1. Vitamin A and Lutein
Among dietary factors, vitamin intake has become increasingly positive in reducing oxidative stress and, as a result, improving the outcome of many eye pathologies. Vitamin A is a fat-soluble life-essential group of compounds characterized by an unsaturated isoprenoid chain structure. Famously, vitamin A performs important functions including cell proliferation, reproduction, foetal growth and development, vision in darkness, corneal and conjunctiva development, immune system functioning, and central nervous system formation [
62]. Unlike water-soluble vitamins, vitamin A easily accumulates in the body, especially in the liver and adipose tissue. This characteristic determines the advantage of resisting the development of clinical deficiency symptoms, but at the same time, it has the disadvantage of being able to provide accumulation toxicity. Vitamin A can be supplied in the diet both from products of animal origin, such as retinol, and vegetable carotenoids, such as provitamin A [
63]. As already discussed, the retina is responsible for visual perception, mediated through specific structures known as cones and rods that are fundamental for vision in light and dark conditions, respectively. Active vitamin A is associated with a protein receptor coupled to protein G, the complex known as rhodopsin, generating a chain of reactions whose last consequence is the transmission of optical perceptions to the brain via the optic nerve [
62]. Vitamin A is responsible for the maintenance of homeostasis reduction–oxidation. In fact, retinol binds to different proteins, acting as a redox reagent. In addition, carotenoids, such as β-carotene, α-carotene, lutein, lycopene, and cryptoxanthin, are well-known antioxidants [
64,
65]. An excessive intake of vitamin A is potentially toxic; toxicity has been associated with 100,000 RE per day (1 RE = 1 μg retinol) in adults and 10,000 RE per day in children. In women in the first trimester of pregnancy, a dose of 3000–9000 RE per day created teratogenic effects. The Group of Experts on Vitamins and Minerals have not been able to set a safe limit for Vitamin A; therefore, it is recommended that a maximum intake per day is 700 lg for men and 600 lg for women [
66]. Among the approximately 850 types of naturally occurring carotenoids, very few of them are present in human tissues. Among these it is important to mention lutein and its stereoisomers, zeaxanthin and meso-zeaxanthin, present in the human retina [
67]. It is a class of a carotenoid, named xanthophyll, that cannot be synthesized de novo in the human body, and are absorbed only through diet. The most xanthophyll-rich foods, including lutein and zeaxanthin, are leafy green vegetables, such as cabbage, broccoli, peas, spinach, lettuce, and also egg yolk [
68]. These compounds are hydrophobic; however, due to the presence of the hydroxyl group, lutein and zeaxanthin are relatively polar compounds. After their intake, food carotenoids are dispersed in gastric juice and incorporated into lipid droplets, transferred to micelles with food lipids, and finally into the bloodstream. Therefore, fat-rich diets generally facilitate the absorption of dietary carotenoids [
69]. Lutein is particularly concentrated in the central portion of the retina, where the photoreceptor cells, responsible for visual acuity and central vision, are located. In the macula of the retina are found: zeaxanthin, in the middle-peripheral region; meso-zeaxanthin, in the epicentre; and lutein, concentrated in the periphery. The absence of these three cartenoids is often used to predict the risk of developing macular diseases [
69]. Lutein is also found in the lens, protecting it from age-related eye diseases, such as cataracts [
70]. Lutein is retained in the human retina for a prolonged period of time and it has been shown that, even after three months from the interruption of lutein supplementation, the optical density of the macular pigment remains high despite its low serum concentration [
71,
72]. Lutein has been shown to exert an extremely powerful antioxidant action with several mechanisms of action: (1) render the role of the oxygen singlet poorly active; (2) reduce or eliminate free radicals; (3) filter blue light, thereby reducing phototoxic damage to photoreceptor cells; (4) reduce the expression of inducible nitric oxide synthase (iNOS) [
73,
74,
75]. In addition, lutein is able to turn off the inflammatory process, inhibiting the pro-inflammatory cytokine cascade, the expression of nuclear-kB transcription factor (NF-kB), and the activation of the complement system [
76,
77,
78,
79]. Many clinical studies have attributed lutein to antioxidant and anti-inflammatory properties in the eye, justifying a benefit in some diseases such as age-related macular degeneration, diabetic retinopathy, cataracts, retinitis pigmentosa, and myopia [
80,
81]. Lutein supplementation showed a relatively high safety profile and was classified as “GRAS” by the US Food and Drug Administration (FDA) [
82]. Although German, Canadian and American studies have reported daily intakes of lutein of 1.9, 1.4, and 2 mg, respectively [
83,
84], these results have been shown to be undervalued, and the randomized clinical trial “Age-Related Eye Disease Study 2” (AREDS 2) showed a lutein intake of 10 mg per day over 5 years in more than 4000 patients. Subsequently, the Council for Responsible Nutrition (CRN) stated that lutein intake is safe up to 20 mg/day [
85].
