Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Defining dyslexia has still not reached a consensus. This uncertainty may explain why only one of the seven definitions proved satisfactory according to the four-level model. Today, dyslexia is a term that is commonly known and denotes an innate disposition leading to reading and/or writing difficulties. Medicine, linguistics, psychology, pedagogics, social sciences have been involved in assessing dyslexia from different angles.
- dyslexia
- definitions
- cognitive level
1. Introduction
As the art of reading became widespread and common, the condition “word blindness” was also observed and described at the end of the 19th century by medical doctors. The condition was characterized as dramatic because the distance between the writing skills on the one hand and the intellectual abilities on the other was great. The doctors related these weak skills to language functions localized in the angular gyrus in the left hemisphere of the brain [1][2][3].
The American medical doctor Samuel Torrey Orton (1879–1948) called the difficulties “strephosymbolia”, which means “twisted symbols” [4]. He had observed that many of the children he worked with tended to reverse the letters or read and write them in the wrong order. In his research, he eventually focused on language difficulties, studying over three thousand children and adults with such difficulties. This led to a theory that the children’s reading difficulties could be explained by the fact that the left hemisphere of the brain did not become dominant in relation to the right hemisphere of the brain. He also pointed out that the difficulties were familial.
Based on this, Orton wanted to develop a way to learn to read and write as integrated right- and left-brain functions. He started a school based on this idea, which consisted of “multisensory” training. This is a combination of kinesthetic (motion-based) and tactile (touch or sensory) learning strategies integrated with the learning of visual and auditory concepts [5].
Right up until the 1960s, children who did not learn to read and write as expected were seen as single cases, either as developmentally disabled or as non-educationally skilled. Some were taken under the protective wings of concerned teachers who saw these children and gave them extra instruction, often after the end of the school day.
2. 1950–1970
2.1. From Medicine to Educational Psychology Approach
Eventually, dyslexia was studied not only by doctors but also by psychologists, sociologists, and pedagogues. This led to a conflict of competence between researchers and clinicians who evoked new theories about the symptoms and causes of dyslexia. The backdrop to what occurred was the so-called “cognitive revolution”—a reaction to behaviorism, which emphasized that psychological science could only base itself on observable factors. Fundamental to the cognitive revolution was the idea that human activities are complex processes that require organization and planning. Noam Chomsky developed the theory of universal grammar in the 1950s [6]; Jean Piaget developed his well-known theories about the cognitive development of the child through stages [7]; Lev Vygotskij pointed out the importance of culture to the child’s development [8]; and George Miller launched his theories on information processing [9]. This led clinicians, sociologists, and educators to discuss how the environment through pedagogical methods could affect the dyslexic pupil’s skills and difficulties. In 1968, the World Federation of Neurology (WFN) defined dyslexia as follows:
This definition has been criticized as being “an exclusion definition”, which refers to the fact that, for example, underprivileged people or people with low IQ could be excluded from being able to receive a dyslexia diagnosis. Despite this criticism, the definition has been used as a criterion for subject selection, especially in medically oriented research. In a research context, this serves a purpose of avoiding cluttering comorbidities, but in clinical work, the consequences have been more debatable.
Wechsler’s intelligence tests, published in the period 1949 to 1967, are probably the tests that have been most commonly used to map cognitive profiles in both clinical and research settings. The typical dyslexic IQ profile has been presented as low scores in the following four subtests: Arithmetic, Coding, Information, and Digit pan, abbreviated to the so-called ACID profile. Thus, the researchers would naturally look for an ACID profile when investigating possible dyslexia, compatible with the WNF’s definition. In practice, this meant that people with an IQ score lower than 85 points, which includes 17% of the population, could not be diagnosed with dyslexia. For an overview of the tests, please see Frank [12].
2.2. Groupings by Function Analysis
In the 1960s, Johnson and Myklebust focused on children who had problems with information processing, which could inhibit comprehension, speech, reading, mathematical or logical reasoning [13]. The difficulties observed in reading and writing were categorized. Visual dyslexia characterized the difficulties of those who were unable to learn words as a whole or had difficulties with visual discrimination. Difficulties in reversing words or letters while reading or writing were a typical symptom of this group. Auditory dyslexia characterized the difficulties of those who failed to synthesize the phonemes they heard into a visual component like a letter or a word.
