Rehabilitation is the process of treating post-stroke consequences. Impaired limbs are considered the common outcomes of stroke, which require a professional therapist to rehabilitate the impaired limbs and restore fully or partially its function. Due to the shortage in the number of therapists and other considerations, researchers have been working on developing robots that have the ability to perform the rehabilitation process. During the last two decades, different robots were invented to help in rehabilitation procedures. This paper explains the types of rehabilitation treatments and robot classifications. In addition, a few examples of well-known rehabilitation robots will be explained in terms of their efficiency and controlling mechanisms
- exoskeleton
- electromyograph
- rehabilitation robots
- stroke
1. Introduction
The World Health Organization reported that around 15 million people suffer from stroke yearly; around six million of them become disabled. The disabilities vary form fully paralyzed limbs to weakness[1][2].
Scientists have found that particular activities of the brain can be transferred to a different location in the brain, and this is known as neuroplasticity[3]. Studies showed that repetitive motions for the impaired limbs allow the brain to develop new neural pathways and, ultimately, restore full or partial control of motor functions[2].
Impaired functions can be fully or partially restored by investigating neuroplasticity[4]. Using a rehabilitation robot could trigger neuroplasticity by providing a repetitive exercise for the impaired functions. In this respect, rehabilitation robots are defined as an operated machine that is designed to perform specific movements[2].
The importance of using a rehabilitation robot comes from its ability to provide quantitative and continuous monitoring for patient performances during the training, which allows us to understand the recovery mechanism during the repeated tasks[5].
2. Rehabilitation Robots and Their Classifications
2.1. According to Robot Treatment Approaches
Rehabilitation robots can be classified into two types, according to their treatment approaches. The first approach is continuous passive movement (CPM). CPM requires no volunteer effort performed by the patient where the limb is controlled and moved by the robot[6]. CPM treatment reduces muscle tone, which eventually improves the mobility of muscles, joints and tendons[5]. Furthermore, CPM activates the cortical area that has the corresponding sensorimotor and leads to an action similar to normal movement[5]. The second approach is active-assisted movement, where the robot requires a signal from the patient to perform the movement. This signal could be an electromyogram (EMG) and follows the patient’s intention to move the limb[7]. Rehabilitation robots with active-assisted movement require voluntary effort from the patient and, consequently, provide significant motor improvement when they are compared to CPM rehabilitation[5]. Therefore, most of the current researchers focus on active-assisted rehabilitation using robots[5].
The EMG-driven robots use an EMG signal an as “on-off” controller, which means that, once the patient voluntarily initiates the robot, the robot will repeat its action for a period of time. Then, the patient will be allowed another voluntary signal[8].
2.2. According to the Robot Structures
Rehabilitation robots are also classified as end-effectors and exoskeleton robots[9]. End-effectors are simple robots that have a distal movable handle, and the patient attaches his/her hand to this handle and follows a specific trajectory[10]. This kind of robot is characterized by its ability to adapt to different sizes and shapes of movements, as the rehabilitation process requires[11]. End-effector robots have the disadvantage of not providing a rotation movement, which makes it not suitable for pronation and supination movements[2]. End-effectors have been developed recently to provide bilateral rehabilitation training, where the impaired limb copies the movement of the unimpaired limb in a synchronized behavior[12]. Some researchers have reported that bilateral rehabilitation has the feature of activating the impaired hemisphere by making the left side and the right side of the body follow the same trajectory[13].
Exoskeleton robots are characterized by encapsulating the limb with a splint or bionic structure[14]. Exoskeleton robots calculate the required torque for each joint and control the limb movements[15]. In comparison with end-effector robots, exoskeletons require a smaller working environment. Exoskeleton robots, however, comprise the limb joint axes as they provide a very specific movement[2]. In addition, exoskeleton robots are not feasible for bilateral rehabilitation, as the right limb exoskeleton cannot be used for the left limb, and eventually, it is expensive to design right and left exoskeleton robots to perform bilateral rehabilitation training[12] [22].
3. Examples of Rehabilitation Robots
Designing a rehabilitation robot faces a few challenges that have to be considered first[16]. Electromechanical implementation is one of these challenges, which refers to that the robot has to be light, durable, flexible and have the mechanism to perform a normal muscle motion[17]. The interpretation of user intent is another challenge, where the human–robot interaction plays an important role in the rehabilitation process[16]. A neural muscle signal is one of the tools that is used to extract the user’s intent[18]. In addition, a robot’s degrees of freedom (DOF) and the safety precautions should be taken into account in designing the rehabilitation robot; otherwise, the safety and the efficiency of the robot will be compromised[18][19]. The following are some examples of well-known rehabilitation robots[20]. Table 1 summarizes the characteristics of the rehabilitation robots.
