Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Hybrid Renewable Energy Sources (HRES) microsystems, like microgrids incorporated with solar panels and battery, is identified to ensure higher and more reliable energy access in rural healthcare centres. At the same time, the adoption of Demand Side Management (DSM) in the HRES deployment in countryside healthcare facilities is reported to decrease the initial cost of installation and improve efficiency.
- energy access
- rural healthcare
- hybrid renewable energy sources
1. Background
Inaccessibility to adequate electricity has proven to be one of the most pressing concerns confronting the world, and this has affected about 1.6 billion people worldwide [1][2]. Given the distance and cost of expanding the grid, most rural areas in developing countries (including Nigeria) have difficulty accessing power. As a result, many rural healthcare facilities have been unable to fulfil their original mission adequately. This electricity inadequacy in most distant villages has widened the infrastructural development, and the economic gap has exacerbated poverty and made raising their standard of living more difficult. Research shows that roughly 17% of the world’s populace cannot access a grid-connected power supply. Of the 17%, 85% of these individuals are living in rural settlements, of which Sub-Sahara Africa has the highest proportion [1][3][4][5][6].
Some elementary services, including clean water, healthcare, internet connectivity, and education, necessitate electricity for productivity [4][7][8][9][10], whereas essential healthcare services in rural areas, including lighting, medical equipment, and heating, suffer from unreliable energy supply. As a result, proper medical diagnosis and treatment are denied; therefore, many people have to find their way to cities for better diagnosis and treatment. Additionally, healthcare workers lost interest in rendering medical services in rural healthcare centres, and those present could not operate for long hours because of inaccessibility to reliable energy [11]. The primary factor for the early closure of some healthcare centres is the lack of access to a quality power supply at night and the shortfall of staffing [5][12].
There is more rural-urban drift in sub-Saharan Africa since less or no concern has been given to rural electrification over time [3][5][13][14]. In many healthcare facilities, energy is required for adequate ventilation, temperature and water control, lighting, and medical equipment operations [11]. To avoid life risks, patients receiving medical care with ventilators or oxygen masks must not suffer from power outages. Poor power supply to rural areas causes the rural health personnel to refer many of their patients to the city for better treatment, as many die during this cause [15][16][17].
There is widespread agreement that healthcare centres will improve productivity if only a sufficient power supply is available [2][18][19][20]. A reliable energy source that will serve 24 h is essential for a healthcare centre to operate on a full scale [5][18]. Insufficient and unreliable electricity is among the significant factors blocking the fulfilment of the United Nations’ Sustainable Development Goals number three (SDG-3) [17]. The primary power source of most rural health centres is generators powered with diesel or gasoline. In contrast, it cannot serve in the long run as fuel costs increase operational expenses [2][15][20]. Apart from the cost of running the generator set, there is the possibility of a health hazard resulting from the emission from the generator [21].
2. Effects of No Access to Reliable Energy Sources in Rural Healthcare Centres
The World Health Organization (WHO) makes it known that good healthcare service directly depends on access to a reliable electricity supply, and saving a life without electricity will be difficult [1][6][12][22][23]. Figure 1 shows the effect of unreliable energy access on rural healthcare services [24].