Later, Boder extended this grouping to three different types of dyslexia. Dysphonetic dyslexia reflects deficits in associating symbols with sounds [14]. Typical reading errors would include letters being omitted, or the meaning of the word being distorted, and typical misspellings would be of a sound nature, e.g., the /t/ and /g/ being pre-exchanged. Dyseidetic dyslexia reflects a deficit in the ability to perceive letters and whole words as configurations, or visual gestalts, but not difficulties with the auditory processing. Mixed dysphonetic–dyseidetic dyslexia is a combination of both types of difficulties and difficulties in perceiving letters and words as visual gestalts.
3. 1970–2000
3.1. Deficits within the Phonological System
A turning point in the view of subgroups of dyslexia came with research, which refuted that dyslexia could be explained by difficulties in remembering sequences of visual symbols—so-called visual dyslexia [15][16][17]. Instead, Vellutino pointed out that much research supports the theories that dyslexia (reading disability) is due to either difficulties with one or more aspects of linguistic functions or specific difficulties with visual/verbal integration. This represented the beginning of the explanation model, which has been dominating for a long time, namely that dyslexia is closely related to a difficulty in processing linguistic elements. By testing phonological awareness, rapid phonological retrieval, and phonetic transcoding in working memory, Snowling and Hulme found that people with dyslexia had special difficulties with what was collectively referred to as phonological processing [18]. Phonological awareness (PA) is defined as a conscious access to the sound components of the spoken language and the ability to manipulate these sounds. Phonological awareness is a metalinguistic skill that requires conscious attention and reflection on linguistic structures. Phonological awareness is therefore associated with other skills, such as general cognitive abilities, verbal short-term memory, and perception of speech [19].
The linguistic approach to dyslexia contributed to questioning the validity of the discrepancy criteria from the 1970s and 1980s. The Connecticut Longitudinal Study identified a representative sample of 445 preschool children and followed them for many years. An important finding was that children aged 6 to 18, who either had a discrepancy between IQ and reading scores or no such discrete but low reading scores, showed no difference in reading development compared to a control group [20].
3.2. Dyslexia and Access to Lexicon: The Theory of the Double Deficit
A combination of difficulties within the phonological system, which is shown both by misproduction and difficulty with rapid automatized naming (RAN), has proven to be characteristic of people with major dyslexic difficulties, regardless of the linguistic affiliation. According to some research, these two components appear to be independent of each other. RAN is a skill composed of several factors, such as attention, perception, concept formation, memory, phonology, semantics, and motor skills. Difficulties with RAN are related to reading difficulties in several ways. One explanation is that deviations in the magnocellular system will lead to slower processing of visual stimuli, which in turn will lead to slower identification of letters. Another explanation is that RAN deficits can be an indication of a general dysfunction when it comes to processing in visual, auditive, and motor domains, in addition to the orthographic and phonological processing systems. When difficulties with PA and RAN are both present, the dyslectic impairments seem more pervasive and severe [21].
3.3. Neuroanatomical Aspects
Deviant Hemispheric Dominance of Language
Again, dyslexia attributed to deviant laterality in terms of the hemispheric dominance of language was in focus. The theories whereby elevated testosterone content in the mother during pregnancy affects the pattern of brain asymmetry received much attention [22][23][24][25]. The theories were seen as controversial but became a source of inspiration for looking at dyslexia in new ways. In the 1990s, new techniques were adopted in brain research, such as electrophysiological measurements (EEG) and brain scans (MRI). This allowed one to “see” depictions of the brain structure and function under given conditions.
These theories were, to some extent, exploited educationally. The balance model of dyslexia describes the relationship between reading and the function of the two brain hemispheres [26]. Beginner reading is primarily controlled from the right hemisphere of the brain but shifts to the left half of the brain as the child learns to read. In some children, this shift does not occur, and they develop a type of dyslexia in which they continue to rely on a right-hemispheric visuo-perceptual analysis of writing (P-type dyslexia). In other children, the shift over to the left hemisphere occurs prematurely, and they develop a type of dyslexia in which the visual recognition of writing is not sufficiently automated (L-type dyslexia). These different types of dyslexia must have different training programs, which are called hemisphere-specific stimulation [27].
