Metastatic breast cancer (MBC) remains in most cases an incurable disease with genetic complexity and heterogeneity. Improvements in classification and management have been introduced, in addition to the development of endocrine and anti-HER2 targeted therapies. Cytological material can be processed for ancillary testing for diagnostic and therapeutic purposes. Reassessment of receptor status is indicated due to changes in tumor biology and metastatic presentation. PD-L1 expression is the only approved biomarker for predicting immune checkpoint inhibitor response in metastatic TNBC, evaluated by immunostaining. The feasibility of applying PD-L1 assays in MBC cytological samples can be recommended, with the adoption of a combined positive score. Non-formalin cytological samples provide higher purity, cellular yield, and better tumor fraction for single-multi gene assays. In MBC, molecular tests enable personalized therapy such as PIK3CA, NTRK fusion genes, and MSI. Cytopathology combined with molecular analysis must be performed effectively in routine clinical practice, through procedure standardization and experience dissemination.
1. Introduction
Approximately 30% of female cancers are breast cancer (BC), which continues to be the most common disease in the world with a mortality-to-incidence ratio of 15% [
1]. The vast majority of deaths due to breast cancer are attributed to metastasis and its associated relapse, which usually occurs in patients ~5–20 years after their first diagnosis [
2]. Around 30% of breast cancer patients still relapse with distant metastasis [
3]. Even they were reported as metastasis-free at the time of diagnosis, nearly 25% of patients with node-negative breast cancer develop metastases [
4]. When metastatic breast cancer (MBC) is diagnosed, the 5-year survival rate is in the range of 38% [
5].
The most common sites of breast carcinoma metastases are the bones, liver, lungs, and brain [
2], but other secondary localizations have been described in the literature, including those of the peritoneal cavity [
6]. Different patterns of metastatic sites in breast cancer are observed according to the hormone receptor, HER2 subtype, and histological type. The comprehension of primary and metastatic disease has advanced significantly, allowing the characterization of biomarkers and adequate follow-up for different groups of patients.
In the approach of metastatic disease, fine needle aspiration cytology (FNAC) can be the diagnostic technique of first choice for the documentation of suspected metastases [
8]. The minimally invasive nature of cytological procedures facilitates tissue sampling, can be applied to several types of metastatic lesions, and is useful for patients in poor general conditions. The demands and implementation of cytology on metastatic breast cancer are increasing with the advances in radiological and endoscopic techniques for obtaining cytological material.
2. Metastatic Breast Cancer: Molecular Cytological Approach
2.1. Immunocytochemistry Biomarkers: Receptor Status
ICC biomarker tests in MBC are recommended in the guidelines of the American Society of Clinical Oncology (ASCO)/American Pathology Association [
11]. Three breast cancer subtypes were defined based on immunostaining estrogen receptor (ER), progesterone receptor (PR), and human epidermal growth factor receptor 2 (HER2) status: Hormone receptor (HR)+/HER2− subtype was defined by HR positive (either ER or PR positive) and HER2− status; HER2+ subtype by HER2 positivity as assessed by IHC and in situ hybridization in case of 2+ IHC score; and triple negative (TNBC) subtype by lack of expression of ER, PR and HER2 [
12].
ER, PR, and HER2 status are critical predictive markers for most of the currently available targeted treatments. HR+ cancers are found to have increased metastasis to the bone. HER-2+ and TNBC subtypes are associated with brain metastasis. Metastases to the lung and bones are frequently seen in TNBC tumors, whereas there appears to be a higher rate of liver metastasis in HER2 positive breast cancer subtypes [
5].
The use of cytology specimens for receptor analysis is a rapid, inexpensive, and less invasive alternative to biopsy at metastatic sites and in metastatic breast cancer patients [
13]. Following specific validation, immunostaining can be performed on any cytological preparation, including cellblocks (CBs), cytospins, smears, and liquid-based cytology (LBC) [
14], particularly in cellblocks and LBC sediments.