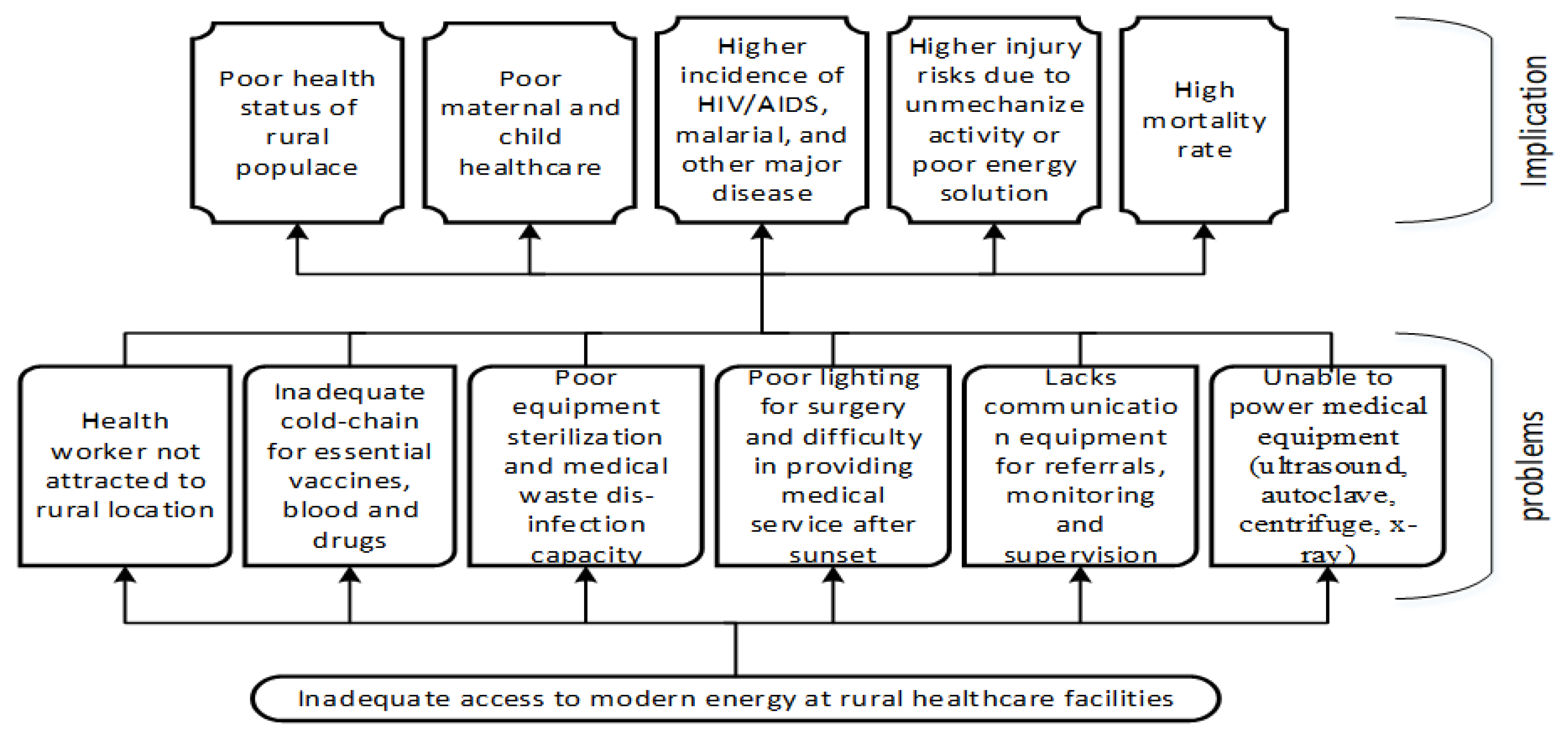
Figure 1. Energy access impacts on rural health care services [24].
The optimal approach to rural accessibility to energy is by using the natural resources available [8][21][25]. In 2014 and 2015, the National Primary Health Care Development Agency (NPHCDA) of Nigeria coordinated the construction of 91 Primary Health Centres (PHCs) across the country at an equal rate. However, most of these PHCs, worth over two billion naira, have been abandoned due to an inaccessible power supply that is reliable [5]. Multiplying the numbers of healthcare infrastructure does not impact healthcare improvement without providing an accessible power supply [22][24]. The cost spent on the inactive healthcare centres will finance the installation of off-grid solar systems for about 667 existing PHCs across the country [5].
