1. Introduction
Adolescents’ health and well-being are of great concern worldwide [
1]. In 2019, a coalition of governments, United Nations agencies, non-governmental organizations and academic institutions proposed a call to action for adolescent well-being, working closely with adolescents and young people themselves for a more concerted and collaborative approach to their well-being [
2,
3]. Several countries targeted the improvement of food environments with actions directed to adolescents, as summarized by Al-Jawaldeh and colleagues [
4]. Adolescents were mentioned in 12 of the Sustainable Development Goals indicators relevant to health, including those associated with nutrition, reproductive health, sexual and intimate partner violence, child marriage, education and employment [
5]. Investments in this population group are emphasized to deliver a “triple dividend”, i.e., improving their health now, enhancing it throughout their later life course and contributing to the health of future generations [
6].
Despite these initiatives, the health and well-being of adolescents as a population group is still severely challenged.
The rate of adolescents affected by overweight or obesity more than doubled to almost one in five from 1990 to 2016 [
7]. Such increases are mostly the result of changes in the food environment and lifestyle [
8]. Obesity development depends on the relationship between a person and the background, that is, individual physiology and behavior are shaped by strong social and environment factors. Obesity represents a thorny health issue for policymakers, it being a condition that relies on complex and interrelated biological, genetic, social, environmental and behavioral determinants and exerts damaging lifelong effects [
8][
9,
10]. When occurring in adolescence, obesity may have major implications for both the affected adolescent and the society [
11]. It is associated with adolescent metabolic syndrome and a higher risk of obesity and non-communicable diseases (NCDs) in adulthood [
8,
9]. Furthermore, several psychological problems (i.e., body weight stigma, poor self-esteem, eating disorders, internet addiction, etc.) affect the social life and well-being of adolescents with obesity by contributing to addictive behaviors that may lead to a vicious poor self-management cycle (i.e., social isolation, avoidance of healthcare services, decreased physical activity, increased weight gain), which creates additional barriers to healthy behavior changes [
8,
12,
13,
14,
15]. Overall, obesity causes multiple medical, psychological and social co-morbidities, leading to a reduced quality of life, unemployment, increased social disadvantages and, ultimately, to the transmission of risks across generations [
8,
11].
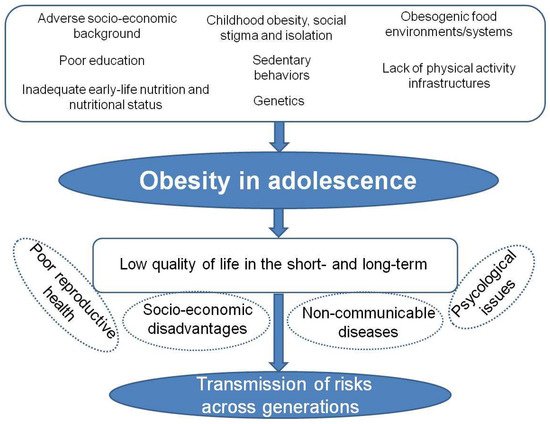
Figure 1 illustrates the complex network of the main causes and consequences of obesity in adolescence.
Figure 1. The interconnected main risk factors and the short- and long-term consequences of obesity in adolescents.
Obesity prevention and treatment strategies—both at the individual and population level—are not working in the long term. Lifestyle and behavioral interventions aimed at reducing calorie intake and increasing energy expenditure have limited effectiveness. Despite being the responsibility of an individual, behavioral changes can be ineffective in the context of a lack of supportive policies in sectors such as health, agriculture, transport, urban planning, environment, food processing and marketing and education. Approaches that combine individual interventions with changes in the environment and society are paramount [
8].
Each year, 12 million girls aged 15–19 years and almost 1 million girls under 15 years give birth [
16]. Pregnancy in these adolescents carries a higher risk of complications than it does in older women [
17,
18,
19]. It is associated with preeclampsia and eclampsia, preterm delivery, a low birth weight and increased neonatal morbidity and mortality [
20,
21,
22,
23]. Furthermore, adolescence motherhood may have important life-altering implications and socioeconomic costs for the adolescent, her child and her family [
24]. By impacting schooling, social connections, employment opportunities, market participation and dependence on state welfare programs, adolescent childbearing holds back the personal development of the girl and reduces her educational attainment and lifetime earnings, thereby nourishing a cycle of poverty for the mother–child dyad [
18].
The Coronavirus disease (COVID-19) pandemic has worsened the existing threats faced by young people, with long-lasting effects on their future health and well-being, and has exacerbated pre-existing inequalities [
25,
26]. School closures were widely implemented across the globe during 2020, affecting over 220 million young people and having negative impacts on their opportunities for learning, critical thinking and the development of their social skills, with likely affected their employment prospects and wider contributions to society [
27]. The loss of sexual and reproductive health services due to restrictions between March and August 2020 led to increased unplanned pregnancies and unsafe abortions for approximately an extra 1.3 million and 1.2 million, respectively [
28]. Restrictive measures have impacted the food environment negatively and have increased food insecurity and physical inactivity, thus contributing to a raised risk for overweight and obesity among young people [
7,
29,
30,
31].
