Atopic dermatitis (AD) is a highly heterogeneous inflammatory disease regarding both its pathophysiology and clinical manifestations. However, it is treated according to the “one-size-fits-all” approach, which may restrict response to treatment. Thus, there is an unmet need for the stratification of patients with AD into distinct endotypes and clinical phenotypes based on biomarkers that will contribute to the development of precision medicine in AD. The development of reliable biomarkers that may distinguish which patients with AD are most likely to benefit from specific targeted therapies is a complex procedure and to date none of the identified candidate biomarkers for AD has been validated for use in routine clinical practice. Reliable biomarkers in AD are expected to improve diagnosis, evaluate disease severity, predict the course of disease, the development of comorbidities, or the therapeutic response, resulting in effective and personalized treatment of AD.
1. Introduction
Atopic dermatitis (AD) is a common inflammatory skin disorder affecting up to 25% of children and up to 10% of adults [
1,
2]. Apart from the inflammation of the skin, AD is also characterized by systemic inflammation manifesting with other atopic (asthma, allergic rhinitis), non-atopic (cutaneous lymphomas) and psychiatric (anxiety, depression) co-morbidities, epidermal barrier dysfunction and persistent pruritus [
3]. AD is often associated with elevated serum immunoglobulin E (IgE) levels and a personal or family history of type I allergies. Its course involves chronic relapses that significantly compromise the patients’ quality of life [
1]. With its very high incidence in childhood, chronicity, devastating effect on quality of life for the affected patients and their families, enormous socioeconomic costs, and the recent development of new promising therapeutic options, AD represents a major challenge.
AD has a complex pathogenesis involving multiple genetic, immunologic, and environmental factors, which leads to a dysfunctional skin barrier and dysregulation of the immune system [
4]. The disease is characterized by high heterogeneity in both pathophysiology and clinical manifestations leading to its classification into different endotypes or subtypes and clinical phenotypes [
5]. Regarding immunologic heterogeneity, although AD is primarily characterized by excessive activation of type 2 T helper (Th2) cells and type 2 innate lymphoid (ILC2) cells, with a predominant increase in type 2 cytokines in the skin, the additional activation of Th1, Th17 and Th22 cytokine pathways also contributes to its pathogenesis. [
6,
7]. Moreover, the clinical manifestations of AD can be classified according to their correlation with patients’ age, disease severity, age of onset and ethnic origin [
8].
Despite the high degree of clinical and molecular heterogeneity of AD, the disease is currently treated according to the “one-size-fits-all” approach, which may restrict the efficacy of the therapy administered [
8]. Even the newly developed biologic agents that target specific cytokines or their receptors and the broad-acting Janus kinase inhibitors fail to completely control disease in most AD patients [
9,
10,
11,
12]. In addition, to date, the diagnosis is exclusively based on clinical criteria due to the lack of distinct laboratory or histological features, while the quantification of disease severity using measurement tools, such as the SCORing of Atopic Dermatitis (SCORAD), Eczema Area and Severity Index (EASI) and Investigator’s Global Assessment (IGA), relies on the observer’s subjective assessment [
13]. Therefore, there is still a high unmet medical need for the identification of reliable biomarkers that could reduce observatory differences and would be useful as objective tools for the diagnosis, disease severity measurement and especially the development of precision medicine in AD.
2. Definition and Subtypes of Biomarkers
To date, there are available several, although overlapping, definitions of the term biomarker. A biomarker or biological marker is defined as a “characteristic that is objectively measured and evaluated as an indicator of normal biologic processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention”, according to the National Institutes of Health (NIH) [
14]. Another definition of biomarker proposed by the World Health Organization (WHO) is as follows: “any substance, structure or process that can be measured in the body or its products and influence or predict the incidence of outcome or disease. Biomarkers can be classified into markers of exposure, effect, and susceptibility” [
15].
