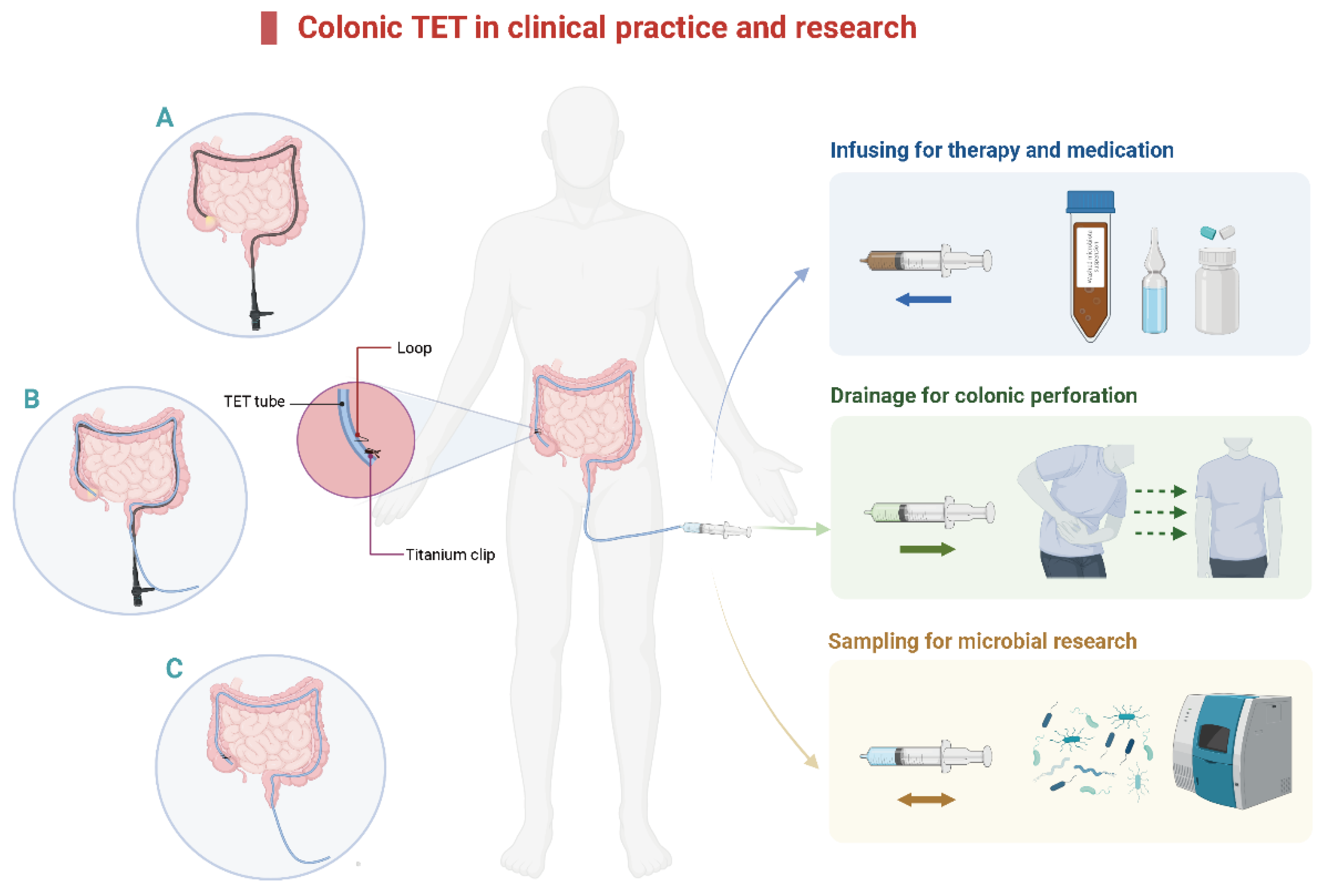
The limitation of traditional delivery methods for fecal microbiota transplantation (FMT) gave birth to colonic transendoscopic enteral tubing (TET) to address the requirement of frequent FMTs. Colonic TET as a novel endoscopic intervention has received increasing attention in practice since 2015 in China. Emerging studies from multiple centers indicate that colonic TET is a promising, safe, and practical delivery method for microbial therapy and administering medication with high patient satisfaction.