Most of these off-grid PHCs illuminate the clinic at night with torchlight, mobile phones, and candles. For instance, a study reported that Dakwa primary healthcare centre, situated in an off-grid community in Abuja, Nigeria, uses kerosene lamps as a means of lighting at night. The midwives and healthcare staffs carry out their night work, including childbirth, using torchlight. There is a report of a midwife whose torchlight went off in the middle of delivery, and the baby was delivered in darkness [5].
3. Significance of Accessing Reliable Electricity in Rural Healthcare Centres
The social advancement of a community is defined by the regular and satisfactory supply of energy [9][10]. However, a reliable energy supply is vital to the healthy functionality of healthcare centres through technological-based medical facilities [11]. Electrification happens to be the basis of achieving standard healthcare administration in rural areas and catching the interest of health personnel for quality services [26]. Access to stable electricity will improve the health personnel’s working rate and attract and motivate more skilled health workers in rural areas, thus enhancing the healthcare status of the locals [17]. However, many barriers challenge planners and policymakers to feed electricity in remote areas [27]. Several findings and research were carried out to make electricity accessible to the off-grid a success [14]. Supreme services such as diagnostics and treatment cannot be offered to patients without electricity. Most medical equipment cannot operate without electricity. A freezer/refrigerator is required to store pharmaceutical items and needs lighting at night for treatment; hence accessibility to energy is essential for exemplary healthcare services [11].
The improvement of one sector affects the other. While the output of a sector, such as energy, serves as input to many others. Therefore, every sector relies on electricity access. For instance, devices such as television, radio, or mobile phones help broadcast health news, especially during the pandemic, and access to electricity thus improves the usage of these devices to serve the expected purpose [11]. Consequently, it is necessary to enhance the living conditions of the workers and their families with facilities such as electricity access, communication, education, and other social development to entice the interest of medical workers in rural areas [10]. Furthermore, energy security catches the interest of health workers, increases facility service hours, and reduces health service expenses [25]. Thus, regular and sustainable electricity supply in healthcare facilities contribute positively to the improvement and success of healthcare [24][28].
In disease management, electricity access is essential for treatment, diagnosis, and refrigeration. A solution to energy accessibility is an immediate deployment of mini-grids for healthcare facilities in rural or urban areas with low power supply [3][11]. Small-scale hydropower may be required via mini-grid/off-grid as energy provision solutions in rural areas. This deployment will serve the healthcare facilities and provide nearby communities with sustainable energy. Small-scale hydropower could be a trusted procedure, but modification is necessary to suit the local situation and grid size [29]. Health centres can achieve high-reliable energy services through microgrids incorporated with solar panels and battery storage. Both healthcare amenities and households in urban or rural areas could benefit from a backup via solar panels and a battery storage system microgrid. Hence, danger due to power outages could be overcome as renewable backup is feasible and cost-effective in rural areas [11][15].
Furthermore, a renewable energy microsystem is a tool for producing, storing, and providing electricity that depends on renewable energy and is separated from any distribution system. Without technical maintenance to the solar PV, components will be broken down, and the system may stop working [30]. Therefore, the beneficiary can be trained on preventive and corrective maintenance of the system. The preliminary instruction given to the user will help them perform elementary maintenance, such as periodically adding distilled water to the battery.
The Service Accessibility and Readiness Assessment tool of the World Health Organisation (WHO) has identified energy accessibility as a necessity for good healthcare services and facilities. It further emphasises the importance of energy accessibility for primary applications such as lighting, refrigeration, sterilisation, ventilation, internet communication, and computer operation [25]. Additionally, functionality of equipment such as oxygen aspirators, microscopes, and electrocardiograms require dependable electricity [31].