The Hypothesis of Deviations in the Cerebellum
If reading and writing are to become functional, the skills must be automatized. The cerebellum is involved in the coordination of motor skills, balance, and muscle tone, but it is also involved in the automation of motor skills and in adapting the control of learning. According to Fawcett and Nicolson, cerebellum damage has led to difficulties with attention and working memory and with dyslexic symptoms when reading [28].
The Theory of Deviant Temporal Processing
Temporal processing implies the time spent to perceive, interpret, and produce sequential visual or auditory stimuli. Language is produced in sequences, and reading and writing are also activities that require similar temporal processing.
According to Tallal’s theories of auditory processing, the ability to distinguish different sounds in a fast tempo is a crucial linguistic building block [29][30]. A brain that does not distinguish quickly enough does not have the ability to distinguish between language sounds, which is a prerequisite for a child to learn to read. Hence, deviations in one or more of these processing skills can cause reading to degrade [31][32].
Additionally, deviations in the transient visual system, which reveals movements and changes in figures, is considered important for transmitting what one sees peripherally when reading [33]. The hypothesis of deviations in the magnocellular system comes from observations made by people with dyslexia who say that letters seem to move around or lie over each other [34].
New Definitions
The notion of the relationship between language and dyslexia showed that phonological problems were a common feature in people with reading/writing difficulties, regardless of the IQ goals [35][36]. An interesting and important debate regarding dyslexia began in the mid-1990s with a definition of dyslexia proposed by The Orton Dyslexia Society Research Committee in 1994:
“Dyslexia is one of several distinct learning disabilities. It is a specific language-based disorder of constitutional origin characterized by difficulties in single word decoding, usually reflecting insufficient phonological processing. These difficulties in single word decoding are often unexpected in relation to age and other cognitive and academic abilities; they are not the result of generalized developmental disability or sensory impairment. Dyslexia is manifest by variable difficulty with different forms of language, often including, in addition to problems with reading, a conspicuous problem with acquiring proficiency in writing and spelling”[37]
The discrepancy criterion was no longer found valid, which was particularly clarifying when it came to the group with measured IQ between 70 and 85—the so-called “garden-variety” group. Low IQ could no longer be used as an exclusion criterion from being diagnosed with dyslexia. Towards a Definition of Dyslexia”, Lyon (1995) describes this as a theory-driven working definition that should be changed in accordance with research.
The fact that the field was constantly changing is shown by a definition that emerged from the British Dyslexia Association (BDA) three years later:
“Dyslexia is a complex neurological condition which is constitutional in origin. The symptoms may affect many areas of learning and function, and may be described as a specific difficulty in reading, spelling and written language. One or more of these areas may be affected. Numeracy, notational skills (music), motor functional and organisational skills may also be involved. However, it is particularly related to mastering written language, although oral language may be affected to some degree”[38]
In line with both the WFN and the Orton Society/Lyon definitions, BDA 1998 defines dyslexia as an innate difficulty. Reading, spelling, and writing are described as areas of difficulty, but in addition, there are difficulties that clinicians recognize, namely comorbid difficulties with mathematics, motor skills, attention, and with interpreting symbols, such as sheet music.
A Causal Model
The many theories about what dyslexia is and how dyslexia can be explained have led to a lot of uncertainty and disagreement among researchers, clinicians, in the school system, and, not least, in those concerned. One conclusion of this divergence is that there are several theories that can explain dyslexia, but no one theory alone can give an unambiguous explanation.