2. Vitamin C and Coenzyme Q10
Vitamin C (ascorbic acid) is, chemically, a low-molecular-weight carbohydrate capable of donating electrons to free radicals from both the second and third carbon, quenching their reactivity and acting as a reducing agent. While most vertebrates can synthesize this compound, humans, together with guinea pigs, some fish, birds, and insects, rely exclusively on dietary intake to maintain the body’s levels of vitamin C. This is a hydrophilic vitamin, and despite its small size, it does not cross the plasma membrane by passive diffusion [
86]. During the detoxification reactions of ROS, vitamin C oxidizes to dehydroascorbate, but this oxidized form can subsequently be reduced to generate vitamin C again by glutathione-dependent enzymes. However, if the oxidative damage is continuous, dehydroascorbate undergoes an irreversible degradation; in the event in which vitamin C is present in excessive doses, it can act as a pro-oxidant, contributing to the formation of hydroxyl radicals and increasing oxidative damage. This means that vitamin C can pass from being an antioxidant in physiological conditions to a pro-oxidant under pathological conditions [
87]. Vitamin C is particularly present in the eye in the aqueous humor (saline fluid that is located between the cornea and the crystalline) and vitreous humor (connective tissue of gelatinous consistency occupying the eyeball cavity between the posterior surface of the lens and the retina). Particularly in these districts, its concentration exceeds plasma concentrations by 20 to 70 times [
88]. In the eye, vitamin C absorbs UV light, preventing the penetration of UV rays and subsequent photoinduced oxidative damage in the tissues, behaving as a physiological “sunscreen” [
89]. In addition, vitamin C can scavenge or quench the superoxide anion radical, hydrogen peroxide, hydroxyl radical, singlet oxygen, and reactive nitrogen oxide [
90], protecting the cornea, the lens and other ocular tissues against oxidative damage. Finally, vitamin C has been shown to play a role in the prevention of lipid peroxidation of membranes [
91]. Since it has been shown that individuals with vitamin C deficiency developed cataracts more easily than others, and that there was a close correlation between vitamin C and the health of the crystalline, numerous studies have been conducted on the relationship between vitamin C and the risk of cataracts [
92,
93]. The recommended daily allowance (RDA) based on the intake of vitamin C, is 75 and 90 mg/day for women and men, respectively, established by the U.S. Institute of Medicine (IOM) in 2000 [
94]. Recent data suggest that the current RDA for vitamin C set by the IOM for men and women may be too low. On the basis of a comprehensive review of the scientific evidence, it was concluded that 200 mg/d is the optimum intake of vitamin C for the majority of the adult population, to the advantage of the health benefits for the eye [
95]. Coenzyme Q10 (coQ10) possesses a quinone structure and, for this reason, is also known as ubiquinone. The chemical structure of coQ10 is very similar to that of vitamin K; nevertheless, this cofactor is not considered a vitamin because it is the only fat-soluble antioxidant that animal cells synthesize de novo in the body [
96]. It is found in all cell membranes and its main function is to be a cofactor of the mitochondrial enzymes that cooperate in the formation of ATP, an energy source needed to perform cellular biochemical functions. In particular, this liposoluble compound works to transport the electrons in mitochondria during aerobic cellular respiration, from complex I (NAHD ubiquinone oxioreductase) and complex II (succinate ubiquinone reductase) to complex III (ubiquinone cytochrome c reductase). Another function of coQ10 is to participate in the creation of a proton gradient in the intermembrane space [
97]. This compound also possesses direct and indirect antioxidant properties in its reduced form (CoQ10H
2). The direct antioxidant property is achieved by reducing the accumulation of ROS, while the indirect action occurs with the regeneration of a form of vitamin E (α-tocopherol) [
98]. CoQ10 collaborate in lowering the lysosomal pH, transporting H
+ ions inside, in order to facilitate an acidic environment necessary to degrade cellular debris [
99]. Finally, it has been recognized that coQ10 participates in gene expression, and this could explain its effects on overall tissue metabolism [
100,
101]. Since the quantity of coQ10 present in the body is determined by two sources, biosynthesis [
102,
103] and dietary supplementation, its deficiency may occur for the following reasons: (1) reduced dietary intake; (2) impaired biosynthesis; (3) increased usage by the body [
104]. A shortage of coQ10 is mainly manifested by reduced energy metabolism, impaired protection from free radicals, and deacidification of lysosomes [
105,
106,
107]. Since the retina is the most metabolically active tissue of the body, with the highest consumption of energy (tissue/size ratio), patients with coQ10 deficiency may develop retinopathies, suggesting that coQ10 can play an important role in pathogenesis of retinal conditions [