Despite all the advantages derived from energy accessibility, there is difficulty in expanding energy in rural communities. The barriers include a lack of finance, inadequate planning, lack of community contribution, and no maintenance [25]. The cold chain of the vaccine relies totally on the availability of sustainable power. Little change in vaccine temperature renders the vaccine impotent [32]. Therefore, national immunisation programs will be successfully carried out in rural areas when reliable electricity is available. A stable electricity supply can enhance healthcare-related services like health broadcasts (sensitisation against infectious diseases) and maternal and neonatal health administration, improving society’s health conditions in rural communities. Health-related news is easily accessed in rural areas through radio and television, especially for illiterate people, compared with newspapers, magazines, or any other printed information source [12]. Since access to electricity can practically improve the healthcare status and orientation of the rural populace, alternative energy systems must be developed to achieve this goal.
4. Rural Healthcare Centre Power Supply Alternative the Off-Grid Renewable Energy Systems
The extension of the electric grid to the local area is quite tricky due to the distance and cost of distribution; hence it is more convenient to utilise renewable resources or fossil fuel-based energy generation in a remote area. Moreover, renewable energy resources are the best alternative to electrifying rural healthcare centres [14]. Initially, renewable energy was categorised as peculiar innovation but is now seen as a priority energy source due to its incitement and funding rate making it easier to acquire [33].
Solar PV and wind turbine has become reasonable option economically with technological advancement; as a result, it is more appreciable for off-grid application [34], whereas sun intensity and wind speed are the base factors that define the utilisation of PV solar and wind turbine, respectively. Stand-alone and mini-grids are off-grid energy systems that outstand conventional fuels and cost-effective alternatives to increase electricity accessibility [26]. More than 60% of new electricity access will be powered by 2030 through renewable energy sources. About half of the provision will be made with standalone and mini-grid systems [26]. Energy access emanating for photovoltaic sources has tremendously given rural service a leeway in sub-Sahara Africa in line with SDG mandate. This was demonstrated during the COVID-19 pandemic where much pressure was mounted on rural health facilities [35]. Solar PV produces clean energy at an affordable cost on a small scale as the principal installation budget comprises the facilities’ expenses to use the power with low or zero operating costs.
The local council owns most rural healthcare centres; therefore, the local government is expected to regulate the Hybrid Renewable Energy System (HRES) used in healthcare centres to power health facilities. At the same time, the local council budget is insufficient to provide the required maintenance of HRES. Provision for funds to maintain HRES can be secured through public-private-partnership to prevent the early breakdown of the system. Similarly, educating the staff properly on usage and the maintenance of the HRES can reduce the maintenance cost of the system, which could be done while installing the system. In addition, this training will aid energy availability for emergency or crucial medical equipment at any time [15].
Off-grid renewable energy solutions have become an option for making electricity accessible to off-grid areas due to their cost affordability and a swift decrease in technology costs [26]. Countries such as Nepal have constructed micro-hydro projects to boost the socio-economy and replace off-grid diesel generators with renewable energy or hybridised due to large possible demand [26]. With the implementation of smart devices developed from artificial intelligence and internet of things technologies, there is a chance of combining solar and wind in energy production. The electricity needs in rural healthcare centres can be grouped into (i) health personnel and facility lighting, (ii) power for special operations and essential equipment, and (iii) security lighting. African Solar Designs’ need assessments discovered that off-grid energy structures, specifically the Solar PV system, supply vital energy, although inadequate for the groups of electricity needed [27]. They also discovered that there are abandoned solar PV systems in many rural healthcare centres that are not functioning due to a deficiency in PV system management. The principal factors causing the drawback were poor system operation, lack of funds for system maintenance, and lack of community intervention [13][27]. Core United Nations (UN) allied agencies acquired PV solar-powered refrigerators for cold chain conservation [5], thus improving the child immunisation program since the cold storage device is critical to keep the vaccine at the required temperature [12].