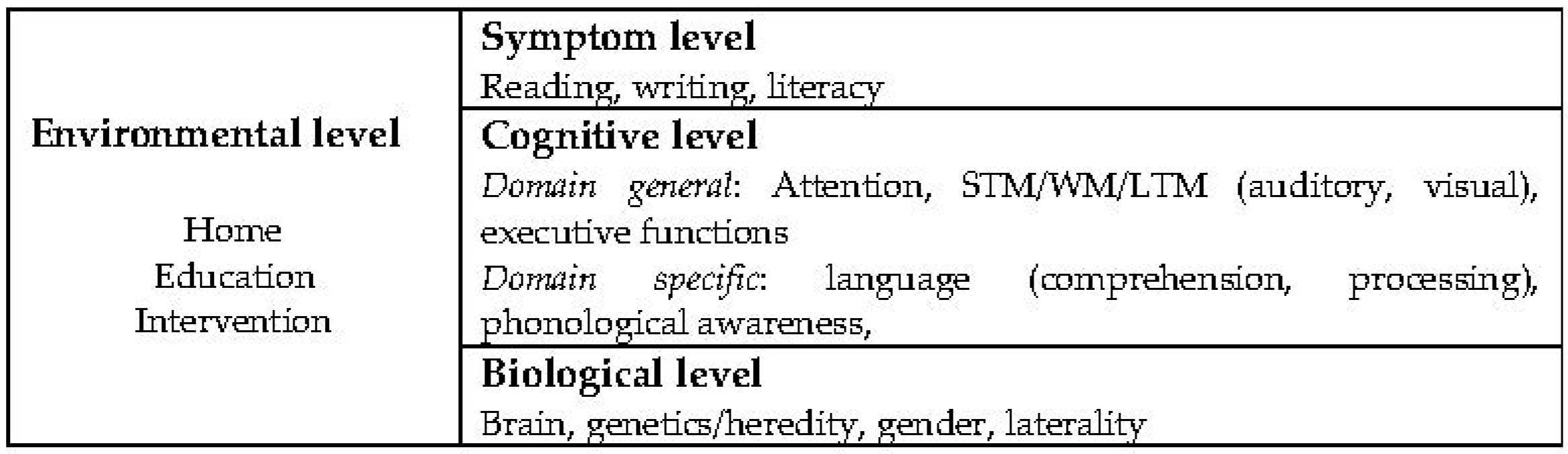
The causal model put forth by Morton and Frith provided a structural approach to several types of deviations [39]. Figure 1 illustrates their four basic interactive levels of explanation. The symptomatic level concerns observable behavior, to be understood at the cognitive level by underpinnings that have to be tested out, and which, again, can be understood or based on known or anticipated biological factors. Further, the environmental level implies the culture in which the person grows.
4. 2000–2020
4.1. 2000–2010, New Definitions
A cross-cultural study led by the Italian scientist Paulesu and his international team introduced exciting and challenging dyslexia research by the new millennium [41]. It focused on whether dyslexia differs in different languages and cultures. An international group of students with dyslexia was tested at the four levels described by Morton and Frith 1995, and modern brain scanning methods were applied. It was concluded that the underlying cognitive and biological factors in people with dyslexia are universal.
Similar views were promoted by the English researcher Elaine Miles [42]. She pointed to the dominant role the Anglo–American language has played in dyslexia research and stressed the importance of bringing out research in different languages. This applies not only to the various orthographic features of the written languages, such as the degree of transparency or depth, but also to the role that linguistic inflection patterns, tonality, and logographic fonts can play in how to define dyslexia. This was also reflected in studies of variations in Chinese dyslexia [43]. Other researchers underlined that writing is as equally important a factor in dyslexia as reading and that cognitive skills that are known to be essential in reading also affect writing [44]. These new approaches were mirrored in concurrent definitions—first, in the definition by the International Dyslexia Association (IDA) in 2002:
“Dyslexia is a specific learning disability that is neurobiological in origin. It is characterized by difficulties with accurate and/or fluent word recognition and by poor spelling and decoding abilities. These difficulties typically result from a deficit in the phonological component of language that is often unexpected in relation to other cognitive abilities and the provision of effective classroom instruction. Secondary consequences may include problems in reading comprehension and reduced reading experience that can impede growth of vocabulary and background knowledge.”[45]
Five years later, a new BDA definition used the terms “literacy” and “language related skills” and included not only cognitive factors but also intervention, with a special focus on digitalization and the role of the teacher:
“Dyslexia is a specific learning difficulty which mainly affects the development of literacy and language related skills. It is likely to be present at birth and to be lifelong in its effects. It is characterised by difficulties with phonological processing, rapid naming, working memory, processing speed, and the automatic development of skills that may not match up to an individual’s other cognitive abilities. It tends to be resistant to conventional teaching methods, but its effects can be mitigated by appropriately specific intervention, including the application of information technology and supportive counselling”[46]
That comorbidity had been ignored or avoided in research by studying “pure” groups was criticized. Due to the relationship between speech, language, and reading disorders, it was argued that to understand these disorders fully, the relationships between them must be considered both on a cognitive and etiological basis [47]. A few years later, the working definition presented in the Rose Report identified the cognitive factors typical of dyslexia and identified dyslexia as a continuum rather than a binary impairment [48]:
