The interaction of electromagnetic fields (EMF) with living tissues or manufactured objects can produce different effects on these exposed entities. In different circumstances, these fields are used daily in various friendly applications. Applications of non-ionizing RF-EMF, frequencies from 100 kHz to 300 GHz have continuously increased. This involves medicine (e.g., magnetic resonance imaging and RF ablation), manufacturing (e.g., heaters and solders), home usages (e.g., child video display unit and Wi-Fi), protection and navigation (e.g., radar and RFID) and particularly in telecommunications (e.g., TV transmitting and mobile phones). This growth signifies that great amounts of the population are undergoing exposure to RF(radiofrequency)-EMF and worry has been inflated concerning public health concerns due to such exposure.
- electromagnetic fields
- radiofrequency exposure
- biological effects
- atypical symptom
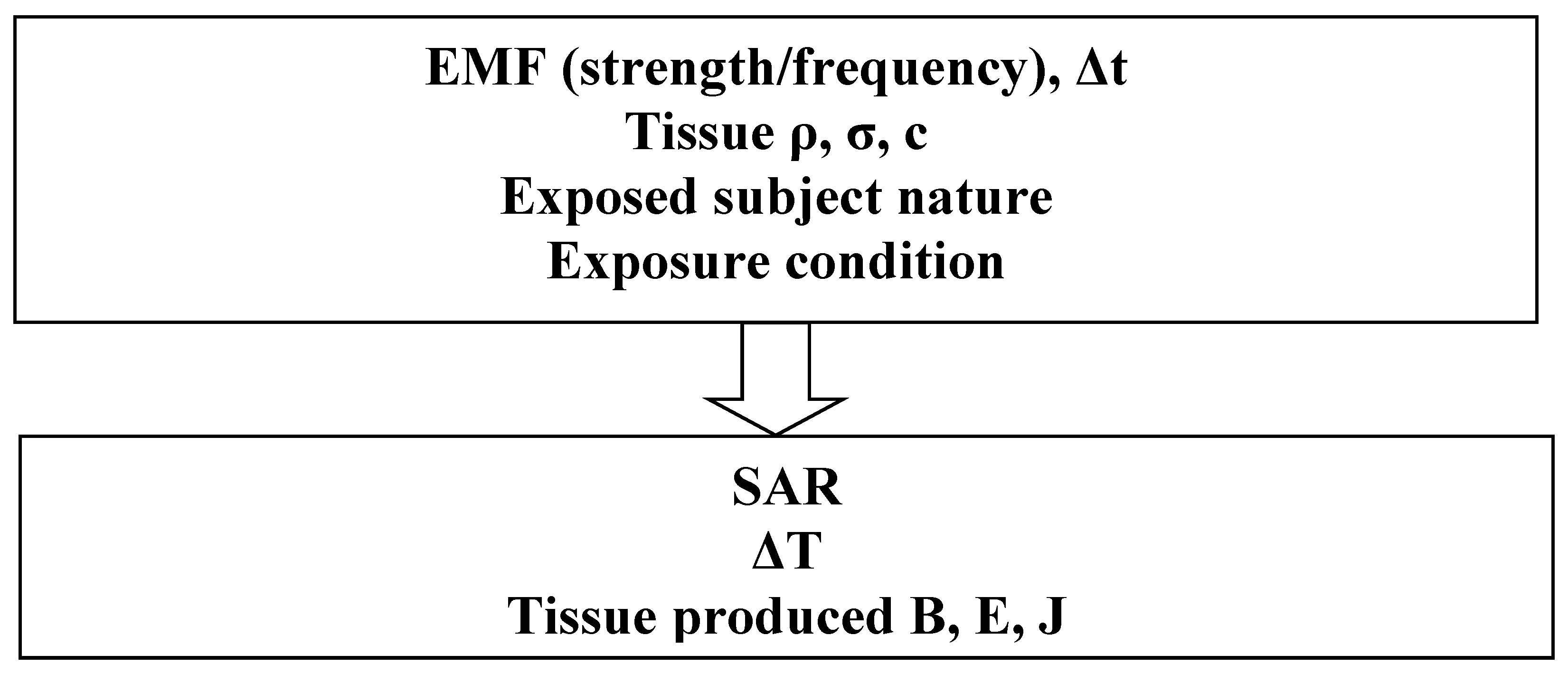
1. Characteristics of Sources and Interactions
2. Thermal BE Due to RF-EMF
3. Health Safety Standards
4. AS Due to RF-EMF
5. Evaluation of RF-EMF BE and AS
6. Governing Mathematical Equations
This entry is adapted from the peer-reviewed paper 10.3390/app13031265
References
- Razek, A. Biological and Medical Disturbances Due to Exposure to Fields Emitted by Electromagnetic Energy Devices—A Review. Energies 2022, 15, 4455.
- Eriksson, N.; Höög, J.; Mild, K.H.; Sandström, M.; Stenberg, B. The psychosocial work environment and skin symptoms among visual display terminal workers: A case referent study. Int. J. Epidemiol. 1997, 26, 1250–1257.
- Lidén, S. “Sensitivity to electricity” a new environmental epidemic. Allergy 1996, 51, 519–524.
- Bergqvist, U.; Vogel, E. Possible Health Implications of Subjective Symptoms and Electromagnetic Fields; A Report Prepared by a European Group of Experts for the European Commission, DG V; National Institute for Working Life: Stockholm, Sweden, 1997; p. 135. Available online: https://gupea.ub.gu.se/bitstream/handle/2077/4156/ah1997_19.pdf?sequence=1 (accessed on 10 January 2023).