- fecal microbiota transplantation
- transendoscopic enteral tube
- drainag
1. Introduction
2. The Concept and Technique of Colonic TET
3. The Applications of Colonic TET
3.1 Colonic TET for Microbial Therapy
| Delivery Ways | Advantages | Limitations |
|---|---|---|
| Oral capsules | Overcome the concern of invasive administration; easy to perform | Efficacy may affect by gastric acid and the preservation state of bacteria |
| Gastroscopy | Easy to reach the target location | Not convenient to repeat FMTs |
| Mid-gut/Nasojejunal tube/PEGJ tube | Easy to reach the target location; convenient to repeat FMTs; easy to maintain | Placed under gastroscopy; limited and special population for use |
| Colonoscopy | Easy to reach the target location | Not convenient to repeat FMTs |
| Colonic TET tube | Easy to reach the target location; convenient to repeat FMTs; easy to maintain; | Placed under colonoscopy |
| Stoma in ilecolon/colon | Convenient to repeat FMTs; easy to perform | Only for selected population with surgical double-cavity stoma in ilecolon/colon |
| Enema | Easy to perform; low cost | Difficulty to hold the bacteria suspension in rectum for a long time |
| Author, Year | Article Type | Case, n | Sex, Male, n (%); Age, Mean (Range), Years |
Indication | Clinical Success Rate | Satisfaction Rate | The Mean Retention Time | Adverse Events | The Target Location | The Endoscopic Clips | The Average of Endoscopic Clips |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zhang et al., 2022 [32] | Prospective study | 27 | 17(63.0%); 47.48 ± 12.34 | UC | 100% | NA | NA | NA | NA | NA | NA |
| Chen et al., 2021 [42] | Retrospective study | 16 | 10 (62.5%); 39.88 ± 11 | UC | 100% | 97.3% | NA | 3 | NA | NA | NA |
| Zhong et al., 2021 [20] | Prospective study | 47 | 42 (89.36%); 5(4–6) | 21 autism, 6 UC, 2 rCDI, 1 CD, 17 others | 100% | 100% | 6 (5–7) | 4 | 29 in ileocecal, 12 in the transverse colon, 6 in left colon ileum | 35 in large, 12 in small | 2 (1.75–3) |
| Long et al., 2020 [43] | Prospective study | 257 | 138 (57%); 39.9 ± 18.4 | 132 UC, 14 CD, 10 epilepsy, 8 autism, 56 others | 100% | NA | 9.3 ± 3.8 (2–28) | 21 | 215 in ileocecal, 6 in the transverse colon, 25 in the left colon, 6 in descending colon | 154 in large, 103 in small | 3.5 ± 1.0 (2–6) (in 95 cases) |
| Luo et al., 2020 [44] | Retrospective study | 9 | 6 (66.7%); 47.44 ± 12.26 | UC | 100% | NA | NA | 1 | NA | NA | NA |
| Wen et al., 2020 [21] | Randomized controlled trial | 303 | 155 (51.16%); 44.4 ± 17.6 | 93 constipation, 88 UC, 32 IBS, 9 CD, 2 health, 75 others | 100% | 100% | 8 (6–10) | 9 | NA | NA | 2.65 ± 1.1 |
| Liu et al., 2021 [18] | Prospective study | 5 | NA | Health | 100% | NA | NA | NA | 5 in ileocecal | NA | NA |
| Chen et al., 2020 [33] | Prospective study | 44 | 25 (57%); 44.4 ± 17.6 | UC | 100% | NA | NA | 5 | NA | NA | NA |
| Chen et al., 2020 [36] | Prospective study | 5 | 5 (100%); 47.9 ± 10.6 | UC | 100% | NA | NA | 0 | NA | NA | NA |
| Zhang et al., 2019 [45] | Randomized controlled trial | 21 | NA; 49.2 ± 13.77 | UC | 100% | 100% | NA | 3 | 21 in ileocecal | NA | NA |
| Wang et al., 2019 [41] | Case series | 5 | 4 (80%); 56.33 (31–94) | 4 rCDI, 1 CD | 100% | NA | NA | NA | 5 in left colon | NA | NA |
| Zhang et al., 2021 [17] | Case | 3 | 1 (50%); 38 (25–51) | 2UC, 1 CD | 100% | NA | NA | NA | 1 in left colon, 2 in descending colon | NA | NA |
| Luo et al., 2021 [44] | Case | 1 | 1 (100%); 32 | UC | 100% | NA | NA | NA | NA | NA | NA |