Cellblocks have technical advantages over other cytological preparations; they can produce a greater number of sections, which is appropriate for an immunostaining panel. Additionally, samples are embedded in paraffin, and antigen retrieval techniques are identical to those used in histology; therefore, marker validation is not necessary. Studies have been reported in which the results of analysis for receptors in fine-needle aspiration CBs fixed in 10% buffered formalin showed excellent agreement with those in the corresponding tissue blocks, including solid tumors at metastatic sites [
15].
Aspiration cytology is particularly useful in the assessment of breast cancers, allowing a sampling that frames the spatial heterogeneity common to this neoplasm. MBC after therapy for early breast cancer (EBC) tends to have more aggressive tumor biology and a worse outcome compared with de novo MBC [
7,
18]. Thus, improvements in EBC therapies seem to have led to an alteration in tumor biology and metastasis presentation in subsequent MBC, presumably resulting from a molecular selection process [
5]. The discrepancies are responsible for a therapy regimen change in 14–20% of patients [
19].
2.2. Immunocytochemistry Biomarkers: Program Death Ligand-1 (PD-L1)
PD-L1 expression, as assessed by immunohistochemistry, is the only established biomarker for predicting the response to immune checkpoint inhibitors in metastatic TNBC. PD-L1 positivity predicted the efficacy of pembrolizumab (Clone 22C3) in combination with first-line chemotherapy for advanced TNBC [
12].
According to recent NCCN guidelines [
12], PD-L1 expression in TNBC is determined by using Combined Positive Score (CPS), which is the number of PD-L1 staining cells (tumor cells, lymphocytes, macrophages) divided by the total number of viable tumor cells, multiplied by 100, with a cut-off ≥10%.
A minimum of 100 viable tumor cells must be present for the specimen to be considered adequate for PD-L1 evaluation. Any perceptible and convincing partial or complete linear membrane staining (≥1+) of viable tumor cells, lymphocytes, and macrophages that are perceived as distinct from cytoplasmic staining is considered PD-L1 staining and should be included in the scoring [
33].
2.3. Genomic Biomarkers
For metastatic breast cancer, the goal of molecular testing is to find tumor-specific mutations and then target therapy already approved or under study in clinical trials to increase survival and quality of life [
36]. The European Society of Medical Oncology (ESMO) recommends including MBC patients in molecular screening programs to assess targeted therapies [
37], either in the framework of multigene panels or to test specific genes that allow for personalized therapy.
Molecular tests are significantly influenced by pre-analytical and analytical tissue management [
43]. The analytical sensitivity of each molecular assay varies according to the amount and quality of DNA/RNA extracted from the sample tumor. Molecular platforms require approximately a range from 1 ng to 200 ng input nucleic acid masses (10 ng usual minimum input for most NGS assays). A fraction of malignant cells greater than 10% to 20% is generally considered a lower acceptable limit for these methods [
41]. Most NGS assays demand approximately between 1000–5000 cells [
43].
FNAC can be used in routine diagnostic workflow and clinical trials for tumor molecular profiling. The viability is related to the higher purity of the samples, as in smears and touch preparations. The adoption of non-cross-linking alcoholic reagents may yield superior results in terms of quality and quantity of extracted nucleic acids with respect to formalin [
42]. About three to fourfold more cells are required from an FFPE sample from ethanol-fixed material to isolate 10 ng of nucleic acids [
44].
Among the different cytological preparations, recent researches have validated the viability of adopting supernatant fluids for NGS analysis [
45,
46], while CBs and smears have shown to be appropriate for more complex NGS analysis, such as tumor mutational burden profiling [
47]. To prevent medico-legal problems, whole slide scanning and digital storage are required when only one diagnostic slide is available for testing [
48].
