The safety data on COVID-19 vaccines seems reassuring, and there is no way to deny the value of this immunization in view of its importance in reducing severe forms of COVID-19 infections. The cases of endocrinopathies reported to these vaccines are only scattered cases whose meeting is done gradually. Unlike thyroid or pancreatic impairment, pituitary damage is much rarer and plausibly underdiagnosed. This is mainly due to the entanglement of its symptoms with those of post-vaccination flu syndrome or those of a potential long Covid. Damage in the pituitary gland can be due either to hypophysitis or to pituitary apoplexy. The physiopathology, however, does not seem to differ enormously since it involves the ASIA syndrome which can be a consequence of the involvement of either the adjuvants or the Spike S proteins. The hypothesis of the VITT syndrome is also mentioned in the case of pituitary apoplexy.
- COVID-19
- Hypophysitis
- Apoplexy
- Diabetes insipidus
A large spectrum of endocrine dysfunctions was reported in literature involving the thyroid gland, pancreatic islets, the pituitary and the adrenal gland . So far, many reviews have focused on the analysis of thyroid or pancreatic disorders [1]. The cases of pituitary disorders are not very numerous, but we strongly believe that they are underestimated given the intricacy of the clinical symptoms with features of COVID-19 itself. Pituitary disorders were more common among women. The two most preponderant disorders that we collected were hypophysitis and pituitary apoplexy. Their clinical presentation was slightly different, but they mainly diverged on pathophysiological aspects. The mechanisms that explain the adverse effects of COVID-19 vaccine on the pituitary gland are explained in the figures below.
Among pathophysiological mechanisms of post-vaccine hypophysitis, autoimmune and inflammatory syndromes induced by vaccine adjuvants (ASIA) were the most cited.
Adjuvants, are substances used to enhance the magnitude and durability of the immune response, which makes them an undeniable asset in vaccines ‘upgrading processes. In genetically susceptible subjects; exposure to adjuvants may, on rare occasions, set off polygenic auto-immune diseases. The immune disruption in such cases is attributed mainly to molecular mimicry, which triggers polyclonal activation of B lymphocytes. Reviewed data on adjuvants used in COVID-19 vaccines showed that components such as aluminum salts, emulsions, oils, toll-like receptors, AS01B, four lipids of the mRNA vaccine and polyethylene glycol might generate an immune response in susceptible individuals (figure 1).
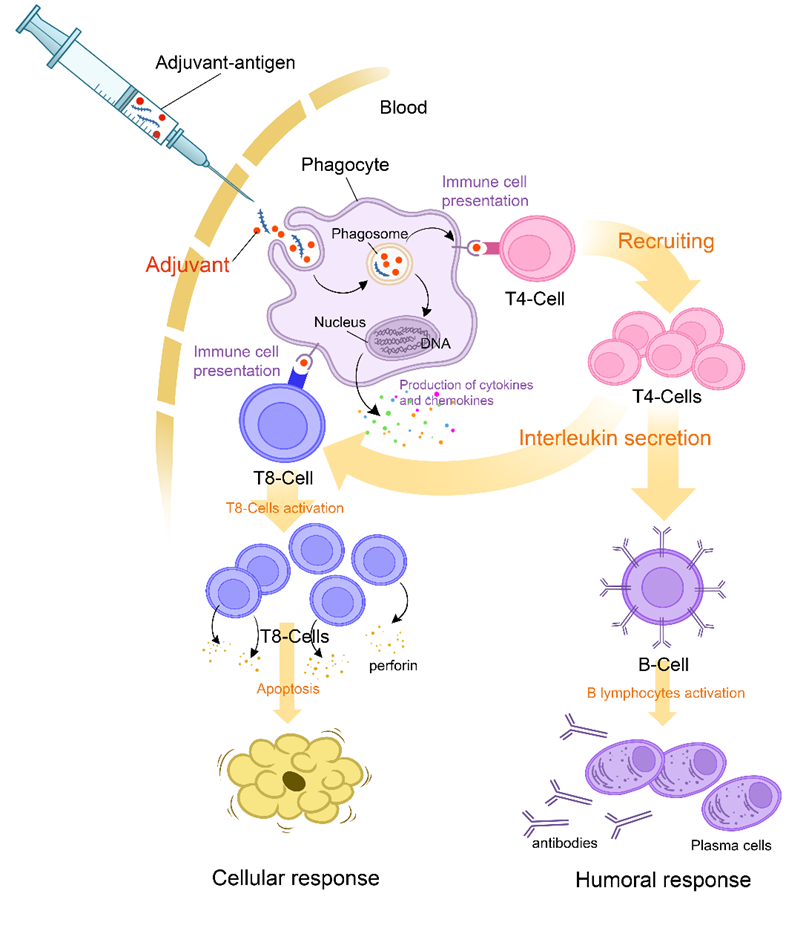
Figure 1. Mechanism of action of Adjuvants and initial triggers explaining pathophysiology of ASIA syndrome following Covid-19 vaccine.