Today’s adolescents are living through “socio-historically situated intersecting crises”, including precarity and climate change [
26,
32]. By challenging human health and well-being with current and future global threats to weather, ecosystems and human systems, climate change is amplifying health and social inequities [
33]. Climate anxiety and pessimistic beliefs about the future, along with emotional dissatisfaction with government responses, are widespread among young people and impact their daily functioning and the risk of mental health problems [
34]. Pathophysiological consequences of heat exposure are documented, including increased risks of interpersonal and collective violence [
35]. Although difficult to be quantified, climate change-related pathways may alter global food production by affecting the quantity, quality and affordability of foods, thus exacerbating nutrient deficiencies, obesity and vulnerability among the most food-insecure populations [
36].
Taken together these challenges can be viewed as the destruction of the social contract with young people. The social contract is “
the entirety of explicit or implicit agreements between all relevant societal groups and the sovereign (i.e., the government or any other actor in power), defining their rights and obligations toward each other” [
37]. According to this contract, governments must guarantee protection, the provision of basic services and participation in political decision-making processes on different levels. People must exert their roles as elected officials, employers, parents, customers and citizens to influence the societal norms and institutional policies of worksites, schools, food retailers and communities [
36]. Adolescents are expected to be not only the beneficiaries but also the central actors in driving the transformative change needed to advance healthy, safe and sustainable food systems and diets [
7].
To date, national policymakers and the international community have failed to protect and listen to young people, and there are continuing gaps in effective programs to support healthy adolescent growth, nutrition and development [
7], as well as education and social justice. Governments tend to place the responsibility for choices about healthy behaviors on citizens, without facilitating policies aimed at addressing the underlying structural determinants of such choices or taking into account that population groups such as adolescents are often unable to adopt them. As Low and colleagues [
38] state:“
When individuals do not realistically have a choice, whether as a result of lack of capability or opportunity, or of demotivating socioeconomic contexts, this reflects the failure of society in providing those aspects of life which permit choice”. Whilst governments may expect citizens—including adolescents, many of whom are too young to vote—to fulfill their side of the social contract in terms of their social obligations, the present situation makes it impossible for them to do so.
The dual challenges of adolescent parenthood and obesity are of great public health relevance because of the life-altering health and socioeconomic effects on both the parents and the offspring. Here, we adopt a new perspective on the issues faced by adolescents by viewing the challenge of adolescent pregnancy against the increasingly common background of obesity in an attempt to provide policymakers, practitioners and academics with suggestions for preventive nutrition-based strategies to break the intergenerational cycle of malnutrition and NCDs.
2. How the Dilemmas from the Broken Social Contract Drive the Problems of Adolescent Pregnancy and Obesity
Obese and pregnant adolescents are the result of diverse underlying societal, economic and other forces. Adolescent pregnancy can be associated with socioeconomic deprivation as both a cause and a consequence. Girls faces work, social and economic dilemmas, as well as gender inequality. The lack of job, services and education feeds into inequalities and amplifies vulnerabilities, unhealthy behaviors, insecurity and long-term implications for educational and occupational achievements within the parents–offspring pair. Around the globe, impoverished and poorly educated girls are more likely to become pregnant than their wealthier and educated counterparts; adolescents from an ethnic minority or marginalized group, who lack choices and opportunities in life or who have limited or no access to sexual and reproductive health are more likely to become pregnant[
39]. Although the right to exercise choice is fundamental to the Universal Declaration of Human Rights, making “healthy choices” is difficult for members of the population who live in low-resource settings and who are socially, educationally, economically or politically disadvantaged [
38]. Poverty and socioeconomic inequalities impact the rates of adolescent motherhood; this emerged from the analysis of results by World Bank income groups, suggesting an inverse relation between income and unintended pregnancy, resulting in substantial differences between low-income and high-income countries, with low-income countries having the highest unintended pregnancy rate and the lowest proportion of unintended pregnancies ending in abortion for 2015–19 [
110]. Women and children in lower socioeconomic groups seem to show high levels of obesity compared with the rest of the population [
24]. Findings from the Millennium Cohort Study, a nationally representative, ethnically diverse birth cohort looking at the trajectories of fat mass index and their ratio over 10 years across childhood and adolescence, showed a less healthy body composition among children and young people growing up in disadvantaged socioeconomic circumstances and living in more deprived areas compared with the more advantaged counterparts [
111]. Mother–offspring dietary trajectories are stable across early life, with poorer diet quality associated with maternal socio-demographic and childhood adiposity [
112]. Poverty likely predisposes low-income individuals towards a suboptimal diet, mostly due to limited purchasing power, which favors fast-food and convenience stores carrying shelf-stable junk foods whilst limiting the access to food outlets stocked with fresh products and whole grains. Nutrient-dense foods such as fresh fruits and vegetables may have a high “per calorie” cost compared to calorie-dense foods that are low in nutritional value [
113]. Living in low socioeconomic status (SES) families, with parents lacking social support or who are unemployed, belonging to a minority group or migrant background and experiencing adverse childhood conditions all lead to a greater risk of obesity [
114]. Adolescent mothers are a population at academic and occupational risk. Moreover, NEET (not in employment, education or training) status is higher among females than among males [
115,
116]. The disconnection from the educational system and the workforce may increase the susceptibility for risky health behaviors, which are already at higher rates among adolescents, ultimately impacting future health [
101]. The educational and occupational attainments of parents are basic factors for the family’s SES, with a higher SES linked to more resources for children’s academic and career development and a larger social context for youth competence development, which may predict young adults’ educational and occupational achievements [
117]. Parents’ education is a form of capital with positive implications for youth achievement. Health literacy may help create a pro-active environment building health, educational and job opportunities. The relevant abstention from formal education among pregnant adolescents causes many of them to not have the opportunity to continue their education once they become a mother. It prevents girls from using their potential to invest in education, find a job and have an income and increases the chances of a recurring pregnancy [
118]. Growing job insecurity and the systematic labor market exclusion of youth at the very beginning of their professional careers are likely linked with high risks of poverty, being part of the precariat, social exclusion, disaffection and insecurity and a higher propensity toward unhealthy behaviors [
119,
120]. The loss of education and unemployment—that is, the lack of food skills and financial resources, respectively—may lead to increased food insecurity [
100], with consequences on the health of the mother–child dyad.