108,
109]. In addition, a study by Que et al. showed higher coQ10 concentrations in young people (30 years) compared to older human retinas (80 years), highlighting how the oxidative stress plays a key role in the pathogenesis of many age-related diseases, such as atherosclerosis, cataracts, and Alzheimer’s disease [
110,
111,
112]. In this way, the accumulation of ROS in aging results in increased cell damage that mediates the apoptotic mechanisms of cell death [
113]. Age-related macular degeneration (AMD) causes loss of central vision, which has a significant impact on quality of life. Plasma coQ10 levels are substantially reduced in patients with AMD, compared with control patients, and this suggests an association between coQ10 and AMD pathogenesis [
114]. Since the retina and the ocular macula are exposed to light more than any other organ or tissue in the body, these districts will be particularly sensitive to oxidative stress and lipid peroxidation. The result of this oxidative damage leads to apoptotic cell death [
115]. Glaucoma is characterized by the loss of RGC, which are fundamental in the transmission of the signal from the photoreceptors to the optic nerve. As the prevalence of glaucoma increases with age, there may be a possible correlation between RGC and coQ10 deficiency in old age [
116,
117]. Experimental studies have shown that intravitreal administration of coQ10 minimizes apoptosis in RGC. This supported the neuroprotective role of coQ10 [
118,
119]. The normal concentration range of coQ10 in human plasma is 0.8–1.2 mg/L, and in cases of deficiency, supplementation typically given to adults at 1.2–3 g/day [
120].
3. Astaxanthin
Carotenoids are a class of compounds with over 600 natural fat-soluble pigments that play a crucial role in the photosynthetic process, as well as protective activity against damage caused by excessive exposure of light and oxygen. They are taken through the diet, constituting a robust nutritional role as a source of vitamin A [
121]. Their oxygenated derivatives are known as xanthophylls; both classes of pigments share a structural scheme consisting of alternating single and double bonds, responsible for the absorption of the excess energy contained in other molecules and carrying out, accordingly, an antioxidant role [
122]. Astaxanthin, a xanthophyll carotenoid, is a naturally occurring red pigment in numerous living organisms (bacteria, microalgae and yeasts), present as a secondary metabolite. This compound is biosynthesized by phytoplankton and microalgae (such as
Haematococcus pluvialis, Chlorella zofingiensis and
Xanthophyllomyces dendrorhous), which are the basis for the feeding of zooplankton and krill, the ideal food of animal species which store this pigment in the skin and adipose tissue. Finally, all the superior aquatic species that feed on these foods become rings of the trophic chain containing astaxanthin. This carotenoid is responsible for the colouring of some sea creatures, including salmonids, tuna, shrimps, crustaceans, lobsters, and crayfish [
123]. The chemical structure of astaxanthin provides a long chain structure and two terminal polar groups; this particular conformation provides the compound with both lipophilic and hydrophilic properties. Precisely because of this feature, astaxanthin extends through the entire double-layer membrane, carrying out its protective activity both inside and outside the cell membrane [
124,
125]. Astaxanthin has been shown to have numerous beneficial activities on human health, including a protective effect on the skin, the cardiovascular and nervous system, and antioxidant, anti-inflammatory, anti-cancer, and antidiabetic properties, among others [
126,
127]. In the last two decades, the potential role of astaxanthin in protecting eye health has been highlighted, showing a significant improvement in macular degeneration, cataracts, diabetic retinopathy, and glaucoma [
128]. To date, astaxanthin is considered to be the most beneficial antioxidant carotenoid provided in nature; in fact, it is more potent than most known antioxidants, according to the following ratios: 6000 times more powerful than vitamin C; 550 times stronger than vitamin E (alpha-tocopherol); and 40 times more powerful than beta-carotene [
129]. The reason for this exceptional oxidative protection is explained by its chemical structure: the terminal polar groups quench free radicals and the double bonds, its intermediate segment, removes high-energy electrons [
130]. The peculiarity of astaxanthin is to be able to neutralize single oxygens and radicals in both the non-polar (hydrophobic) and polar (hydrophilic) zones [
131]. Several studies have confirmed the antioxidant efficacy of astaxanthin and have identified the reduction of oxidative marker levels, such as malondialdehyde (MDA), and the increase in antioxidant agents including SOD, CAT and GPX1 [
132,
133,