Solar PV home systems comprise a charge controller, a PV module, an inverter, and a battery connected to generate a direct current that charges the battery via the charge controller and power dc appliances. Additionally, Alternating Currents (AC) loads can be powered by the inverter [23]. Using an energy storage device in the system enhances the utilisation of the renewable energy system and reduces the need for a generator set. Eventually, the amount of fuel consumption reduces. Solar PV and wind turbines generate energy at a peak level consumed during the day; the rest of the energy stored enables power availability when solar and wind cannot supply. Lithium-ion batteries in rural areas’ energy storage tools contribute to the storage of energy at a very high rate when charging, and there is less loss in the circuit during discharging of the battery. A hybrid storage unit consisting of lead-acid and lithium-ion batteries can supply maximum load demand. The setup is advantageous as the lead-acid battery charging is standardised and thus elongates the battery life span and prevents early spoilage of the battery. The Lithium-ion battery can sense a quick rise in demand and thereby ease lead-acid accumulator by carrying the peak load demand.
The environmental benefit derived from using wind, solar, or hybrid power systems, including solar and wind, is no production of harmful emissions. Moreover, a hybrid system with diesel generators is also characterised by low atmospheric emissions of greenhouse gases. However, the noise generated from turbine blades and land space occupied by constructed systems of wind or solar contributes negatively to the environment, as the land cannot be used for another purpose. Thus, it is recommended to use existing rooftops to install solar panels and locate the wind site away from residential areas, health clinics, or school environments [18][23].
Switching to the renewable energy alternative as a means of power supply in rural areas contributes to the duration of the operation in rural healthcare centres. Therefore, getting access to a reliable power supply will increase the opening hours of the off-grid rural healthcare since the health workers can get the facilities powered for operation both day and night. In addition, the cost of securing