“Dyslexia is a learning difficulty that primarily affects the skills involved in accurate and fluent word reading and spelling. Characteristic features of dyslexia are difficulties in phonological awareness, verbal memory and verbal processing speed. Dyslexia occurs across a range of intellectual abilities. It is best thought of as a continuum, not a distinct category, and there are no clear cut-off points. Co-occurring difficulties may be seen in aspects of language, motor coordination, mental calculation, concentration, and personal organization, but these are not, by themselves, markers of dyslexia. A good indication of the severity and persistence of dyslexic difficulties can be gained by examining how the individual responds or has responded to well-founded intervention”[48]
4.2. 2010–2020
In their summary of the current understanding of dyslexia, Peterson and Pennington concluded that much progress had been made in understanding dyslexia [49]. It is a brain-based and neurodevelopmental disorder, multifactorial and universal in nature. Advanced use of brain scanning methods and analyses, as suggested in EEG, and of longitudinal design using fMRI have enhanced the understanding of dyslexia [50][51][52]. Additionally, modern eye tracking methods have shed further light on how the dyslexic brain works during reading [53]. Along with these research methods, frequent comorbidities with other learning disabilities, such as ADHD, language, and mathematic impairment, are in focus [54]. Additionally, the dominance of the Anglo–American language, and hence, problems related to deep orthography, which may have biased the understanding of dyslexia, was questioned in multicultural studies [55][56][57][58][59].
Thus, currently, dyslexia is seen as a complex disorder that varies from person to person, building on the biological, linguistic, psychological, and pedagogical knowledge. According to Snowling, Hulme, and Nation, scholar have still not reached a consensus on what dyslexia is. Rather, they argue that:“ …loosening the criteria for dyslexia has influenced common understanding of the condition and led to diagnostic confusion [60]. In the longer term, the use of the term may need to change …… that loosening the criteria for dyslexia means that a far wider range of individuals now receive the label; furthermore, by understanding the cooccurrence of dyslexia with other disorders, scholars reach a better understanding of the heterogeneity of its manifestations” (p. 501). Further, they conclude that this multi-dimensionality of dyslexia is complex, but to fail to acknowledge this complexity cannot be defended ethically.
With this connotation of dyslexia, a definition recently codified in U.S. law (PL 115–391) is not promising. Here, dyslexia is defined as
“an unexpected difficulty in reading for an individual who has the intelligence to be a much better reader”, as referred to in Shaywitz [61].
This is definitely loosening the grip of any evidence-based understanding of dyslexia, as it is pointing back to the WNF definition of 1968.
5. Evaluation of the Different Definitions
Applying the model by Morton and Frith [39], only two of the definitions reported here meet its requirements. The WNF definition (1968) denotes a symptom (difficulty in learning to read), cognitive traits (adequate intelligence), biological traits (constitutional origin), and environment (sociocultural opportunity). However, as dyslexia is seen as a multifactorial disorder, the four levels are inadequately described in this definition. The second definition that reaches the requirements is that of the BDA [46], which defines symptoms (affects the development of language and literacy skills), the cognitive level (difficulties with phonological processing, rapid naming, working memory, processing speed, and the automatic development of skills that may not match up to an individual’s other cognitive abilities), the biological level (present at birth and to be lifelong in its effects), and environmental level (effects can be mitigated by appropriately specific intervention, including the application of information technology and supportive counselling). Four of the definitions include comorbidities [37][38][46][48], while two include intervention [46][48]. The latest definition codified in U.S. law (PL 115–391) only includes reading and intelligence at the cognitive level.