Table 1. Characteristics of the rehabilitation robots. DOF: degrees of freedom, MIME: mirror image movement enabler, ARM: Assisted Rehabilitation and Measurement, CADEN-7: cable actuated dexterous exoskeleton for neuro-rehabilitation with seven degrees of freedom, T-Wrex: therapy Wilmington exoskeleton and BONES: Biomimetic Orthosis for Neurorehabilitation.
|
Characteristics
Type of Robot |
Targeted Impaired Functions |
Number of DOF Provided |
Therapy Classification |
Security Precautions |
|
MIT-MANUS |
Upper limb rehabilitation |
Five DOF |
Passive |
· Therapy session has to be monitored by a therapist. · Magnet safety lock is equipped to provide further safety. · MANUS provides a low torque to avoid limb fatigue. |
|
MIME |
Upper limb rehabilitation (Shoulder and Elbow) |
Six DOF |
Passive Active |
· The affected limb is strapped by a splint. · The performance is guided by a PUMA robot. |
|
ARM Guide |
Upper limb function |
One DOF |
Passive Active |
One DOF that provides linear constraints. |
|
ARMin |
Upper limb rehabilitation |
Seven DOF |
Passive |
· Robot has no sharp edges. · Robot has several positions sensors. · Unique software to monitor the performance. |
|
CADEN-7 |
Upper limb rehabilitation |
Seven DOF |
Passive Active |
Three levels of safety: mechanical, electrical and software. |
|
L-EXOS |
Upper limb rehabilitation |
Five DOF |
Active |
· Maximum velocity is 10 rpm. · Maximum torque is 120 Nm. |
|
T-Wrex |
Upper limb rehabilitation |
Five DOF |
Active |
Positions sensors and custom grip sensors |
|
REHAROB |
Upper limb rehabilitation (Shoulder and Elbow) |
Three DOF |
Passive |
Sensors to control and monitor the generated forces. |
|
BONES |
Upper limb rehabilitation |
Four DOF |
Active |
One extra actuator is added for safety issues. |
3.1. MIT-MANUS
MIT-MANUS is a CPM robotic workstation developed by the Massachusetts Institute of Technology that is used to rehabilitate upper limbs post-stroke[21]. MIT-MANUS is an interactive workstation where the patient has to visually interact with a PC game to follow specific movements[17]. The MANUS workstation provides five degrees of freedom, two translation degrees of freedom for the elbow and the forearm, represented by flexion/extension and pronation/supination, respectively. In addition, three degrees of freedom for the wrist, represented by flexion/extension, pronation/supination and abduction/adduction[21]. A magnet safety lock is used to attach the patient’s hand to the device; this technique provides an easy procedure to free the patient from the device[21]. Furthermore, the MANUS workstation provides low torques[21]. Therapy sessions, however, have to be monitored by a therapist to ensure the patient’s safety[18]. The MANUS workstation is characterized by its impedance control, which provides a specific movement to the limbs[21]. The MANUS workstation records the patient’s performance (specifically, the force, velocity and the position); then, the performance data are sent to the control computer to adapt the robot according to the patient’s requirements[22]. The MANUS workstation has been experimentally proven to provide therapeutic effects for upper limb impairment[8].
3.2. MIME
Mirror image movement enabler (MIME) is a CPM robotic system that consists of a wheelchair and height-adjustable table[23], where the patient sits on the wheelchair and puts his/her affected limb on the adjustable table. The affected limb is strapped into the forearm splint that restricts the movements of the wrist and the hand[23]. A Puma 560 (Programmable Universal Machine for Assembly) robot was used as the manipulator, where the robot attached to the splint and applied force to the affected limb during its movements[24]. The Puma 560 robot provided six degrees of freedom, which provided a large range of movement positions in a 3D space[25]. MIME, provides the three treatments modes that are the passive, active-assistive/active-resistive and bilateral modes[17]. In addition, MIME is commonly used in the passive and active-resistive modes[12]. In the passive mode, the robot moves the limb in a specific trajectory towards the target. The active-resistive mode involves prohibiting the limb’s movements in the identified trajectory by providing a viscous resistance, and the patient has to provide maximal effort to reach the target[26]. MIME is used to strengthen the muscles and improve the limb’s motions[8].