| Zhao et al., 2021 [38] | Case | 2 | 0 (0%); 40 (32–48) | Refractory IgA nephropathy | 100% | NA | NA | 2 | NA | NA | NA |
| Wang et al., 2020 [41] | Case | 1 | 1 (100%); 77 | rCDI | 100% | NA | NA | NA | NA | NA | NA |
| Zhong et al., 2019 [20] | Case | 1 | 1 (100%); 31 | CD | 100% | NA | NA | NA | NA | NA | NA |
| Zhang et al., 2019 [45] | Case | 1 | 1 (100%); 55 | UC | 100% | NA | NA | NA | NA | NA | NA |
3.2. Colonic TET for Drainage and Decompression from Deep Colon
3.3 Colonic TET for Traditional Microbiota Research
Microorganisms play critical roles in various physiological functions of the host. Exploring the human microbiota-host interaction could reflect the connection between health and disease [58][59]. Principally, all gut microbiota-derived metabolites are produced in one of three ways: directly from ingested compounds, from host-derived substrates, or de novo from primary metabolites [59]. Therefore, finding a more effective method to sample metabolites is vital. In most studies, fecal samples were used to study the gut microbiome. Although they can be acquired easily, continual fecal samples are rarely taken within short intervals [60]. Some studies found that the ileocecal microbiome, localized in the middle part of the gastrointestinal tract, had relatively higher diversity than the fecal microbiome [61]. Moreover, studies on sampling the intestinal lavage fluid (IVF) microbiome found that pathogenic microbiota was more abundant in the IVF than in feces, and the microbiome in the IVF may be a better indicator for evaluating the risk of developing colorectal cancer compared with fecal samples [62].
Microbial circadian rhythmicity is a feature of mammalian metabolism that might be a significant factor in the development of metabolic disease [63]. Lora V’s group found that the intestinal microbiota in the mouse small intestine programs diurnal metabolic rhythms through histone deacetylase 3 [64]. To investigate community dynamics in the intestine with better resolution, Wang et al. applied colonic TET to extract cecum fluid samples from healthy volunteers twice daily (10 a.m. and 10 p.m.) via syringe, from which metagenomic, metatranscriptomic, metabolomic, and virome analyses were conducted [65][66]. The results revealed the individuality of reconstruction in microbiome composition, functions, and shared characteristics of the internal resilience of the gut microbiome. Sampling the ileocecal microbiota in situ provides unique insights into the diurnal patterns or circadian rhythms of the human gut microbiome for the first time. Based on samples from a healthy human cecum, Liu et al. further identified that gut microbial methionine impacts circadian clock gene expression and reactive oxygen species level in the host gastrointestinal tract [18]. Moreover, Fawad et al. reported that gut microbe-generated short-chain fatty acids entrained intestinal epithelial circadian rhythms by inhibiting histone deacetylase [67]. Collection of intestinal fluid with a sterile syringe is recommended. Colonic TET is currently the best non-invasive tool for collecting microbial samples from the deep colon in humans.
4. Conclusions
This entry is adapted from the peer-reviewed paper 10.3390/jcm12030780
References
- Surawicz, C.M.; Brandt, L.J.; Binion, D.G.; Ananthakrishnan, A.N.; Curry, S.R.; Gilligan, P.H.; McFarland, L.V.; Mellow, M.; Zuckerbraun, B.S. Guidelines for diagnosis, treatment, and prevention of Clostridium difficile infections. Am. J. Gastroenterol. 2013, 108, 478–498; quiz 499.
