Atherosclerotic cardiovascular disease (ASCVD) morbidity and mortality are decreasing in high-income countries, but ASCVD remains the leading cause of morbidity and mortality in high-income countries. Over the past few decades, major risk factors for ASCVD, including LDL cholesterol (LDL-C), have been identified. Statins are the drug of choice for patients at increased risk of ASCVD and remain one of the most commonly used and effective drugs for reducing LDL cholesterol and the risk of mortality and coronary artery disease in high-risk groups. Unfortunately, doctors tend to under-prescribe or under-dose these drugs, mostly out of fear of side effects. The latest guidelines emphasize that treatment intensity should increase with increasing cardiovascular risk and that the decision to initiate intervention remains a matter of individual consideration and shared decision-making.
1. Introduction
Statins are commonly used drugs in patients at high cardiovascular risk. These drugs reduce serum low-density lipoprotein cholesterol (LDL-C), which is involved in the pathogenesis of cardiovascular disease [
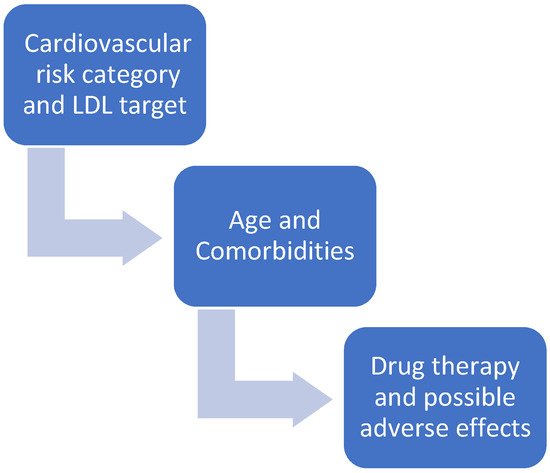
1]. Proper treatment of patients with hypercholesterolemia begins with the notion that not all patients are the same and that treatment must be individualized. The first step is to determine the patient’s overall cardiovascular risk [
2] (
Figure 1). Depending on each patient’s specific risk category, specific therapeutic targets for LDL cholesterol need to be achieved [
2]. In addition to cardiovascular risk, individual patient characteristics and possible adverse effects of drugs in specific patient categories must also be considered (
Figure 1). In addition, statins vary in their chemical composition (
Figure 2), pharmacokinetics, and potency of lowering LDL cholesterol [
3].
Figure 1. How to decide which statin and what dosage.
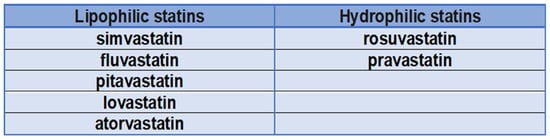
Figure 2. Hydrophilic and lipophilic statins.
1.1. Are Statins All the Same?
Statins are the drug of choice for the treatment of hypercholesterolemia to lower LDL cholesterol. They act principally in the liver by competitively inhibiting 3-hydroxy-3-methylglutaryl-CoA reductase activity. The pharmacological activity determines the decrease in intracellular cholesterol concentration, which leads to an increase in the expression of LDL receptors on the surfaces of hepatocytes. Increased LDL receptor expression leads to increased uptake of LDL-C in the blood, resulting in lower plasma concentrations of LDL-C and other apolipoprotein B-containing lipoproteins, including triglyceride-rich particles [
1]. Although all statins act by the same mechanism of action, they differ in chemical composition and pharmacokinetics, affecting treatment and adverse effects. Lovastatin, pravastatin, and simvastatin are fungal-derived 3-hydroxy-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors, while atorvastatin, cerivastatin, fluvastatin, pravastatin, pitavastatin, and rosuvastatin are fully synthetic compounds [
4]. Atorvastatin, fluvastatin, lovastatin, and simvastatin are relatively lipophilic compounds, while pravastatin and rosuvastatin are more hydrophilic (
Figure 3) [
5]. Lipophilic drugs are more susceptible to oxidative metabolism by the CYP450 system (cytochrome P450) [
6]. Due to the risk of drug interactions that inhibit CYP450, statins metabolized by the CYP450 system are more likely to cause muscle damage; this leads to increased blood statin levels, which lead to an increased risk of toxic effects [
7]. Several studies have compared lipophilic and hydrophilic statins in the clinical setting [
8,
9]. Lipophilic statins reduce adenosine triphosphate (ATP) production, which theoretically increases myocardial stunning after ischemia and worsens myocardial function after reperfusion [
10]. This was demonstrated in an animal study in which lipophilic statins exacerbated myocardial shock and decreased tissue ATP following coronary reperfusion, whereas hydrophilic statins did not show these effects. A meta-analysis concluded that lipophilic statins have risks of major adverse cardiovascular events, myocardial infarction, and all-cause mortality comparable with hydrophilic statins [
11].