3.3. Assisted Rehabilitation and Measurement (ARM) Guide
The Assisted Rehabilitation and Measurement guide (ARM guide) is also an example of a CPM rehabilitation robot and is used for the training and evaluating of upper limb functions[27]. The ARM guide, shown in Figure 1, uses the reaching principle as a therapy technique, where the patient’s arm is attached to a splint, and the patient is advised to reach for things[17]. The ARM guide provides one degree of freedom on a linear constraint rather than multiple active degrees of freedom. Therefore, the ARM guide is considered as an inexpensive and a simple rehabilitation robot[27]. The orientation of the ARM guide can be changed vertically or horizontally[27].
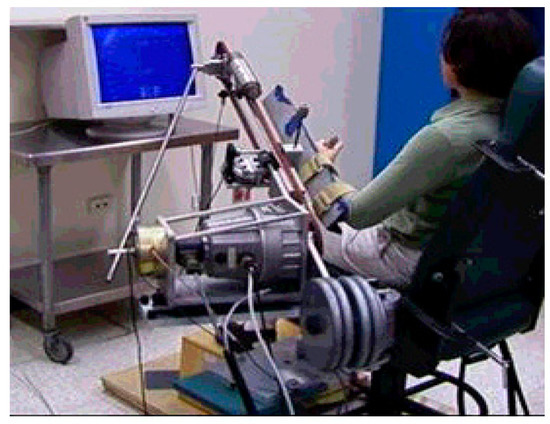
Figure 1. Assisted Rehabilitation and Measurement (ARM) guide robotic system. Source:[27].
3.4. ARMin
ARMin is an upper limb rehabilitation robot and is characterized by providing seven degrees of freedom (DOF), allowing shoulder rotations in three dimensions, flexion/extension of the elbow, supination/ pronation of the forearm and flexion/ extension of the wrist, in addition to supporting the closing and opening of the hand[28]. ARMin consists of a chair and robotic arm, where the seated patient attaches his/her hand to the robotic arm and adjusts its length to its optimum, as shown in Figure 2[29][30]. ARMin has three levels of safety, where the device is equipped by many sensors that work as a system to detect any malfunction that could arise. Secondly, the ARMin has no sharp edges, and no joint will move out of the range of a human limb[28]. Thirdly, a unique algorithm was developed to monitor the repeated motions, and immediate shutdown happens in case of malware being found[24].
The results showed an improvement in the limb’s motion, where the user was able to extend his/her limb to further distances. In addition, the strength of the support was decreased gradually as the patient recovered their motor sensory[18][30].
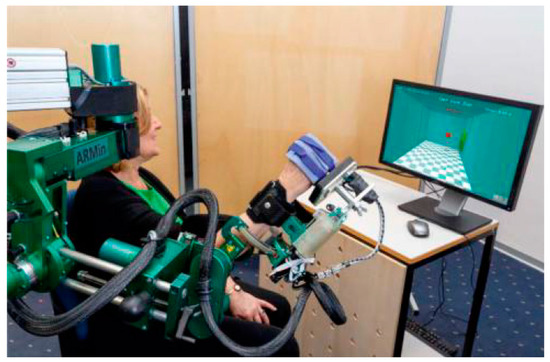
Figure 2. ARMin rehabilitation robot. Source:[30].
3.5. Cable Actuated Dexterous Exoskeleton for Neuro-Rehabilitation with Seven Degrees of Freedom (CADEN-7)
Cable actuated dexterous exoskeleton for neuro-rehabilitation (CADEN-7) provides seven degrees of freedom[31]. CADEN-7 is considered an active-assisted robot that uses surface electromyography to control the upper limb[32]. CADEN-7 is also equipped with three levels of safety, taking into consideration the electrical aspects, mechanical aspects and software aspects[31]. The unique design of CADEN-7 makes it suitable to avoid hyperextension and erratic motions. CADEN-7, however, has to be fixed on external forms and cannot be portable due its size and weight[18].
3.6. L-EXOS
The Light Exoskeleton (L-EXOS) system focuses on providing repetitive movements and gives a simultaneous measurement for the therapeutic progress[33]. L-EXOS, incorporates visual reality to guide the patient to a specific trajectory[34]. In terms of safety concerns, L-EXOS provides a velocity equal to 10 rpm, and the maximum torque cannot exceed 120 Nm. In addition, L-EXOS provides five degrees of freedom, and each movement is equipped by a sensor[18].