134]. Therefore, we can conclude that astaxanthin exerts antioxidant activities not only through direct scavenging of radicals, but also by activating the cellular antioxidant defense system [
135,
136]. Finally, astaxanthin exerts a robust anti-inflammatory [
137,
138] and anti-apoptotic activity [
139,
140]. In the last two decades, it has been shown that treatment with astaxanthin improves many eye conditions. For example, Otzuka et al., showed that treatment with axanthin 100 mg/kg could inhibit retinal dysfunction caused by light [
141].
Trehalose, also referred to as α,α-Trehalose or α-D-Glucopyranosyl-α-D-glucopyranooside, is a non-reducing disaccharide consisting of two portions of glucose linked through an α,α1,1-glucosidic bond [
150]. This component is usually found in the environment in different species of plants, fungi, algae, bacteria, yeasts, insects, and other lower invertebrates, but never in mammals or other vertebrates. Once ingested with food, trehalose is hydrolyzed in the small intestine in two molecules of D-glucose through the trehalase enzyme. It is also known to be used as a sweetener; in industry as, a stabiliser or packaging material; in the pharmaceutical industry, as an excipient; and in the textile industry, as a texturing agent 2 [
151]. The chemical structure of trehalose justifies the impossibility of crossing cell membranes; to date, it has been established that this compound can penetrate the cytosol through vesicular internalization of endocytosis [
152,
153]. Trehalose has also recently been used for its therapeutic effects in the treatment of cardiometabolic disease and degeneration in animal and human models [
154]. Takahashi et al. [
155] found that trehalose reduced neuronal damage in a model of ischemia in rabbits. In the case of neurodegeneration or traumatic brain injury, oral administration of 2% trehalose has been shown to improve the cognitive characteristics involved in injured brain areas [
156]. In addition, this compound induced the increase of zinc and iron in the brain, essential for the maintenance of brain functions [
157,
158]. Finally, trehalose increased the expression of proteins involved in synaptic activity, neuroprotection, and neurogenesis [
159]. Trehalose has become known for its pro-autophagic action; it is able to eliminate and recycle damaged macromolecules in response to cellular stress. For this reason, it was considered protective against the aggregation of the β-amyloid protein in neuronal cell lines [
160] and metabolic disorders. More generally, it is possible to affirm that the action of this compound guarantees homeostatic paths that depend on the type of tissue involved [
161]. Trehalose has been found to be a stress-reactive factor; in particular, it is a response factor when the cells of the organisms that produce it are exposed to environmental stress, such as heat, cold, dessication, and oxidation. When stress conditions become excessive, these organisms synthesize trehalose, which helps them maintain cellular integrity. With this strategy, these organisms can prevent the denaturation of proteins, facilitate their stabilization, and inhibit protein aggregation [
162,
163]. Another important function of trehalose is to properly moisturize the dried tissues of the organisms that synthesize this compound. This strategy, known as the “water hypothesis”, is based on the ability of trehalose to form hydrogen bonds between its polar groups and lipids or membrane proteins [
164]. In this way, trehalose can maintain the integrity of phospholipids guaranteeing the functional properties of biological membranes [
165]. There is a large volume of evidence that testifies to a specific role of trehalose in performing antioxidant and anti-inflammatory effects and, in recent years, has shown beneficial effects in ophthalmology [
166]. For example, cell exposure to H
2O
2 causes severe oxidative damage to the amino acids of cellular proteins; nevertheless, trehalose is able to reduce such damage, in this way protecting both proteins and lipids of the membrane [
167]. Trehalose has an established ability to maintain the degree of hydration; this compound has been used to protect the cells of the anterior ocular surface in dry-eye disease [
169]. In addition, the effect of trehalose was enhanced when it was added to a single formulation with hyaluronate, an anionic glycosaminoglycan polysaccharide with lubricative and water-retaining properties [
170]. The trehalose highlighted the ability to reduce photodamage caused by UVB radiation in the epithelium of the cornea [
171]. Following UVB irradiation, trehalose was found to reduce the resulting corneal disorders, speeding up healing, suppressing neovascularization, restoring corneal transparency, and restoring proper immunohistochemistry [
172]. Chen and Haddad (2004) also highlighted the effectiveness of trehalose against hypoxic or anoxic lesions. The cornea is not only affected by damage caused by ROS, but also by insufficient oxygen supply. In these cases, apoptotic death occurs; trehalose has been shown to effectively suppress these disorders [
173].