- Xiang, L.; Ding, X.; Li, Q.; Wu, X.; Dai, M.; Long, C.; He, Z.; Cui, B.; Zhang, F. Efficacy of faecal microbiota transplantation in Crohn’s disease: A new target treatment? Microb. Biotechnol. 2020, 13, 760–769.
- Ding, X.; Li, Q.; Li, P.; Zhang, T.; Cui, B.; Ji, G.; Lu, X.; Zhang, F. Long-Term Safety and Efficacy of Fecal Microbiota Transplant in Active Ulcerative Colitis. Drug Saf. 2019, 42, 869–880.
- Huang, H.; Chen, H.; Luo, Q.; Xu, H.; He, J.; Li, Y.; Zhou, Y.; Yao, F.; Nie, Y.; Zhou, Y. Relief of irritable bowel syndrome by fecal microbiota transplantation is associated with changes in diversity and composition of the gut microbiota. J. Dig. Dis. 2019, 20, 401–408.
- Pan, Z.; Zhong, H.; Huang, D.; Wu, L.; He, X. Beneficial Effects of Repeated Washed Microbiota Transplantation in Children with Autism. Front. Pediatr. 2022, 10, 928785.
- Meijnikman, A.S.; Gerdes, V.E.; Nieuwdorp, M.; Herrema, H. Evaluating Causality of Gut Microbiota in Obesity and Diabetes in Humans. Endocr. Rev. 2018, 39, 133–153.
- Dai, M.; Liu, Y.; Chen, W.; Buch, H.; Shan, Y.; Chang, L.; Bai, Y.; Shen, C.; Zhang, X.; Huo, Y.; et al. Rescue fecal microbiota transplantation for antibiotic-associated diarrhea in critically ill patients. Crit. Care 2019, 23, 324.
- Ding, X.; Li, Q.; Li, P.; Chen, X.; Xiang, L.; Bi, L.; Zhu, J.; Huang, X.; Cui, B.; Zhang, F. Fecal microbiota transplantation: A promising treatment for radiation enteritis? Radiother. Oncol. 2020, 143, 12–18.
- Zheng, Y.; Chen, X.; Cai, J.; Yuan, Y.; Xie, W.; Xu, J.; Xia, H.H.; Zhang, M.; He, X.; Wu, L. Washed microbiota transplantation reduces proton pump inhibitor dependency in nonerosive reflux disease. World J. Gastroenterol. 2021, 27, 513–522.
- Gulati, M.; Singh, S.K.; Corrie, L.; Kaur, I.P.; Chandwani, L. Delivery routes for faecal microbiota transplants: Available, anticipated and aspired. Pharmacol. Res. 2020, 159, 104954.
- Zhang, F.; Cui, B.; He, X.; Nie, Y.; Wu, K.; Fan, D.; FMT-Standardization Study Group. Microbiota transplantation: Concept, methodology and strategy for its modernization. Protein Cell 2018, 9, 462–473.
- Peng, Z.; Xiang, J.; He, Z.; Zhang, T.; Xu, L.; Cui, B.; Li, P.; Huang, G.; Ji, G.; Nie, Y.; et al. Colonic transendoscopic enteral tubing: A novel way of transplanting fecal microbiota. Endosc. Int. Open 2016, 4, E610–E613.
- Youngster, I.; Russell, G.H.; Pindar, C.; Ziv-Baran, T.; Sauk, J.; Hohmann, E.L. Oral, capsulized, frozen fecal microbiota transplantation for relapsing Clostridium difficile infection. JAMA 2014, 312, 1772–1778.
- Long, C.; Yu, Y.; Cui, B.; Jagessar, S.A.R.; Zhang, J.; Ji, G.; Huang, G.; Zhang, F. A novel quick transendoscopic enteral tubing in mid-gut: Technique and training with video. BMC Gastroenterol. 2018, 18, 37.
- Marcella, C.; Cui, B.; Kelly, C.R.; Ianiro, G.; Cammarota, G.; Zhang, F. Systematic review: The global incidence of faecal microbiota transplantation-related adverse events from 2000 to 2020. Aliment. Pharmacol. Ther. 2020, 53, 33–42.