This entry is adapted from the peer-reviewed paper 10.3390/brainsci12101323
References
- Berkhan. Ueber die Störung der Schriftsprache bei Halbidioten und ihre Aehnlichkeit mit dem Stammeln. Eur. Arch. Psychiatry Clin. Neurosci. 1885, 16, 78–86.
- Hinshelwood, J. Congenital Word-Blindness; HK Lewis & Company: London, UK, 1917.
- Morgan, W.P. A Case of Congenital Word Blindness. Br. Med. J. 1896, 2, 1378.
- Orton, S.T. Specific reading disability—Strephosymbolia. Bull. Orton Soc. 1963, 13, 9–17.
- Orton, S.T. Reading, Writing and Speech Problems in Children; WW. Norton & Company: New York, NY, USA, 1937.
- Chomsky, N. Aspects of the Theory of Syntax; MIT Press: Cambridge, MA, USA, 1965.
- Piaget, J. The Language and Thought of the Child; Hartcourt: New York, NY, USA, 1926.
- Vygotsky, L.S. Thought and language; MIT Press: Cambridge, MA, USA, 1962.
- Miller, G.A. The magical number seven plus or minus two: Some limits on our capacity for processing information. Psychol. Rev. 1956, 63, 81–97.
- Critchley, M. The Dyslexic Child: Developmental Dyslexia, 2nd ed.; ScienceDirect, Public Health; Heinemann: London, UK, 1970; Volume 84, pp. 155–306.
- Matejcek, Z. Report of research group on developmental dyslexia and world literacy. Bull. Orton Soc. 1968, 18, 21–22.
- Frank, G. The Wechsler Enterprise: An Assessment of the Development, Structure and Use of the Wechsler Tests of Intelligence; Elsevier: New York, NY, USA, 2013; Volume 27.
- Johnson, D.J.; Myklebust, H.R. Learning Disabilities: Educational Principles and Practices; Grune & Stratton: New York, NY, USA, 1967; pp. 322–328.
- Boder, E. Developmental Dyslexia: A Diagnostic Approach Based on Three Atypical Reading-spelling Patterns. Dev. Med. Child Neurol. 1973, 15, 663–687.
- Vellutino, F.R. Visual Processing Deficiencies in Poor Readers: A Critique of Traditional Conceptualizations of the Etiology of Dyslexia. In Proceedings of the Annual Meeting of the International Reading Association World ‘Congress’ Reading, Hamburg, Germany, 1–3 August 1978.
- Vellutino, F.R. Dyslexia: Theory and Research; MIT Press: Cambridge, MA, USA, 1979.
- Vellutino, F.R. Dyslexia. Sci. Am. 1987, 256, 34–41.
- Snowling, M.; Hulme, C. A longitudinal case study of developmental phonological dyslexia. Cogn. Neuropsychol. 1988, 6, 379–401.
- Mcbridechang, C. What is phonological awareness. J. Educ. Psychol. 1995, 87, 179–192.
- Shaywitz, B.A.; Fletcher, J.M.; Holahan, J.M.; Shaywitz, S.E. Discrepancy compared to low achievement definitions of reading disability: Results from the Connecticut Longitudinal Study. J. Learn. Disabil. 1992, 25, 639–648.
- Wolf, M.; Bowers, P.G. The double-deficit hypothesis for the developmental dyslexias. J. Educ. Psychol. 1999, 91, 1–24.
- Albert Galaburda, M.D. Developmental dyslexia: Current anatomical research. Ann. Dyslexia 1983, 33, 41–53.
- Geschwind, N.; Galaburda, A.M. Cerebral lateralization: Biological mechanisms, associations, and pathology: I. A hypothesis and a program for research. Arch. Neurosci. 1985, 42, 428–459.
- Geschwind, N.; Galaburda, A.M. Cerebral lateralization: Biological mechanisms, associations, and pathology: II. A hypothesis and a program for research. Arch. Neurosci. 1985, 42, 521–552.