5. Curcumin and Quercetin
Curcumin is a pigment insoluble in water extracted from the rhizome of
Curcuma longa, a species that belongs to the
Zingiberaceae family. The obtained powder contains 2–5% curcumin. Curcumin is a biologically active phytochemical compound with health benefits, and its extract also contains β-carotene, lycopene, epigallocatechin gallate, and quercetin [
174,
175]. In recent years, several studies have confirmed the use of curcumin for the prevention and treatment of many diseases, especially inflammatory diseases and cancer [
176,
177]. Curcumin inhibits the production of free radicals, and therefore shows antioxidant properties [
178]. The effect of curcumin on oxidative damage is based on its ability to scavenge ROS and reactive nitrogen species (RNS) [
179]. It can modulate the activity of active enzymes in the neutralization of free radicals, GSH-Px, CAT, and SOD [
180]. In addition, it can inhibit enzymes that generate ROS, such as lipoxygenase/cyclooxygenase and xanthine hydrogenase/oxidase Finally, being lipophilic, curcumin is able to eliminate peroxylic radicals, behaving like vitmin E. Antioxidant properties of curcumin cause the inhibition of oxidative stress and this reduces the risk for many lifestyle diseases [
181]. In addition, curcumin exerts an anti-inflammatory effect; it lowers the expression of the gene IκBα, gene cyclooxygenase-2 (COX-2), prostaglandin E-2 (PGE-2), interleukin 1-6-8 (IL-1, IL-6, IL-8), and tumor necrosis factor α (TNF-α). The anti-inflammatory effect is also exerted by the ability of curcumin to activate the proliferator-activated peroxisome receptor γ (PPAR-γ), a nuclear receptor protein that binds to the peroxisome proliferator response element (PPRE) and regulates gene transcription [
182]. Recently it has been highlighted that ROS are fundamental regulators of angiogenesis, the process that allows new blood vessels form within the vascular system, and that vascular function critically depends on the amount of ROS present. In fact, while high doses of ROS induce oxidative stress and subsequent cell death, both conditions inhibit angiogenesis; low doses of ROS promote it through some sublethal damage to the cell membrane, subsequently releasing the growth factor of fibroblasts FGF-2, which are directly involved in angiogenesis [
183,
184]. Given the properties of curcumin, this compound could be used in the treatment of diseases related to angiogenesis, including eye diseases [
185,
186]. Most retinal diseases, as already mentioned, imply an abundance of ROS and reduced levels of scavenger antioxidants. In particular, RGC and photoreceptors are extremely sensitive to oxidative stress damage, and it is known that the accumulation of ROS is often involved in several diseases of the retina, such as uveitis, age-related macular degeneration, diabetic retinopathy, retinal tumors, and proliferative vitreoretinopathy (PVR) [
187]. In order to know the effect of curcumin after an oxidative stress insult, Munia et al., have shown that this nutraceutical compound was capable of protecting human retinal epithelial cells from death [
188]. Dry-eye disease is characterized not only by reduced secretion of tears, but also rapid tear evaporation, responsible for the damage to the eye surface [
189]. This disease includes an inflammatory process involving IL-6, IL-8, IL-1β [
190]. It has been shown that curcumin could exert a protective effect through its anti-inflammatory activity, inhibiting the expression of pro-inflammatory cytokines in conjunctiva [
191]. Uveitis is an inflammation of the eye that includes the iris and adjacent tissue. Lal et al. reported an improvement in patients with chronic uveitis who have been given oral capsules of curcumin (75 mg/capsule) [
192]. A decrease in aqueous flare and keratic precipitates was observed after treatment. Its beneficial effects can be derived from their antioxidant, anti-inflammatory, and antifibrinolytic properties [
189]. Because curcumin has low oral solubility and bioavailability, its biomedical potential cannot be exploited in animals and humans [