fuel reduces as the need for fuel purchase reduces. Additionally, there is a high chance of gaining access to digital medical facilities, improving the health care service, and thus ending the cause of referring patients to another clinic. In contrast, government policy has not risen to support renewable energy technology, which challenges regulations for marketing renewable energy systems and the presence of standard equipment [36].
Additionally, a recent study demonstrated the economic and technical feasibility of hybrid renewable energy systems, indicating the cost-effectiveness of Solar PV/Wind/DG/Battery that achieved CO2 emission reduction and reliable power supply to make a case for renewables [37]. In the typical off-grid Hybrid Renewable Energy System (HRES) shown in Figure 2, the battery provided is considered for storing excess energy via a converter attached to the system. The converter provides ports for AC and DC output loads since it can receive AC and DC power as input.
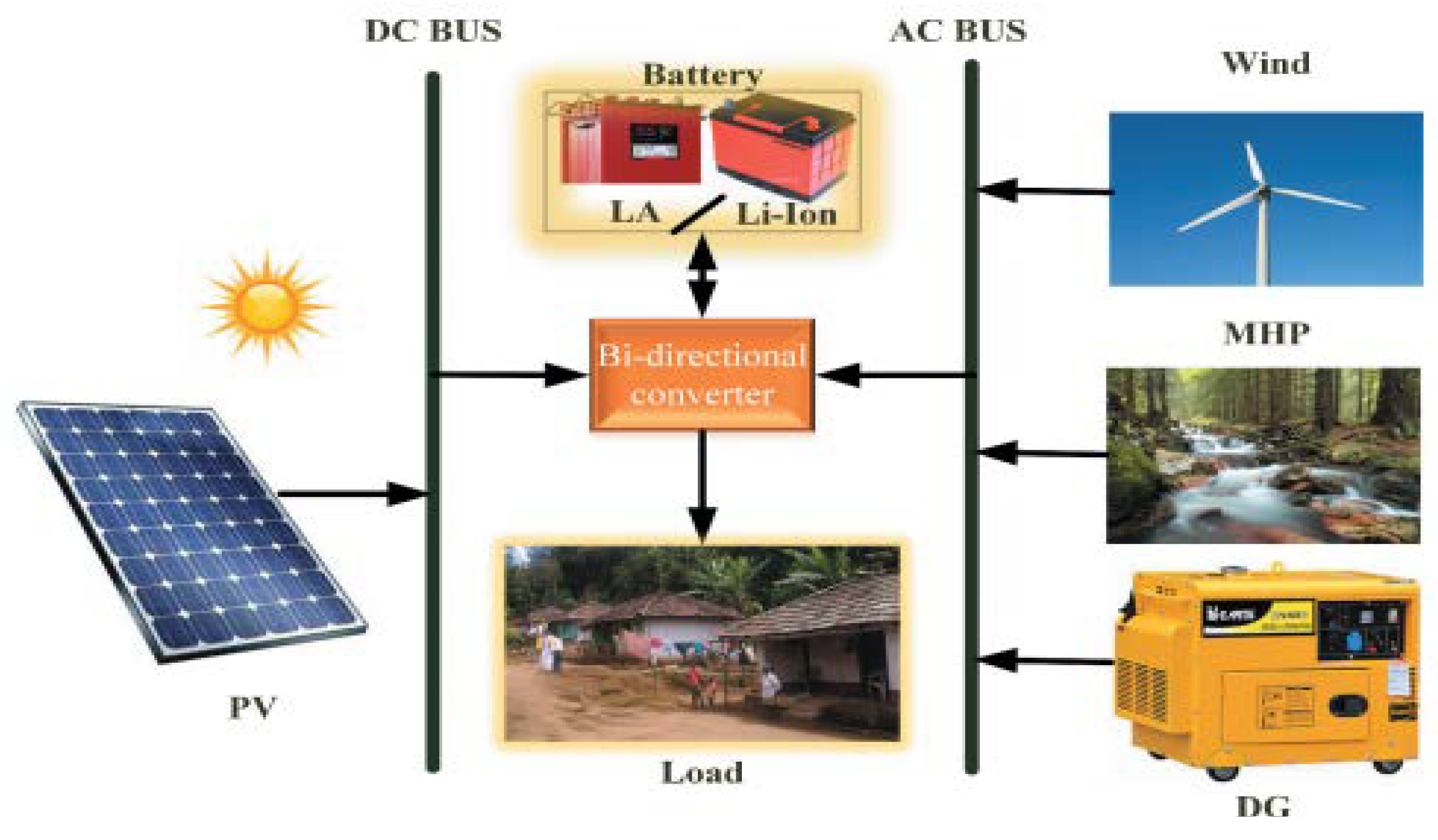
Figure 2. HRES schematic diagram.
This entry is adapted from the peer-reviewed paper 10.3390/en15249554
References
- Franco, A.; Shaker, M.; Kalubi, D.; Hostettler, S. A review of sustainable energy access and technologies for healthcare facilities in the Global South. Sustain. Energy Technol. Assess. 2017, 22, 92–105.
- Oladigbolu, J.O.; Al-Turki, Y.A.; Olatomiwa, L. Comparative study and sensitivity analysis of a standalone hybrid energy system for electrification of rural healthcare facility in Nigeria. Alex. Eng. J. 2021, 60, 5547–5565.
- Adair-Rohani, H.; Zukor, K.; Bonjour, S.; Wilburn, S.; Kuesel, A.C.; Hebert, R.; Fletcher, E.R. Limited electricity access in health facilities of sub-Saharan Africa: A systematic review of data on electricity access, sources, and reliability. Glob. Health Sci. Pract. 2013, 1, 249–261.
- Akinyele, D.O.; Rayudu, R.K. Community-based hybrid electricity supply system: A practical and comparative approach. Appl. Energy 2016, 171, 608–628.
- Ikenna, D.; Salman, T.; Okoye, T.T. Improving Access to Clean Reliable Energy for Primary Health Care Centres in Nigeria: Situation Analysis of PHCs in the Federal Capital Territory. In Heinrich Boell Stiftung Nigeria; Heinrich Boell Stiftung Nigeria: Abuja, Nigeria, 2018.