The genomic alterations in MBC include ERBB2 amplifications, PIK3CA mutations, germline BRCA 1/2 mutations, somatic BRCA 1/2 mutations, NTRK fusions, ESR1 mutations (mechanism of resistance), PTEN mutations, AKT1
E17K mutations, NF1 mutations (resistance biomarker), MDM2 amplifications, ERBB3 mutations, and microsatellite instability (MSI) [
37]. According to the ESMO Scale for Clinical Actionability of Molecular Targets (ESCAT), only five molecular alterations are associated with breast cancer treatment efficacy with the highest level of evidence (ESCAT I): ERBB2 amplification, germline BRCA1/2 mutations, PIK3CA mutations, MSI, and NTRK fusion [
37].
Therapeutically relevant genomic biomarkers to be assessed concerning immunochemistry classification include: germline BRCA1/2 mutations in HER2-negative MBC; somatic BRCA mutations in HER2-low MBC; PIK3CA, germline BRCA1/2 mutations, PALB2 mutations (optional), and ESR1 (optional) in ER positive, HER2-negative MBC; PD-L1, germline BRCA1/2 mutations, and PALB2 mutations (optional) in TNBC tumors; and in all patients MSI, TMB, and NTRK only if corresponding therapies are available [
5,
49].
3. Conclusions
The genomic scenery of metastatic breast cancer is enriched in druggable genomic drivers and is more complex than early breast cancer [
50]. Identifying these genomic alterations and consequently targeted treatments is the goal of personalized medicine. It is important to emphasize that molecular diagnosis from small cytological and/or tissue samples has been working for patients with advanced lung cancer [
54], with encouraging effects in reducing mortality and increasing survival [
55].
The exploration of cytological specimens seems closer and more connected with current precision oncology, in which cancer characterization, in both the diagnostic and therapeutic fields, focuses on the “smallest” level: the molecular. For this purpose, the cytopathological method has inherent advantages related to its minimally invasive nature, which may allow an easier approach, greater sampling, and greater tumor representativeness, which are essential in the heterogeneous landscape common to the tumor biology and evolution of MBC.
For ancillary testing in advanced breast cancer, the use of cytological specimens can offer two advantages. The variety of cytological preparations available from FNAC enables the selection of certain preparations for each type of test based on its performance and sensitivity. Second, non-FFPE FNA samples provide higher purity, higher cellular yield, and a better tumor fraction for molecular testing. The benefits of cytological processing for ancillary tests extend particularly to the most common metastatic site of breast cancer. Bone FNA samples do not require exposure to decalcifying agents, which are well known to have a marked effect on hormone receptor tests and molecular assays.
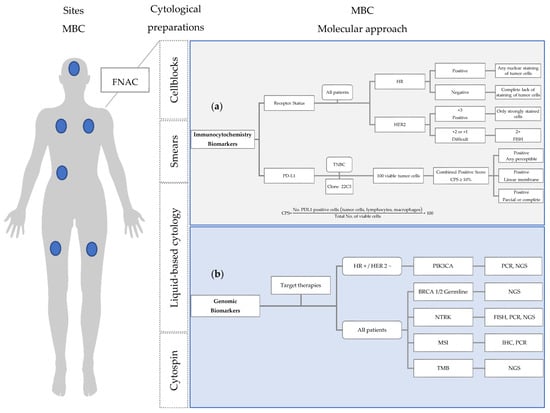
To that end, a framework for a practical approach in the characterization of MBC hallmarks, with information on standardization for cytological processing and diagnosis is outlined (Figure 1)
Figure 1. Molecular approach in the characterization of MBC hallmarks, using cytological preparations: (a) Immunocytochemistry biomarkers: Criteria for assessing HR and HER2 receptor status and PD-L1 expression in cytological material; (b) Genomic biomarkers: therapeutically relevant molecular changes in MBC and detection methods. FISH: fluorescence in situ hybridization; HR: hormone receptor; FNAC: fine needle aspiration cytology; MBC: metastatic breast cancer; NGS: next generation sequencing; PCR: polymerase chain reaction; TNBC: triple negative breast cancer.
This entry is adapted from the peer-reviewed paper 10.3390/jmp3040028