193]. The exogenous curcumin administered in humans for a period of about 8 weeks has been shown to be able to adequately perform all the functions of this natural compound [
194]. Quercetin is a member of the subclass of flavonols and is abundant in the human diet. It has received considerable attention from the scientific community in recent years thanks to numerous effects on human health, including antioxidant [
195], anti-inflammatory [
196], anti-cancer [
197,
198], anti-aging [
199], and anti-autoimmune effects, [
200] and effects upon metabolic pathologies [
201]. The eye surface serves as a protective and functional barrier for the rest of the eye. Diseases of the eye surface can affect the structure of the cornea or conjunctiva, leading to corneal thinning, inflammation, and visual deficits [
202]. Prolonged inflammation in these districts can lead to a partial or even complete loss of vision, affecting quality of life. Unfortunately, to date, we do not possess a non-invasive treatment that can preserve corneal function; surgery and corneal transplantation remain the only solution [
203]. Given the problems and side effects involved in a corneal transplant, scientists have sought an alternative. The effectiveness of the administration of ocular drugs depends on many factors, including drug absorption, bioavailability, and retention on the front surface. Lipophilic drugs, in general, are associated with increased corneal epithelial permeability, and the solubilization of these compounds in water eye drops was tested. Topical application of quercetin or other flavonoids may be more effective in treating conditions affecting the eye surface [
204]. Studies have shown that a protective role is carried out by quercetin when administered at an average daily consumption of about 16–23 mg/day in human populations [
205,
206,
207]. In
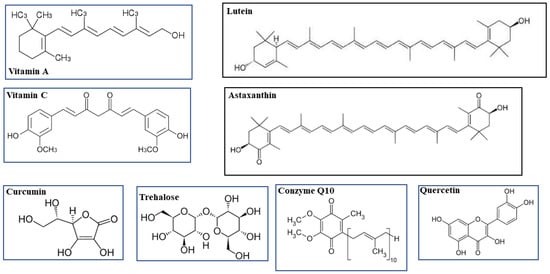
Figure 1, the chemical structures of the examined compounds are represented.
Figure 1. Chemical structures of the examined compounds.
6. PUFAs
Polyunsaturated fatty acids (PUFAs) are lipids whose hydrocarbon chain has a polar hydrophilic end with a carboxyl group (-COOH) and another end with a non-polar hydrophobic methyl group (-CH3). The n-3 and the n-6 represent two classes of PUFAs defined as “essential”, as they must be taken with the diet because humans do not have the desaturases Δ12 and Δ15, enzymes that catalyze the formation of double bonds along the hydrocarbon chain [
208]. Specifically, linoleic acid (LA, 18:2) is the n-6 PUFA from which γ-linolenic and arachidonic acid derive, while from α-linolenic acid (ALA, 18:3), one derives n-3 PUFAs, such as eicosapentaenoic acid (EPA, 20:5 n-3) and docosahexaenoic acid (DHA, 22:6 n-3). LA is present in safflower, soy, and corn oils, while the vegetables that contain ALA are flaxseed, beans, nuts, and the leaves of some green plants. In the liver, the amount of EPA and DHA obtained from the metabolism of ALA is very small, therefore they must be taken with the diet. Both lean and fatty marine fish, fish oil, and algal-derived supplements are particularly rich in EPA and DHA, although they are present in small quantities in many foods of animal origin. For this reason, they must be present in the daily diet [
209]. In particular, EPA and DHA can be present in cellular phospholipid membranes and have powerful antioxidant and anti-inflammatory effects [
210]. The positive effects of taking n-3 PUFAs are well documented; in fact, the long-term effects against certain pathologies, such as cardiovascular diseases, neurodegenerative diseases, and osteoarthritis, are known [
211]. The n-3 PUFAs are also implicated in diseases affecting the eye. For example, in the case of neovascular eye diseases, such as retinopathy of prematurity, diabetic retinopathy, and age-related macular degeneration, current therapies have significant side effects. Clinical and experimental investigations have shown that such treatments could be accompanied by a higher intake of n-3 PUFAs [
212]. Despite conflicting results between fundamental and clinical research, it appears that PUFAs can act positively on the damage that determines the pathogenesis of glaucoma [