- Olatomiwa, L.; Blanchard, R.E.; Mekhilef, S.; Akinyele, D. Hybrid renewable energy supply for rural healthcare facilities: An approach to quality healthcare delivery. Sustain. Energy Technol. Assess. 2018, 30, 121–138.
- Akinyele, D.O.; Nair, N.K.C.; Rayudu, R.K.; Chakrabarti, B. Decentralised energy generation for end-use applications: Economic, social and environmental benefits assessment. In Proceedings of the IEEE Innovative Smart Grid Technologies Asia (ISGT ASIA), Kuala Lumpur, Malaysia, 20–23 May 2014; pp. 84–89.
- Energypedia. Access to Modern Energy and the Impact on Health. 2018. Available online: https://energypedia.info/wiki/Access_to_modern_energy_and_the_impact_on_health (accessed on 23 June 2022).
- Uzoma, C.C.; Amadi, K.C. Energy access: A key to rural development in Nigeria. J. Soc. Sci. 2019, 5, 452–456.
- Welland, A. Electrification of Health Clinics in Rural Areas: Challenges and Opportunities; CMEDT-Smart Villages Initiative, c/o Trinity College: Cambridge, UK, 2017.
- Aemro, Y.B.; Moura, P.; De Almeida, A.T. Energy access during and post-COVID-19 pandemic in sub-Saharan countries: The case of Ethiopia. In Environment, Development and Sustainability; Springer: Berlin/Heidelberg, Germany, 2022; pp. 1–22.
- Chen, Y.J.; Chindarkar, N.; Xiao, Y. Effect of reliable electricity on health facilities, health information, and child and maternal health services utilisation: Evidence from rural Gujarat, India. J. Health Popul. Nutr. 2019, 38, 1–16.
- Kaygusuz, K. Energy services and energy poverty for sustainable rural development. Renew. Sustain. Energy Rev. 2011, 15, 936–947.
- Rabetanetiarimanana, J.C.I.; Radanielina, M.H.; Rakotondramiarana, H.T. PV-Hybrid Off-Grid and Mini-Grid Systems for Rural Electrification in Sub-Saharan Africa. Smart Grid Renew. Energy 2018, 9, 171.
- Babatunde, O.M.; Adedoja, O.S.; Babatunde, D.E.; Denwigwe, I.H. Off-grid hybrid renewable energy system for rural healthcare centers: A case study in Nigeria. Energy Sci. Eng. 2019, 7, 676–693.
- Kolhe, M.L.; Ranaweera, K.I.U.; Gunawardana, A.S. Techno-economic sizing of off-grid hybrid renewable energy system for rural electrification in Sri Lanka. Sustain. Energy Technol. Assess. 2015, 11, 53–64.
- Moner-Girona, M.; Kakoulaki, G.; Falchetta, G.; Weiss, D.J.; Taylor, N. Achieving universal electrification of rural healthcare facilities in sub-Saharan Africa with decentralised renewable energy technologies. Joule 2021, 5, 2687–2714.
- Akinyele, D.O.; Rayudu, R.K. Strategy for developing energy systems for remote communities: Insights to best practices and sustainability. Sustain. Energy Technol. Assess. 2016, 16, 106–127.
- Ohunakin, O.S.; Adaramola, M.S.; Oyewola, O.M.; Fagbenle, R.O. Solar energy applications and development in Nigeria: Drivers and barriers. Renew. Sustain. Energy Rev. 2014, 32, 294–301.
- Olatomiwa, L.; Mekhilef, S.; Huda, A.S.N.; Ohunakin, O.S. Economic evaluation of hybrid energy systems for rural electrification in six geopolitical zones of Nigeria. Renew. Energy 2015, 83, 435–446.
- Chowdhury, T.; Chowdhury, H.; Hasan, S.; Rahman, M.S.; Bhuiya, M.; Chowdhury, P. Design of a standalone energy hybrid system for a makeshift health care center: A case study. J. Build. Eng. 2021, 40, 102346.