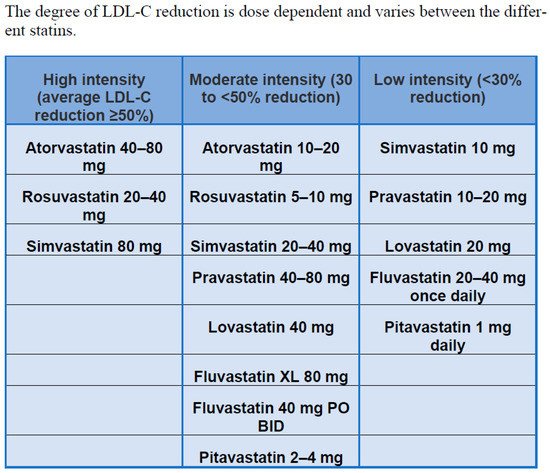
Figure 3. Intensity of statin therapy [
12].
The largest study (involving the most patients, drugs, and doses) was the CURVES study [
13], which compared doses of atorvastatin (10, 20, 40, and 80 mg), simvastatin (10, 20, and 40 mg), pravastatin (10, 20 and 40 mg), fluvastatin (20 and 40 mg) and lovastatin (20, 40 and 80 mg). This was a multicenter, randomized, open-label, 8-week, parallel-group study of 534 hypercholesterolemic patients with LDL values above 160 mg/dL and triglycerides above 400 mg/dL. Atorvastatin 10, 20, and 40 mg resulted in greater LDL-C lowering than equivalent doses of simvastatin, pravastatin, lovastatin, and fluvastatin (238%, 246%, and 251%). Atorvastatin 10 mg produced LDL-C lowering comparable to simvastatin 10, 20 and 40 mg, pravastatin 10, 20 and 40 mg, lovastatin 20 and 40 mg, and fluvastatin 20 and 40 mg. Atorvastatin 10, 20, and 40 mg resulted in greater reductions in total cholesterol compared to mg-equivalent doses of simvastatin, pravastatin, lovastatin, and fluvastatin. All reductase inhibitors tested were similarly tolerated.
1.2. Cardiovascular Risk Category and LDL-C Target
Treatment goals have been defined according to different risk categories (they apply to primary and secondary prevention; treatment must always be combined with lifestyle changes) [
2] (
Table 1).
Table 1. LDL-C target according to cardiovascular risk.
| RISK CATEGORY. |
WHICH PATIENT? |
LDL-C TARGET |
| Very high-risk patients (10-year risk of cardiovascular mortality > 10%) |
Atherosclerotic cardiovascular disease (ASCVD) documented clinically or by imaging (acute coronary syndrome, stable angina, coronary revascularization, stroke or transient ischemic attack, peripheral arterial disease).
Imaging documented ASCVD, including findings known to be relevant to the development of future clinical events, such as
Diabetes mellitus (DM) with end-organ damage (microalbuminuria, retinopathy, and neuropathy) or at least 3 CV (cardiovascular) risk factors or early-onset type 1 diabetes that has been present for more than 20 years.
Severe chronic kidney disease (eGFR < 30 mL/min/1.73 m2). |
LDL < 55 mg/dL or reduce LDL by at least 50% compared to baseline levels |
| Very very high-risk patients |
Very high-risk patients who experience a second vascular event within 2 years of the first during therapy with statins at the highest tolerable dosage. |
LDL < 40 mg/dL |
| High-risk patients (10-year risk of cardiovascular mortality 5–10%) |
Particularly high individual risk factors, such as total cholesterol > 310 mg/dL (>8 mmol/L), LDL-C > 190 mg/dL (>4.9 mmol/L) or blood pressure ≥ 180/110 mmHg.
Familial hypercholesterolemia without other CV risk factors.
Diabetes mellitus without end organ damage, but present for at least 10 years or in conjunction with another CV risk factor.
Chronic moderate kidney disease (eGFR 30–59 mL/min/1.73 m2). |
LDL < 70 mg/dL or reduce LDL values by at least 50% compared to the initial ones |
| Moderate risk patients (10-year risk of cardiovascular mortality > 1% <5%) |
Diabetes in young subjects (T1DM < 35 years, T2DM < 50 years), present for less than 10 years and in absence of other risk factors |
LDL < 100 mg/dL |
| Low-risk patients (risk of cardiovascular mortality at 10 years < 1%) |
|
LDL < 116 mg/dL |
This entry is adapted from the peer-reviewed paper 10.3390/ijms23169326