- Geschwind, N.; Galaburda, A.M. Cerebral lateralization: Biological mechanisms, associations, and pathology: III. A hypothesis and a program for research. Arch. Neurosci. 1985, 42, 634–654.
- Bakker, D.J.; Bouma, A.; Gardien, C.J. Hemisphere-specific treatment of dyslexia subtypes: A field experiment. J. Learn. Disabil. 1990, 23, 433–438.
- Bakker, D.J.; Spyer, G. Neuropsychological Treatment of Dyslexia; Oxford University Press: New York, NY, USA, 1990.
- Fawcett, A.J.; Nicolson, R.I. Automatisation deficits in balance for dyslexic children. Percept. Mot. Ski. 1992, 75, 507–529.
- Tallal, P. Temporal or phonetic processing deficit in dyslexia? That is the question. Appl. Psycholinguist. 1984, 5, 167–169.
- Paula, T. Experimental Studies of Language Learning Impairments: From Research to Remediation. In Speech and Language Impairments in Children; Bishop, D.V.M., Leonard, L.B., Eds.; Psychology Press: Cambridge, UK, 2000; pp. 131–155.
- Tallal, P.E.; Galaburda, A.M.; Llinas, R.R.; von Euler, C. Temporal Information Processing in the Nervous System: Special Reference to Dyslexia and Dysphasia. Conference proceedings. New York City, New York, September 12–15, 1992. Ann. N. Y. Acad. Sci. 1993, 682, 1–442.
- Witton, C.; Talcott, J.; Hansen, P.; Richardson, A.; Griffiths, T.; Rees, A.; Stein, J.; Green, G. Sensitivity to dynamic auditory and visual stimuli predicts nonword reading ability in both dyslexic and normal readers. Curr. Biol. 1998, 8, 791–797.
- Lovegrove, W.J. Do dyslexics have a visual deficit? In Studies in Visual Information Processing; North-Holland/Elsevier Science Publishers: Amsterdam, The Netherlands, 1993; pp. 33–49.
- Stein, J.; Walsh, V. To see but not to read; the magnocellular theory of dyslexia. Trends Neurosci. 1997, 20, 147–152.
- Fletcher, J.M. Memory for verbal and nonverbal stimuli in learning disability subgroups: Analysis by selective reminding. J. Exp. Child Psychol. 1985, 40, 244–259.
- Fletcher, J.M.; Francis, D.J.; Shaywitz, S.E.; Lyon, G.R.; Foorman, B.R.; Stuebing, K.K.; Shaywitz, B.A. Intelligent testing and the discrepancy model for children with learning disabilities. Learn. Disabil. Res. Pract. 1998, 13, 186–203.
- Lyon, G.R. Toward a definition of dyslexia. Ann. Dyslexia 1995, 45, 3–27.
- BDA. The British Dyslexia Association Handbook. Reading: British Dyslexia Association; BDA: New York, NY, USA, 1998.
- Morton, J. Causal modeling: A structural approach to developmental psychopathology. Dev. Psychopathol. 1995, 1, 357–390.
- Helland, T. Neuro-Cognitive Functions in Dyslexia. Variations According to Language Comprehension and Mathematics Skills. Ph.D. Thesis, University of Oslo, Oslo, Norway, 2002.
- Paulesu, E.; Démonet, J.F.; Fazio, F.; McCrory, E.; Chanoine, V.; Brunswick, N.; Cappa, S.F.; Cossu, G.; Habib, M.; Frith, C.D.; et al. Cultural diversity and biological unity in dyslexia. Neuroimage 2001, 13, 584.
- Miles, E. Dyslexia may show a different face in different languages. Dyslexia 2000, 6, 193–201.
- Ho, C.S.H.; Chan, D.W.O.; Lee, S.H.; Tsang, S.M.; Luan, V.H. Cognitive profiling and preliminary subtyping in Chinese developmental dyslexia. Cognition 2004, 91, 43–75.