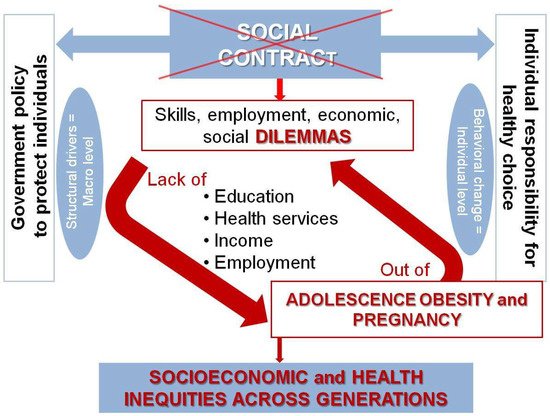
Emerging from the arguments herein discussed, obese adolescent pregnancy can be considered a marker of the broken social contract (Figure 2).
Figure 2. The link between the broken social contract with youth and pregnant adolescents with obesity: a vicious cycle of deepening structural drivers exacerbating the situation across generations unless the policy interventions actively create transformative change.
3. Conclusions and Future Directions
Adolescent obesity and pregnancy are of concern because of the long-lasting consequences on the health and well-being of both the parents-to-be and the next generation. Beyond medical risks, there is a raised social risk related to the physical, emotional, economic and social dependence of adolescent mothers, which may jeopardize several aspects of the mother/infant’s future life. Limited perspectives of personal growth, a lack of educational incentives, labor market and healthy environments affects their opportunities and expectation for the future. Persistent obesogenic environments oppose efforts to facilitate weight loss and prevent weight regain. An obese “precariat” is likely to be in a perpetuating cycle, creating health, economic and social problems that will not just go away.
Considering that the social contract with young people has several break points, society is impelled to re-attain the trust of adolescents. Further efforts on the part of policymakers, healthcare providers and the community must be oriented towards guaranteeing equity and healthy environments for today’s adolescents by implementing the key-factors of successful interventions whilst removing barriers. A more holistic approach is paramount to achieving sustainable, permanent solutions in the real world. This implies a broader perspective of policymakers, including changes in the environment where adolescents live. Prevention cannot be a matter of individual “lifestyle” choices only, but requires collective and policy actions to move from short-term direct benefits or risks to longer-term collective benefits or costs, including the engagement with the food industry. Early-life nutrition, diet diversity, food environments and socioeconomic factors must be considered as the basis on which to further scale up the ongoing initiatives. Actions must be delivered through platforms (e.g., health facilities, community-health workers, schools and mass media) and cross-cutting sectors to nutrition—notably, education, food systems and social safety nets. The health profession may have a key voice in advocating for law taxation and regulation related to food environment and climate. Personal knowledge and competencies need to be mediated by organizational structures and the availability of resources, which enable people to access, understand, appraise and use information and services in ways that promote and maintain good health and well-being for themselves and those around them. Adolescent interventions must vary in terms of form and effectiveness by age, sex, income level and geography, along with social, cultural and country context. Some interventions must be adolescent-specific, and others must be adolescent-inclusive. Achieving universal health coverage requires adolescents themselves to be empowered to initiate action and influence decisions that affect their health and development through meaningful participation. Although personal behaviors are influenced by environments, people can act as agents of change in their roles as citizens. Young people themselves are demanding roles beyond being consumers. Adolescents have the potential to unlock the political and policy paralysis around unhealthy and unequal environments and systems. Stronger participation and demand from civil society for political action are necessary.
This entry is adapted from the peer-reviewed paper 10.3390/nu14173550