- Lindén, V.; Rolfsen, S. Video computer terminals and occupational dermatitis. Scand. J. Work Environ. Health 1981, 7, 62–64.
- Carpenter, D.O. The microwave syndrome or electro-hypersensitivity: Historical background. Rev. Environ. Health 2015, 30, 217–222.
- Lin, J.C. Early contributions to electromagnetic fields in living systems. In Advances in Electromagnetic Fields and Living Systems; Lin, J.C., Ed.; Plenum Press: New York, NY, USA, 1994; pp. 1–26.
- Bren, S. Historical introduction to EMF health effects. IEEE Eng. Med. Biol. 1996, 15, 24–30.
- Dieudonné, M. Controverses autour des champs électromagnétiques et de l’électrohypersensibilité. La construction de problèmes publics “à bas bruit”. St. Publique 2019, 31, 43.
- Schreier, N.; Huss, A.; Röösli, M. The prevalence of symptoms attributed to electromagnetic field exposure: A cross-sectional representative survey in Switzerland. Soz. Praventiv. Med. 2006, 51, 202–209.
- Schröttner, J.; Leitgeb, N. Sensitivity to electricity–temporal changes in Austria. BMC Public Health 2008, 8, 310.
- Blettner, M.; Schlehofer, B.; Breckenkamp, J.; Kowall, B.; Schmiedel, S.; Reis, U.; Potthoff, P.; Schuz, J.; Berg-Beckhoff, G. Mobile phone base stations and adverse health effects: Phase 1 of a population-based, cross-sectional study in Germany. Occup. Environ. Med. 2009, 66, 118–123.
- Karvala, K.; Sainio, M.; Palmquist, E.; Nyback, M.-H.; Nordin, S. Prevalence of various environmental intolerances in a Swedish and Finnish general population. Environ. Res. 2018, 161, 220–228.
- International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to time-varying electric and magnetic fields for low frequencies (1 Hz–100 kHz). Health Phys. 2010, 99, 818–836.
- International Commission on Non-Ionizing Radiation Protection. Guidelines for limiting exposure to electromagnetic fields (100 kHz to 300 GHz). Health Phys. 2020, 118, 483–524.
- IEEE Standard C95.1; IEEE Standard for Safety Levels with Respect to Human Exposure to Electric, Magnetic, and Electromagnetic Fields, 0 Hz to 300 GHz. IEEE: Piscataway, NJ, USA, 2019.
- Sunstein, C.R. Beyond the precautionary principle. Univ. Pa Law Rev. 2003, 151, 1003–1058.
- Schmiedchen, K.; Driessen, S.; Oftedal, G. Methodological limitations in experimental studies on symptom development in individuals with idiopathic environmental intolerance attributed to electromagnetic fields (IEI-EMF)—A systematic review. Environ. Health 2019, 18, 88.
- Ishihara, T.; Yamazaki, K.; Araki, A.; Teraoka, Y.; Tamura, N.; Hikage, T.; Omiya, M.; Mizuta, M.; Kishi, R. Exposure to Radiofrequency Electromagnetic Field in the High-Frequency Band and Cognitive Function in Children and Adolescents: A Literature Review. Int. J. Environ. Res. Public Health 2020, 17, 9179.
- Dieudonné, M. Electromagnetic hypersensitivity: A critical review of explanatory hypotheses. Environ. Health 2020, 19, 48.
- Cirimele, V.; Freschi, F.; Giaccone, L.; Pichon, L.; Repetto, M. Human Exposure Assessment in Dynamic Inductive Power Transfer for Automotive Applications. IEEE Trans. Magn. 2017, 53, 5000304.
- Hariri, H.; Bernard, Y.; Razek, A. Dual piezoelectric beam robot: The effect of piezoelectric patches positions. J. Intell. Mater. Syst. Struct. 2015, 26, 2577–2590.
- Nunes, A.; Daniel, L.; Hage Hassan, M.; Domenjoud, M. Modeling of the magnetic behavior of permanent magnets including ageing effects. J. Magn. Magn. Mater. 2020, 512, 166930.
- Ren, Z.; Razek, A. New technique for solving three-dimensional multiply connected eddy-current problems. IEE Proc. 693 A Phys. Sci. Meas. Instr. 1990, 137, 135–140.
- Ren, Z.; Razek, A. Boundary edge elements and spanning tree technique in three-dimensional electromagnetic field computation. Int. J. Numer. Methods Eng. 1993, 36, 2877–2893.
- Jiao, D.; Jin, J.-M. An effective algorithm for implementing perfectly matched layers in time-domain finite-element simulation of open-region EM problems. IEEE Trans. Antennas Propag. 2002, 50, 1615–1623.
- Carpes, W.P.; Pichon, L.; Razek, A. A 3D finite element method for the modelling of bounded and unbounded electromagnetic problems in the time domain. Int. J. Numer. Model. Electron. Netw. Devices Fields 2000, 13, 527–540.
- Sun, Q.; Zhang, R.; Zhan, Q.; Liu, Q.H. 3-D Implicit–Explicit Hybrid Finite Difference/Spectral Element/Finite Element Time Domain Method without a Buffer Zone. IEEE Trans. Antennas Propag. 2019, 67, 5469–5476.
- Ding, P.; Bernard, L.; Pichon, L.; Razek, A. Evaluation of Electromagnetic Fields in Human Body Exposed to Wireless Inductive Charging System. IEEE Trans. Magn. 2014, 50, 1037–1040.
- Pennes, H.H. Analysis of tissue and arterial blood temperatures in the resting human forearm. J. Appl. Physiol. 1998, 85, 5–34.