213]. Indeed, the effect of PUFAs can be both on intraocular pressure (IOP) and on survival of RGCs. In the first case, endogenous prostaglandins (PGs), obtained from the metabolism of PUFAs, by activating the EP4 and FP receptors, reduce IOP. In the second case, thanks to their anti-inflammatory and antioxidant effects, n-3 PUFAs can reduce the inflammation and oxidative stress responsible for the RGC dysfunction or death [
214]. In particular, patients with pseudoexfoliative (PEX) glaucoma have benefited from the administration of a high, rich DHA nutraceutical formulation that reduced oxidative stress and inflammation. The fact that PUFAs may have beneficial effects for glaucoma is linked to their positive action on endothelial dysfunction and atherosclerosis [
215]. Regarding cataracts, a study was conducted on male Wistar rats, in which it was found that the antioxidant and anti-inflammatory activity of lutein increased in the presence of EPA + DHA [
216]. In particular, micellar lutein with EPA + DHA has been shown to positively regulate α-crystalline chaperone function [
217]. Chang et al. demonstrated a reduction in free fatty acid levels in patients with senile cataracts compared with normal controls. The levels of DHA were particularly low [
168]. Studies on the molecular mechanisms responsible for aging in the eye have allowed us to define the involvement of the ELOVL2 (elongation of very-long-chain fatty acids-like 2) enzyme in the regulation of molecular aging in the retina [
218]. The ELOVL2 enzyme catalyzes an elongation reaction of n-3 and n-6 PUFAs, which are essential for retinal function. DHA is the main PUFA in the retina and is involved in the photoreceptor function in retinal development and has an antioxidant role [
219]. The involvement of PUFAs in AMD, which is the leading cause of blindness in the elderly, has been demonstrated. In particular, the analysis of the eyes of subjects with AMD showed a reduction in PUFAs, and a direct correlation was also reported between the reduced dietary intake of n-3 PUFAs and the increased risk of AMD. Given the function of the ELOVL2 enzyme, it appears that this is directly involved in the onset of AMD along with PUFAs [
220].
7. Grape Seed Extract and Bergamot Polyphenolic Fraction
Grape seed extract has shown beneficial effects in many diseases, thanks to its composition as a flavonoid polyphenolic compound; its main components are: +catechin, −epicatechin gallate, gallate and −epigallocatechin [
230]. Beneficial properties of grape seed include prevention and treatment of diabetes and its complications [
231], prevention of obesity and inflammatory reaction [
232,
233], the ability to modify early cerebrovascular injury caused by hypertension [
234], alleviation of exercise fatigue [
235], protection of the myocardium from injury [
236], lowering blood lipids, regulating the metabolism, and improving the intestinal flora [
237,
238]. Most of these activities are carried out thanks to the antioxidant effect of grape seed extract, which makes it more powerful and effective than other plant polyphenolic compounds [
239,
240]. Among the active ingredients present in grape seed extract, proanthocyanidins are responsible for the biological, therapeutic and pharmacological properties [
241]. Many studies have looked at the correlation between grape seed and eye disease: for example, Mani Satyam et al. showed in an in vivo study in rats that the administration of grape seed extract one day before treatment with sodium selenite, capable of inducing cataract formation in animals, was able to significantly reduce the disease and its damage [
242]. Another recent study showed that treatment with grape seed extracts was able to reduce the damage of retinal degeneration caused by aging, by attenuating the expression of some pro-inflammatory cytokines [interleukin 6 (IL-6), IL-12 and IL-1β)] or the formation of their messenger RNAs [
243]. The protective effects of grape seed proanthocyanidins on retinal ganglion cells have also been confirmed by an important study by Li et al., demonstrating this result in several neurodegenerative disorders [
244].
This entry is adapted from the peer-reviewed paper 10.3390/life13010077