- Allegretti, J.R.; Mullish, B.H.; Kelly, C.; Fischer, M. The evolution of the use of faecal microbiota transplantation and emerging therapeutic indications. Lancet 2019, 394, 420–431.
- Zhang, F.; Wen, Q.; Cui, B. Drainage via colonic transendoscopic enteral tubing increases our confidence in rescuing endoscopy-associated perforation. Endoscopy 2021, 54, E201–E202.
- Liu, X.; Dai, M.; Ma, Y.; Zhao, N.; Wang, Z.; Yu, Y.; Xu, Y.; Zhang, H.; Xiang, L.; Tian, H.; et al. Reconstruction and Dynamics of the Human Intestinal Microbiome Observed In Situ. Engineering 2021, 15, 89–101.
- Zhang, T.; Long, C.; Cui, B.; Buch, H.; Wen, Q.; Li, Q.; Ding, X.; Ji, G.; Zhang, F. Colonic transendoscopic tube-delivered enteral therapy (with video): A prospective study. BMC Gastroenterol. 2020, 20, 135.
- Zhong, M.; Buch, H.; Wen, Q.; Long, C.; Cui, B.; Zhang, F. Colonic Transendoscopic Enteral Tubing: Route for a Novel, Safe, and Convenient Delivery of Washed Microbiota Transplantation in Children. Gastroenterol. Res. Pract. 2021, 2021, 6676962.
- Wen, Q.; Liu, K.-J.; Cui, B.-T.; Li, P.; Wu, X.; Zhong, M.; Wei, L.; Tu, H.; Yuan, Y.; Lin, D.; et al. Impact of cap-assisted colonoscopy during transendoscopic enteral tubing: A randomized controlled trial. World J. Gastroenterol. 2020, 26, 6098–6110.
- Oancea, I.; Movva, R.; Das, I.; de Cárcer, D.A.; Schreiber, V.; Yang, Y.; Purdon, A.; Harrington, B.; Proctor, M.; Wang, R.; et al. Colonic microbiota can promote rapid local improvement of murine colitis by thioguanine independently of T lymphocytes and host metabolism. Gut 2016, 66, 59–69.
- Zhang, T.; Lu, G.; Zhao, Z.; Liu, Y.; Shen, Q.; Li, P.; Chen, Y.; Yin, H.; Wang, H.; Marcella, C.; et al. Washed microbiota transplantation vs. manual fecal microbiota transplantation: Clinical findings, animal studies and in vitro screening. Protein Cell 2020, 11, 251–266.
- Lu, G.; Wang, W.; Li, P.; Wen, Q.; Cui, B.; Zhang, F. Washed preparation of faecal microbiota changes the transplantation related safety, quantitative method and delivery. Microb. Biotechnol. 2022, 15, 2439–2449.
- Fecal Microbiota Transplantation-Standardization Study Group. Nanjing consensus on methodology of washed microbiota transplantation. Chin. Med. J. 2020, 133, 2330–2332.
- Ianiro, G.; Mullish, B.H.; Kelly, C.R.; Kassam, Z.; Kuijper, E.J.; Ng, S.C.; Iqbal, T.H.; Allegretti, J.R.; Bibbo, S.; Sokol, H.; et al. Reorganisation of faecal microbiota transplant services during the COVID-19 pandemic. Gut 2020, 69, 1555–1563.
- Zhang, Y.; Xue, X.; Su, S.; Zhou, H.; Jin, Y.; Shi, Y.; Lin, J.; Wang, J.; Li, X.; Yang, G.; et al. Patients and physicians’ attitudes change on fecal microbiota transplantation for inflammatory bowel disease over the past 3 years. Ann. Transl. Med. 2021, 9, 1619.
- Zhong, M.; Sun, Y.; Wang, H.-G.; Marcella, C.; Cui, B.-T.; Miao, Y.-L.; Zhang, F.-M. Awareness and attitude of fecal microbiota transplantation through transendoscopic enteral tubing among inflammatory bowel disease patients. World J. Clin. Cases 2020, 8, 3786–3796.