3.7. Therapy Wilmington Exoskeleton (T-Wrex)
The therapy Wilmington exoskeleton (T-Wrex) is an active upper limb rehabilitation robot with five degrees of freedom[35][36]. It is dedicated for individuals with significant arm weakness by providing intensive training. The T-Wrex uses the feature of gravity compensation or antigravity for the entire arm, where the patient experiences the sense of a floating arm in space[36]. In addition, the T-Wrex is characterized by providing a large 3D movement that naturalizes the upper limb movements[35]. The T-Wrex consists of two links attached to the forearm and upper arm. In terms of safety, position sensors and custom grip sensors are integrated to the robot, which provide movement measurements for the upper limb[35].
3.8. REHAROB
The Rehabilitation Robot (REHAROB) therapeutic system is a passive rehabilitation robot with three degrees of freedom dedicated for the shoulder and the elbow[36]. The movement trajectory is preprogrammed by the therapist and followed by repetitive movement for the impaired limb. The exercises performed by REHAROB are different than those performed by MIT-MANUS and MIME by providing slow repetitive movements with a constant velocity[37]. These kinds of exercises are efficient in reducing spasticity and increasing the range of mobility for the shoulder and elbow joints[37]. The patient’s upper arm and forearm are attached to the robot’s arm[38]. The REHAROB is equipped by sensors to control and monitor the generated forces[37].
3.9. Exoskeleton Biomimetic Orthosis for Neurorehabilitation (BONES)
The Biomimetic Orthosis for Neurorehabilitation (BONES) is an active rehabilitation robot with four degrees of freedom[36]. The BONES is characterized by its ability to provide arm internal/external rotations without the need to bring or use any bearing element. The unique design was inspired by human biomechanics. In addition, the BONES occupies five actuators to provide a wide range of motion for the upper limb and further measurements for safety issues[39].
This entry is adapted from the peer-reviewed paper 10.3390/app10196976
References
- Lujain Alrabghi; Raghad Alnemari; Rawan Aloteebi; Hamad Alshammari; Mustafa Ayyad; Mohammed Al Ibrahim; Mohsen Alotayfi; Turki Bugshan; Abdullah Alfaifi; Hussain Aljuwayd; et al. Stroke types and management. International Journal Of Community Medicine And Public Health 2018, 5, 3715, 10.18203/2394-6040.ijcmph20183439.
- Robert Bogue; Rehabilitation robots. Industrial Robot: An International Journal 2018, 45, 301-306, 10.1108/ir-03-2018-0046.
- Ori Ossmy; Roy Mukamel; Perception as a Route for Motor Skill Learning: Perspectives from Neuroscience. Neuroscience 2018, 382, 144-153, 10.1016/j.neuroscience.2018.04.016.
- Subasi, A. Electromyogram-Controlled Assistive Devices; Elsevier Ltd.: Amsterdam, The Netherlands, 2019; pp. 285–311. ISBN 9780081024201.
- Xiao Ling Hu; Kai-Yu Tong; Rong Song; Xiu Juan Zheng; Wallace W. F. Leung; A Comparison Between Electromyography-Driven Robot and Passive Motion Device on Wrist Rehabilitation for Chronic Stroke. Neurorehabilitation and Neural Repair 2009, 23, 837-846, 10.1177/1545968309338191.
- Zhang, H.; Austin, H.; Buchanan, S.; Herman, R.; Koeneman, J.; He, J. Feasibility studies of robot-assisted stroke rehabilitation at clinic and home settings using RUPERT. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011.
- J.D. Sanjuan; A.D. Castillo; M.A. Padilla; M.C. Quintero; E.E. Gutierrez; I.P. Sampayo; J.R. Hernandez; M.H. Rahman; Cable driven exoskeleton for upper-limb rehabilitation: A design review. Robotics and Autonomous Systems 2020, 126, 103445, 10.1016/j.robot.2020.103445.
- Rong Song; Kai-Yu Tong; Xiao-Ling Hu; Le Li; Raymond K Y Tong; Assistive Control System Using Continuous Myoelectric Signal in Robot-Aided Arm Training for Patients After Stroke. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2008, 16, 371-379, 10.1109/tnsre.2008.926707.
- Tobias Nef; Gabriela Quinter; Roland Müller; Robert Riener; Effects of Arm Training with the Robotic Device ARMin I in Chronic Stroke: Three Single Cases. Neurodegenerative Diseases 2009, 6, 240-251, 10.1159/000262444.