- Akinyele, D.; Rayudu, R.; Blanchard, R.E. Sustainable Microgrids for Energy-Poor Communities: A Spotlight on the Planning Dimensions; IEEE: Piscataway, NJ, USA, 2016.
- Asian Development Bank. Improving Lives of Rural Communities Through Developing Small Hybrid Renewable Energy Systems; Asian Development Bank: Mandaluyong, Philippines, 2017.
- Olatomiwa, L.; Mekhilef, S.; Ohunakin, O.S. Hybrid renewable power supply for rural health clinics (RHC) in six geo-political zones of Nigeria. Sustain. Energy Technol. Assess. 2016, 13, 1–12.
- Ighravwe, D.E.; Babatunde, M.O. Determination of a suitable renewable energy source for mini-grid business: A risk-based multicriteria approach. J. Renew. Energy 2018, 2018, 2163262.
- Irena, R.E.S. Renewable Energy Target Setting; International Renewable Energy Agency: Abu Dhabi, United Arab Emirates, 2015.
- Javadi, D.; Ssempebwa, J.; Isunju, J.B.; Yevoo, L.; Amu, A.; Nabiwemba, E.; Severi, L. Implementation research on sustainable electrification of rural primary care facilities in Ghana and Uganda. Health Policy Plan. 2020, 35, 124–136.
- Olatomiwa, L. Optimal configuration assessments of hybrid renewable power supply for rural healthcare facilities. Energy Rep. 2016, 2, 141–146.
- Uamusse, M.M.; Tussupova, K.; Persson, K.M.; Bengtsson, L.; Berndtsson, R.; Zobaa, A. Access to sustainable electrification: Possibilities for rural Mozambique. Cogent Eng. 2020, 7, 1765688.
- Dávalos, A.; De Jesús Gil Herrera, R.; Colmenares, R.F.A. Comprehensive solution approach to the sustainability problem of photovoltaic systems: The Bolivian case. Cogent Eng. 2019, 6, 1691314.
- Maggio, G.; Squadrito, G.; Nicita, A. Hydrogen and medical oxygen by renewable energy based electrolysis: A green and economically viable route. Appl. Energy 2022, 306, 117993.
- Olsen, K.; Jimenez, A. Renewable Energy for Rural Health Clinics; National Renewable Energy Laboratory Publishing: Golden, CO, USA, 1998.
- Akinyele, D.; Olatomiwa, L.; Ighravwe, D.E.; Babatunde, M.O.; Monyei, C.; Aikhuele, D. Optimal planning and electricity sharing strategy of hybrid energy system for remote communities in Nigeria. Sci. Afr. 2020, 10, e00589.
- Salisu, S.; Mustafa, M.W.; Olatomiwa, L.; Mohammed, O.O. Assessment of technical and economic feasibility for a hybrid PV-wind-diesel-battery energy system in a remote community of north-central Nigeria. Alex. Eng. J. 2019, 58, 1103–1118.
- Pittalis, M.; Kyriakarakos, G.; Moner-Girona, M. The role of photovoltaics in Clean Energy Access Business Models for Social Infrastructure in Sub-Saharan Africa—Existing Models and Emerging Trends. In Encyclopedia of Sustainability Science and Technology Second Edition; Springer: Berlin/Heidelberg, Germany, 2021.
- Watson, J.; Johnson, O. Renewable Energy Technologies for Rural Development. 2010. Available online: https://policycommons.net/artifacts/100912/renewable-energy-technologies-for-rural-development/ (accessed on 23 June 2022).
- Ramesh, M.; Saini, R.P. Demand Side Management based techno-economic performance analysis for a standalone hybrid renewable energy system of India. Energy Sources Part A Recovery Util. Environ. Eff. 2021, 43, 1–29.
This entry is offline, you can click here to edit this entry!