- Dai, M.; Zhang, T.; Li, Q.; Cui, B.; Xiang, L.; Ding, X.; Rong, R.; Bai, J.; Zhu, J.; Zhang, F. The bowel preparation for magnetic resonance enterography in patients with Crohn’s disease: Study protocol for a randomized controlled trial. Trials 2019, 20, 1.
- Philip, S.; Tageldin, O.; Mansoor, M.S.; Richter, S. Successful Fecal Microbiota Transplant Delivered by Foley Catheter Through a Loop Ileostomy in a Patient with Severe Complicated Clostridioides difficile Infection. ACG Case Rep. J. 2022, 9, e00801.
- Wang, Y.; Zhang, S.; Borody, T.J.; Zhang, F.M. Encyclopedia of fecal microbiota transplantation: A review of effectiveness in the treatment of 85 diseases. Chin. Med. J. 2022, 135, 1927–1939.
- Zhang, W.; Jin, Z.; Yang, Z.; Zhang, J.; Ma, X.; Guan, J.; Sun, B.; Chen, X. Fecal Microbiota Transplantation Ameliorates Active Ulcerative Colitis by Downregulating Pro-inflammatory Cytokines in Mucosa and Serum. Front. Microbiol. 2022, 13, 818111.
- Chen, H.; Huang, H.; Xu, H.; Luo, Q.; He, J.; Li, Y.; Zhou, Y.; Nie, Y.; Zhou, Y. Fecal microbiota transplantation ameliorates active ulcerative colitis. Exp. Ther. Med. 2020, 19, 2650–2660.
- Li, P.; Zhang, T.; Xiao, Y.; Tian, L.; Cui, B.; Ji, G.; Liu, Y.-Y.; Zhang, F. Timing for the second fecal microbiota transplantation to maintain the long-term benefit from the first treatment for Crohn’s disease. Appl. Microbiol. Biotechnol. 2018, 103, 349–360.
- Li, Q.; Ding, X.; Liu, Y.; Marcella, C.; Dai, M.; Zhang, T.; Bai, J.; Xiang, L.; Wen, Q.; Cui, B.; et al. Fecal Microbiota Transplantation is a Promising Switch Therapy for Patients with Prior Failure of Infliximab in Crohn’s Disease. Front. Pharmacol. 2021, 12, 658087.
- Chen, M.; Liu, X.L.; Zhang, Y.J.; Nie, Y.Z.; Wu, K.C.; Shi, Y.Q. Efficacy and safety of fecal microbiota transplantation by washed preparation in patients with moderate to severely active ulcerative colitis. J. Dig. Dis. 2020, 21, 621–628.
- Huang, W.-Q.; Huang, H.-L.; Peng, W.; Liu, Y.-D.; Zhou, Y.-L.; Xu, H.-M.; Zhang, L.-J.; Zhao, C.; Nie, Y.-Q. Altered Pattern of Immunoglobulin A-Targeted Microbiota in Inflammatory Bowel Disease After Fecal Transplantation. Front. Microbiol. 2022, 13, 873018.
- Zhao, J.; Bai, M.; Yang, X.; Wang, Y.; Li, R.; Sun, S. Alleviation of refractory IgA nephropathy by intensive fecal microbiota transplantation: The first case reports. Ren. Fail. 2021, 43, 928–933.
- Cai, J.; Chen, X.; He, Y.; Wu, B.; Zhang, M.; Wu, L. Washed microbiota transplantation reduces serum uric acid levels in patients with hyperuricaemia. World J. Clin. Cases 2022, 10, 3401–3413.
- Xie, W.R.; Yang, X.Y.; Deng, Z.H.; Zheng, Y.M.; Zhang, R.; Wu, L.H.; Cai, J.Y.; Kong, L.P.; Xia, H.H.; He, X.X. Effects of washed microbiota transplantation on serum uric acid levels, symptoms and intestinal barrier function in patients with acute and recurrent gout: A pilot study. Dig. Dis. 2022, 40, 684–690.
- Wang, J.; Wang, Y.; Zhang, F.; Su, Y.; Wang, J.; Wu, D.; Hsu, W. Initial experience of fecal microbiota transplantation in gastrointestinal disease: A case series. Kaohsiung J. Med. Sci. 2019, 35, 566–571.