- Rasedul Islam; Christopher Spiewak; Mohammad Habibur Rahman; Raouf Fareh; A Brief Review on Robotic Exoskeletons for Upper Extremity Rehabilitation to Find the Gap between Research Porotype and Commercial Type. Advances in Robotics & Automation 2017, 6, 1-12, 10.4172/2168-9695.1000177.
- Rachele Bertani; Corrado Melegari; Maria C. De Cola; Alessia Bramanti; Placido Bramanti; Rocco Salvatore Calabrò; Effects of robot-assisted upper limb rehabilitation in stroke patients: a systematic review with meta-analysis. Neurological Sciences 2017, 38, 1561-1569, 10.1007/s10072-017-2995-5.
- Bo Sheng; Yanxin Zhang; Wei Meng; Chao Deng; Shengquan Xie; Bilateral robots for upper-limb stroke rehabilitation: State of the art and future prospects. Medical Engineering & Physics 2016, 38, 587-606, 10.1016/j.medengphy.2016.04.004.
- Qing Miao; Mingming Zhang; Andrew McDaid; Yuxin Peng; Sheng Q. Xie; A robot-assisted bilateral upper limb training strategy with subject-specific workspace: A pilot study. Robotics and Autonomous Systems 2020, 124, 103334, 10.1016/j.robot.2019.103334.
- Benedetta Cesqui; Peppino Tropea; Silvestro Micera; Hermano Igo Krebs; EMG-based pattern recognition approach in post stroke robot-aided rehabilitation: a feasibility study. Journal of NeuroEngineering and Rehabilitation 2013, 10, 75-75, 10.1186/1743-0003-10-75.
- Sebastian Głowiński; Andrzej Błażejewski; An exoskeleton arm optimal configuration determination using inverse kinematics and genetic algorithm.. Acta of Bioengineering and Biomechanics 2019, 21, 45-53, .
- Ali Leylavi Shoushtari; Paolo Dario; Stefano Mazzoleni; A review on the evolvement trend of robotic interaction control. Industrial Robot: An International Journal 2016, 43, 535-551, 10.1108/ir-02-2016-0073.
- S. Hesse; Henning Schmidt; Cordula Werner; Anita Bardeleben; Upper and lower extremity robotic devices for rehabilitation and for studying motor control.. Current Opinion in Neurology 2003, 16, 705–710, 10.1097/01.wco.0000102630.16692.38.
- Morris, M.; A Review of Rehabilitation Strategies for Stroke Recovery. ASME Early Career Tech. Conf. 2015, 11, 24–31, .
- Guo, S.; Gao, J.; Guo, J.; Zhang, W.; Hu, Y. Design of the structural optimization for the upper limb rehabilitation robot. In Proceedings of the 2016 IEEE International Conference on Mechatronics and Automation, Harbin, China, 7–10 August 2016; pp. 1185–1190
- Guowu Wei; Lei Ren; Jian S. Dai; Prehension of an Anthropomorphic Metamorphic Robotic Hand Based on Opposition Space Model. Lecture Notes in Computer Science 2017, 1, 71-83, 10.1007/978-3-319-65289-4_7.
- Hogan, N.; Krebs, H.I.; Charnnarong, J.; Srikrishna, P.; Sharon, A. MIT-MANUS: A Workstation for Manual Therapy and Training I. In Proceedings of the IEEE International Workshop on Robot and Human Communication, Tokyo, Japan, 1–3 September 1992; pp. 161–165.
- Hermano I. Krebs; Laura DiPietro; Shelly Levy-Tzedek; Susan E. Fasoli; Avrielle Rykman-Berland; Johanna Zipse; Jennifer A. Fawcett; Joel Stein; Howard Poizner; Albert C. Lo; et al. A paradigm shift for rehabilitation robotics. IEEE Engineering in Medicine and Biology Magazine 2008, 27, 61-70, 10.1109/memb.2008.919498.
- Peter S. Lum; Charles G. Burgar; Peggy C. Shor; Matra Majmundar; Machiel Van Der Loos; Robot-assisted movement training compared with conventional therapy techniques for the rehabilitation of upper-limb motor function after stroke. Archives of Physical Medicine and Rehabilitation 2002, 83, 952-959, 10.1053/apmr.2001.33101.