Another pathophysiological mechanism arises implying immune system hyper-stimulation and molecular mimicry of the vaccine components. Interestingly, SARS-CoV-2 proteins (from its spike, nucleus and membrane) present sequence similitude with some peptides in endocrine tissues such as the peroxidase in the thyroid gland. Autoimmune inflammation results therefore from a cross-recognition between the modified SARS-CoV-2 proteins in vaccines and the human target protein. In the majority of cases, symptoms of hypophysitis -attesting of auto-immune activation- appear few days after vaccination. The concentration of viral proteins, peaking synchronously could be the underlying reason. In fact, the vaccine-encoded antigen (S protein) is stabilized in its perfusion form in the mRNA vaccines. It spreads systemically through circulation and could contribute therefore to the triggering of autoimmune diseases in susceptible individuals.
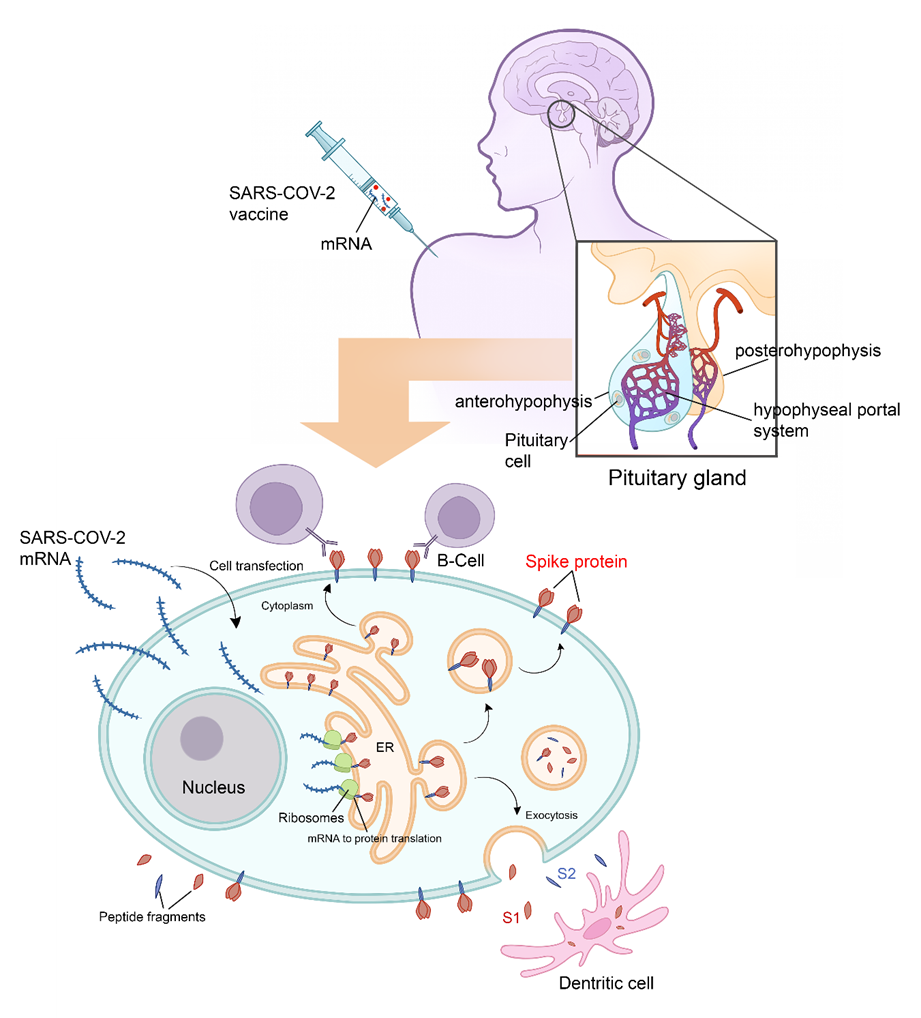
Figure 2. Physiology of pituitary cell protein’s expression and Vaccine induced hypophysitis pathophysiology. Following adjuvant internalization and mRNA release, the viral signal peptide drives antigen production in the endoplasmic reticulum (ER). After sorting in the Golgi network, S protein acquires its final position in the human cell membrane, where S1 is exposed to the extracellular space. Antigen sorting and trafficking may also induce the release of S protein-containing exosomes. Also shown are dendritic cells (professional antigen-presenting cells) engulfing circulating antigens, and antibody-mediated binding of B cells to cell-anchored antigens. All the above mentioned mechanisms potentiate the inflammatory mechanisms. All the Endocrine consequences after hypophysitis are mainly hypogonadism, hypothyroidism, hypoadrenalism and diabetes insipidus.