- Chen, L.; Sun, X.; Liu, Z. Application of colonic transendoscopic enteral tubing in the treatment of extensive moderate ulcerative colitis. Chin. J. Digest. Med. Imageol. 2021, 11, 106–110.
- Long, C.; He, Z.; Cui, B.; Zhang, T.; Wen, Q.; Li, Q.; Zhang, J.; Ji, G.; Zhang, F. Methodology, safety and applications of colonic transendoscopic enteral tubing (with video). Chin. J. Dig. Endosc. 2020, 37, 28–32.
- Luo, W.; Xie, W.; Chen, Q.; Xue, L.; He, X. Evaluation of the efficacy and safety of fecal microbiota transplantation in different ways on ulcerative colitis. Chin. J. Gastroenterol. Hepatol. 2020, 29, 1008–1011.
- Zhang, J.; Wu, J.; Wang, S.; Xu, W. Application of transendoscopic enteral tubing in the treatment of extensive colonic ulcerative colitis. J. Pract. Med. 2019, 35, 2824–2827.
- Shen, B.; Kochhar, G.S.; Navaneethan, U.; Cross, R.K.; Farraye, F.A.; Iacucci, M.; Schwartz, D.A.; Gonzalez-Lama, Y.; Schairer, J.; Kiran, R.P.; et al. Endoscopic evaluation of surgically altered bowel in inflammatory bowel disease: A consensus guideline from the Global Interventional Inflammatory Bowel Disease Group. Lancet Gastroenterol. Hepatol. 2021, 6, 482–497.
- Shen, B.; Kochhar, G.; Navaneethan, U.; Farraye, F.A.; Schwartz, D.A.; Iacucci, M.; Bernstein, C.N.; Dryden, G.; Cross, R.; Bruining, D.H.; et al. Practical guidelines on endoscopic treatment for Crohn’s disease strictures: A consensus statement from the Global Interventional Inflammatory Bowel Disease Group. Lancet Gastroenterol. Hepatol. 2020, 5, 393–405.
- Lan, N.; Hull, T.L.; Shen, B. Endoscopic stricturotomy and ileo-colonic resection in patients with primary Crohn’s disease-related distal ileum strictures. Gastroenterol. Rep. 2020, 8, 312–318.
- Zhang, L.; Lan, N.; Wu, X.; Shen, B. Endoscopic stricturotomy in the treatment of anastomotic strictures in inflammatory bowel disease (IBD) and non-IBD patients. Gastroenterol. Rep. 2019, 8, 143–150.
- Book, T.; Kirstein, M.M.; Schneider, A.; Manns, M.P.; Voigtländer, T. Endoscopic decompression of acute intestinal distension is associated with reduced mortality in critically ill patients. BMC Gastroenterol. 2020, 20, 87.
- Hiraki, M.; Tanaka, T.; Okuyama, K.; Kubo, H.; Ikeda, O.; Kitahara, K. Colon perforation caused by transanal decompression tube after laparoscopic low anterior resection: A case report. Int. J. Surg. Case Rep. 2021, 80, 105640.
- Endo, S.; Kumamoto, K.; Enomoto, T.; Koizumi, K.; Kato, H.; Saida, Y. Comparison of survival and perioperative outcome of the colonic stent and the transanal decompression tube placement and emergency surgery for left-sided obstructive colorectal cancer: A retrospective multi-center observational study “The CODOMO study”. Int. J. Color. Dis. 2020, 36, 987–998.
- An, Y.; Wang, N.; Yang, Z.; Li, Y.; Xu, B.; Guo, G.; Sun, M. Efficacy of transanal drainage tube and self-expanding metallic stent in acute left malignant colorectal obstruction. Ann. Palliat. Med. 2020, 9, 1614–1621.
- Endo, K.; Takahashi, S.; Shiga, H.; Kakuta, Y.; Kinouchi, Y.; Shimosegawa, T. Short and long-term outcomes of endoscopic balloon dilatation for Crohn’s disease strictures. World J. Gastroenterol. 2013, 19, 86–91.