- Nef, T.; Mihelj, M.; Colombo, G.; Riener, R. ARMin—Robot for rehabilitation of the upper extremities. In Proceedings of the IEEE International Conference on Robotics and Automation, Orlando, FL, USA, 15–19 May 2006; pp. 3152–3157.
- Giuseppe Turchetti; Nicola Vitiello; Leopoldo Trieste; Stefano Romiti; Elie Geisler; Silvestro Micera; Why Effectiveness of Robot-Mediated Neurorehabilitation Does Not Necessarily Influence Its Adoption. IEEE Reviews in Biomedical Engineering 2014, 7, 143-153, 10.1109/rbme.2014.2300234.
- Peter S Lum; Charles G Burgar; Peggy C Shor; Evidence for Improved Muscle Activation Patterns After Retraining of Reaching Movements with the MIME Robotic System in Subjects with Post-Stroke Hemiparesis. IEEE Transactions on Neural Systems and Rehabilitation Engineering 2004, 12, 186-194, 10.1109/tnsre.2004.827225.
- D J Reinkensmeyer; L E Kahn; M Averbuch; A McKenna-Cole; Brian D. Schmit; W Z Rymer; Understanding and treating arm movement impairment after chronic brain injury: progress with the ARM guide.. Journal of Rehabilitation Research and Development 2001, 37, 653–662, .
- Mihelj, M.; Nef, T.; Riener, R. ARMin II—7 DoF rehabilitation robot: Mechanics and kinematics. In Proceedings of the 2007 IEEE International Conference on Robotics and Automation, Roma, Italy, 10–14 April 2007; pp. 4120–4125.
- Nef, T.; Riener, R. ARMin—Design of a novel arm rehabilitation robot. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 57–60.
- Keller, U.; Schölch, S.; Albisser, U.; Rudhe, C.; Curt, A.; Riener, R.; Klamroth-Marganska, V. Robot-assisted arm assessments in spinal cord injured patients: A consideration of concept study. PLoS ONE 2015, 10, e0126948.
- Joel C. Perry; Jacob Rosen; Stephen Burns; Upper-Limb Powered Exoskeleton Design. IEEE/ASME Transactions on Mechatronics 2007, 12, 408-417, 10.1109/tmech.2007.901934.
- Jawad Hussain; Kenneth Sundaraj; Yin Fen Low; Lam Chee Kiang; Sebastian Sundaraj; Asraf Ali; A systematic review on fatigue analysis in triceps brachii using surface electromyography. Biomedical Signal Processing and Control 2018, 40, 396-414, 10.1016/j.bspc.2017.10.008.
- Stéphanie Dehem; Vincenza Montedoro; Martin Gareth Edwards; Christine Detrembleur; Gaëtan Stoquart; Anne Renders; Sophie Heins; Dehez Bruno; Thierry Lejeune; Development of a robotic upper limb assessment to configure a serious game. NeuroRehabilitation 2019, 44, 263-274, 10.3233/nre-182525.
- A. Frisoli; Massimo Bergamasco; Maria C Carboncini; Bruno Rossi; Robotic assisted rehabilitation in Virtual Reality with the L-EXOS.. Studies in health technology and informatics 2009, 145, 40–54, .
- Housman, S.J.; Le, V.; Rahman, T.; Sanchez, R.J.; Remkensrneyer, D.J. Arm-training with T-WREX after chronic stroke: Preliminary results of a randomized controlled trial. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; pp. 562–568.
- Rehmat, N.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.Q.; Liang, H. Upper Limb Rehabilitation using Robotic Exoskeleton Systems: A Systematic Review. Int. J. Intell. Robot. Appl. 2018, 2, 283–295.
- Gabor Fazekas; Monika Horvath; Tibor Troznai; Andras Toth; Robot-mediated upper limb physiotherapy for patients with spastic hemiparesis: A preliminary study. Journal of Rehabilitation Medicine 2007, 39, 580-582, 10.2340/16501977-0087.
- Toth, A.; Fazekas, G.; Arz, G.; Jurak, M.; Horvath, M. Passive Robotic Movement Therapy of the Spastic Hemiparetic Arm with REHAROB: Report of the First Clinical Test and the Follow-up System Improvement. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 127–130.
- Klein, J.; Spencer, S.J.; Allington, J.; Minakata, K.; Wolbrecht, E.T.; Smith, R.; Bobrow, J.E.; Reinkensmeyer, D.J. Biomimetic orthosis for the neurorehabilitation of the elbow and shoulder (BONES). In Proceedings of the 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 535–541.