Following large vaccine campaigns, there was mounting evidence of serious adverse effects related to this vaccine, including thrombosis and bleeding. This syndrome has been termed ”Vaccine-Induced Thrombotic Thrombocytopenia” (VITT). It occurred more frequently in young women and was imputed only to viral vector vaccines. VITT seems to be a phenomenon similar to heparin-induced thrombocytopenia and appears to have an autoimmune provenance. Currently, the association of five criteria is used to define VITT, which are: recent vaccination, thrombosis, thrombocytopenia, elevated D-dimer levels, and positivity of anti-PF4 antibodies (figure 3)
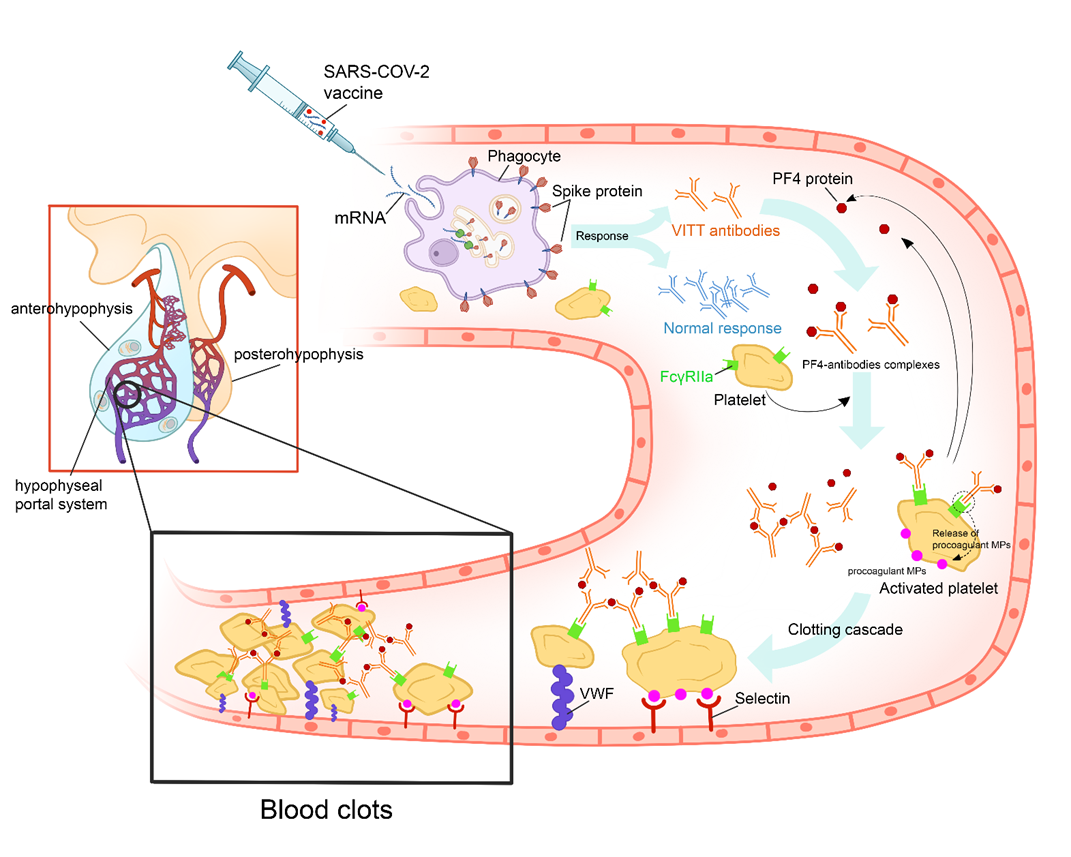
Figure 3. Proposed figure showing the cascade of pathogenic events that could favor the onset of the vaccine-induced immune thrombotic thrombocytopenia in individuals vaccinated with anti-COVID-19 vaccines.
After the administration of the vaccine, the recipient’s cells produce harmless COVID-19 proteins and the immune system responds by producing protective antibodies. In some cases, the vaccine’s adjuvants and Spike proteins trigger a type I interferon response and the production of VITT antibodies. VITT is caused by antibodies that PF4 bound to platelets. These antibodies are IgGs that activate platelets via low affinity platelet FcγRIIa receptors (receptors on the platelet surface that bind the Fc portion of IgG). Anti-PF4 antibodies cause cellular activation that, besides activating platelets and coagulation reactions, the antibodies activate monocytes, neutrophils, and endothelial cells (leading to tissue factor expression). Activation of these other cell types further contributes to high thrombosis risk accelerated by other factors among them VWF and procoagulant MP. All these mechanisms will lead to pituitary apoplexy. (PF4: platelet factor 4; IgG: immunoglobulin G; VITT: vaccine-induced immune thrombotic thrombocytopenia; VWF: Van Willebrand Factor; MP: microparticles).