- Paspatis, G.A.; Arvanitakis, M.; Dumonceau, J.-M.; Barthet, M.; Saunders, B.; Turino, S.Y.; Dhillon, A.; Fragaki, M.; Gonzalez, J.-M.; Repici, A.; et al. Diagnosis and management of iatrogenic endoscopic perforations: European Society of Gastrointestinal Endoscopy (ESGE) Position Statement—Update 2020. Endoscopy 2020, 52, 792–810.
- Belle, S. Endoscopic Decompression in Colonic Distension. Visc. Med. 2021, 37, 142–148.
- Zhang, T.; Xu, L.J.; Xiang, J.; He, Z.; Peng, Z.Y.; Huang, G.M.; Ji, G.Z.; Zhang, F.M. Cap-assisted endoscopic sclerotherapy for hemorrhoids: Methods, feasibility and efficacy. World J. Gastrointest. Endosc. 2015, 7, 1334–1340.
- Dorrestein, P.C.; Mazmanian, S.K.; Knight, R. Finding the missing links among metabolites, microbes, and the host. Immunity 2014, 40, 824–832.
- Silpe, J.E.; Balskus, E.P. Deciphering Human Microbiota–Host Chemical Interactions. ACS Central Sci. 2020, 7, 20–29.
- Tang, Q.; Jin, G.; Wang, G.; Liu, T.; Liu, X.; Wang, B.; Cao, H. Current Sampling Methods for Gut Microbiota: A Call for More Precise Devices. Front. Cell. Infect. Microbiol. 2020, 10, 151.
- Stearns, J.C.; Lynch, M.D.J.; Senadheera, D.B.; Tenenbaum, H.C.; Goldberg, M.B.; Cvitkovitch, D.G.; Croitoru, K.; Moreno-Hagelsieb, G.; Neufeld, J.D. Bacterial biogeography of the human digestive tract. Sci. Rep. 2011, 1, 170.
- Shen, W.; Sun, J.; Yao, F.; Lin, K.; Yuan, Y.; Chen, Y.; Han, H.; Li, Z.; Zou, J.; Jiao, X. Microbiome in Intestinal Lavage Fluid May Be A Better Indicator in Evaluating the Risk of Developing Colorectal Cancer Compared with Fecal Samples. Transl. Oncol. 2020, 13, 100772.
- Reitmeier, S.; Kiessling, S.; Clavel, T.; List, M.; Almeida, E.L.; Ghosh, T.S.; Neuhaus, K.; Grallert, H.; Linseisen, J.; Skurk, T.; et al. Arrhythmic Gut Microbiome Signatures Predict Risk of Type 2 Diabetes. Cell Host Microbe 2020, 28, 258–272.e6.
- Kuang, Z.; Wang, Y.; Li, Y.; Ye, C.; Ruhn, K.A.; Behrendt, C.L.; Olson, E.N.; Hooper, L.V. The intestinal microbiota programs diurnal rhythms in host metabolism through histone deacetylase 3. Science 2019, 365, 1428–1434.
- Cao, J.; Zhang, Y.; Dai, M.; Xu, J.; Chen, L.; Zhang, F.; Zhao, N.; Wang, J. Profiling of Human Gut Virome with Oxford Nanopore Technology. Med. Microecol. 2020, 4, 100012.
- Liu, X.; Ma, Y.; Yu, Y.; Zhang, W.; Shi, J.; Zhang, X.; Dai, M.; Wang, Y.; Zhang, H.; Zhang, J.; et al. Gut microbial methionine impacts circadian clock gene expression and reactive oxygen species level in host gastrointestinal tract. Protein Cell 2022, pwac021.
- Fawad, J.A.; Luzader, D.H.; Hanson, G.F.; Moutinho, T.J.; McKinney, C.A.; Mitchell, P.G.; Brown-Steinke, K.; Kumar, A.; Park, M.; Lee, S.; et al. Histone deacetylase inhibition by gut microbe-generated short chain fatty acids entrains intestinal epithelial circadian rhythms. Gastroenterology 2022, 163, 1377–1390.e11.