- Berninger, V.W.; Nielsen, K.H.; Abbott, R.D.; Wijsman, E.; Raskind, W. Writing Problems in Developmental Dyslexia: Under-Recognized and Under-Treated. J. Sch. Psychol. 2008, 46, 1–21.
- IDA. Definition; IDA: Washington, DC, USA, 2002.
- BDA. British Dyslexia Associtation: Definition of Dyslexia. 2007. Available online: http://www.bdadyslexia.org.uk/about-dyslexia/faqs.html (accessed on 5 August 2022).
- Pennington, B.F.; Bishop, D.V.M. Relations Among Speech, Language, and Reading Disorders. Annu. Rev. Psychol. 2009, 60, 283–306.
- Rose, J. Identifying and Teaching Children and Young People with Dyslexia and Literacy Difficulties. An Independent Report from Sir Jim Rose to the Secretary of State for Children. 2009. Available online: http://dera.ioe.ac.uk (accessed on 5 August 2022).
- Peterson, R.L.; Pennington, B.F. Developmental dyslexia. Annu. Rev. Clin. Psychol. 2015, 11, 283–307.
- Clark, K.A.; Helland, T.; Specht, K.; Narr, K.L.; Manis, F.R.; Toga, A.W.; Hugdahl, K. Neuroanatomical precursors of dyslexia identified from pre-reading through to age 11. Brain J. Neurol. 2014, 137, 3136–3141.
- Perera, H.; Shiratuddin, M.F.; Wong, K.W. Review of EEG-based pattern classification frameworks for dyslexia. Brain Inform. 2018, 5, 1–14.
- Kuhl, U.; Neef, N.E.; Kraft, I.; Schaadt, G.; Dörr, L.; Brauer, J.; Czepezauer, I.; Müller, B.; Wilcke, A.; Kirsten, H.; et al. The emergence of dyslexia in the developing brain. Neuroimage 2020, 211, 116633.
- Benfatto, M.N.; Seimyr, G.; Ygge, J.; Pansell, T.; Rydberg, A.; Jacobson, C. Screening for Dyslexia Using Eye Tracking during Reading. PLoS ONE 2016, 11, e0165508.
- Toffalini, E.; Losito, N.; Zamperlin, C.; Cornoldi, C. Reading in a transparent second language with limited orality: The case of high school students with dyslexia in Latin. Dyslexia 2018, 25, 57–68.
- Joshi, R.M. Simple View of Reading (SVR) in Different Orthographies: Seeing the Forest with the Trees. Read. Dyslexia 2018, 16, 71–80.
- Landerl, K.; Freudenthaler, H.H.; Heene, M.; De Jong, P.F.; Desrochers, A.; Manolitsis, G.; Parrila, R.; Georgiou, G.K. Phonological Awareness and Rapid Automatized Naming as Longitudinal Predictors of Reading in Five Alphabetic Orthographies with Varying Degrees of Consistency. Sci. Stud. Read. 2019, 23, 220–234.
- Landerl, K.; Ramus, F.; Moll, K.; Lyytinen, H.; Leppänen, P.; Lohvansuu, K.; O’Donovan, M.; Williams, J.; Bartling, J.; Bruder, J.; et al. Predictors of developmental dyslexia in European orthographies with varying complexity. J. Child Psychol. Psychiatry 2013, 54, 686–694.
- Martin, A.; Kronbichler, M.; Richlan, F. Dyslexic brain activation abnormalities in deep and shallow orthographies: A meta-analysis of 28 functional neuroimaging studies. Hum. Brain Mapp. 2016, 37, 2676–2699.
- Parrila, R.; Dudley, D.; Song, S.; Georgiou, G.K. A Meta-Analysis of Reading-Level Match Dyslexia Studies in Consistent Alphabetic Orthographies. Ann. Dyslexia 2020, 70, 1–26.
- Snowling, M.J.; Hulme, C.; Nation, K. Defining and understanding dyslexia: Past, present and future. Oxf. Rev. Educ. 2020, 46, 501–513.
- Shaywitz, B.A.; Shaywitz, S.E. The American experience: Towards a 21st century definition of dyslexia. Oxf. Rev. Educ. 2020, 46, 454–471.
This entry is offline, you can click here to edit this entry!