Medicine 2020, 9, 3324, 10.3390/jcm9103324.
- John F. Salmon; F.C. Ophth.; The Association of Iridoschisis and Angle-recession Glaucoma. American Journal of Ophthalmology 1992, 114, 766-767, 10.1016/s0002-9394(14)74059-0.
- Barbara Pieklarz; Emil T. Grochowski; Diana A. Dmuchowska; Emil Saeed; Patryk Sidorczuk; Zofia Mariak; Iris-Claw Lens Implantation in a Patient with Iridoschisis. American Journal of Case Reports 2020, 21, e925234-1-e925234-5, 10.12659/ajcr.925234.
- D L Krohn; E E Garrett; Iridoschisis and keratoconus; report of case in a twenty-year-old man.. A.M.A. Archives of Ophthalmology 1954, 52, 426–432, .
- Alastair Porteous; Sancy Low; Saad Younis; Philip Bloom; Lens extraction and intraocular lens implant to manage iridoschisis. Clinical & Experimental Ophthalmology 2014, 43, 82-83, 10.1111/ceo.12361.
- Shishir Agrawal; Jaya Agrawal; Trilok P. Agrawal; Iridoschisis associated with lens subluxation. Journal of Cataract and Refractive Surgery 2001, 27, 2044-2046, 10.1016/s0886-3350(00)00862-2.
- Richard A Adler; Robert S Weinberg; Iridoschisis and bilateral lens subluxation associated with periocular eczema. Journal of Cataract and Refractive Surgery 2004, 30, 234-236, 10.1016/s0886-3350(03)00517-0.
- Tetsuya Tetsuya Mutoh; A case of iridoschisis associated with lens displacement into the vitreous cavity. Clinical Ophthalmology 2010, 4, 487, 10.2147/OPTH.S9885.
- Merlyn C. Rodrigues; George L. Spaeth; Jay H. Krachmer; Peter R. Laibson; Iridoschisis Associated with Glaucoma and Bullous Keratopathy. American Journal of Ophthalmology 1983, 95, 73-81, 10.1016/0002-9394(83)90335-5.
- Hong-Bin Wang; Yong-Xia Hu; Xue Feng; Corneal endothelial decompensation secondary to iridoschisis in degenerative myopic eyes: a case report. International Journal of Ophthalmology 2012, 5, 116-118, 10.3980/j.issn.2222-3959.2012.01.24.
- Shigeto Kumakura; Teruumi Minezaki; Takaaki Hattori; Hayate Nakagawa; Hiroshi Goto; Non-Descemet’s stripping automated endothelial keratoplasty for bullous keratopathy secondary to iridoschisis. Clinical Ophthalmology 2013, 7, 1353-1355, 10.2147/OPTH.S43180.
- N J Crosby; Peter McDonnell; Peter Shah; Iridoschisis associated with nanophthalmos and bullous keratopathy. International Ophthalmology 2012, 33, 83-85, 10.1007/s10792-012-9627-0.
- Miles F. Greenwald; Philip I. Niles; A. Tim Johnson; Jesse M. Vislisel; Mark A. Greiner; Descemet membrane endothelial keratoplasty for corneal decompensation due to iridoschisis.. American Journal of Ophthalmology Case Reports 2018, 9, 34-37, 10.1016/j.ajoc.2018.01.010.
- Sathish Srinivasan; Mark Batterbury; Paul Hiscott; Bullous keratopathy and corneal decompensation secondary to iridoschisis: a clinicopathological report.. Cornea 2005, 24, 867-9, .
- Richard A. Eiferman; Mark Law; Leon Lane; Iridoschisis and Keratoconus. Cornea 1994, 13, 78-79, 10.1097/00003226-199401000-00013.
- Aleksandra Petrovic; Georgios Kymionis; Massive iridoschisis after penetrating keratoplasty successfully managed with nd:Yag punctures: A case report. European Journal of Ophthalmology 2019, 30, NP15-NP17, 10.1177/1120672119853105.