The safety data on COVID-19 vaccines seems reassuring, and there is no way to deny the value of this immunization in view of its importance in reducing severe forms of COVID-19 infections. The cases of endocrinopathies reported to these vaccines are only scattered cases whose meeting is done gradually. Unlike thyroid or pancreatic impairment, pituitary damage is much rarer and plausibly underdiagnosed. This is mainly due to the entanglement of its symptoms with those of post-vaccination flu syndrome or those of a potential long Covid. Damage in the pituitary gland can be due either to hypophysitis or to pituitary apoplexy. The physiopathology, however, does not seem to differ enormously since it involves the ASIA syndrome which can be a consequence of the involvement of either the adjuvants or the Spike S proteins. The hypothesis of the VITT syndrome is also mentioned in the case of pituitary apoplexy. With that said, it is important for clinicians to know the main symptoms evoking these disorders. These features include retro orbital headaches with visual blurring, polyuro-polydipsic syndrome (in posterior pituitary dysfunction) and deterioration in general state with great asthenia (in case of corticotroph damage). Both corticotroph damage and diabetes insipidus can be life threatening and should alarm practitioners. Presence of these symptoms in the immediate post-vaccination period, must urge the need of the clinician to explore hormonal axis in search for pituitary deficits, which should be urgently and accordingly treated.
References
- Ach T, Kammoun F, Fekih HE, et al. Central diabetes insipidus revealing a hypophysitis induced by SARS-CoV-2 vaccine [published online ahead of print, 2022 Oct 6]. Therapie. 2022;S0040-5957(22)00167-6. doi:10.1016/j.therap.2022.09.007