Since biomarkers are widely used in the process of drug discovery, development and approval, the initial definition of NIH has evolved into a broader, enriched definition of biomarker adopted by the Food and Drug Administration (FDA) namely: “a defined characteristic that is measured as an indicator of normal biological processes, pathogenic processes, or responses to an exposure or intervention, including therapeutic interventions. Molecular, histologic, radiographic, or physiologic characteristics are types of biomarkers. A biomarker is not an assessment of how a patient feels, functions, or survives” [
16]. Moreover, the European Medicines Agency (EMA) defines a biomarker more restrictively as ‘‘a biological molecule found in blood, other body fluids, or tissues that can be used to follow body processes and diseases in humans and animals’’ [
17].
The biologic origin of a biomarker could be genomic information, transcriptomic profiles obtained by analysis of mRNA and miRNA, proteins such as cytokines and other mediators from body fluids (whole blood, serum, plasma, tissue fluids) or tape stripping, and morphological information [
18]. Regarding the purpose/value of biomarkers, there are seven different categories as defined by the FDA-NIH Biomarker Working Group: susceptibility/risk, diagnostic, monitoring/severity, prognostic, predictive, pharmacodynamic/response, and safety [
16]. Thus, evaluation of all these subtypes of biomarkers could play a significant role in the diagnosis, prognosis, management, and treatment of AD.
3. Biomarkers in AD
Clinical research has discovered several different subtypes of potential biomarkers in AD. However, to date none of these candidate biomarkers are used in routine clinical practice, since they have not yet reached the status of validation and qualification [
19]. Recently, an international panel of experts consented that the most important performance elements for high-quality AD biomarkers are reliability, clinical validity, relevance, and high positive predictive value. Regarding the purpose of biomarkers in AD, the prediction of therapeutic response and disease progression was considered the most important. Additionally, insufficient validation by independent researchers was reported as a major obstacle to the transfer of AD biomarkers in clinical practice. All experts identified validation and further studies as a high-priority research objective [
2].
Most of the skin biomarkers in AD have been identified using whole-tissue skin biopsy for sample retrieval, an invasive approach that is not always feasible, especially in the pediatric population. Consequently, less invasive sampling methods have been recently developed for AD biomarker assessment, such as the use of tape strips [
20,
21,
22,
23], dried blood spots [
24], patients’ serum [
25], or saliva [
26].
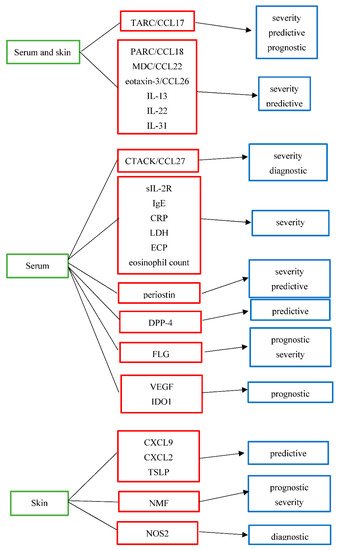
Candidate AD biomarkers can be divided into different subtypes according to their suggested use. The candidate biomarkers for AD and their suggested use are summarized in Table 1 and Figure 1.
Figure 1. Biologic origin and suggested use of potential biomarkers in atopic dermatitis. TARC/CCL17: thymus and activation-regulated chemokine/C-C motif ligand 17, PARC/CCL18: pulmonary and activation-regulated chemokine/C-C motif ligand 18, MDC/CCL22: macrophage-derived chemokine/C-C motif ligand 22, eotaxin-3/CCL26: eosinophil-attracting chemokine/C-C motif ligand 26, IL-13:interleukin-13, IL-22:interleukin-22, IL-31:interleukin-31, CTACK/CCL27:cutaneous T-cell-attracting chemokine/C-C motif ligand 27, sIL-2R:soluble IL-2 receptor, IgE:immunoglobulin E, CRP:C-reactive protein, LDH:lactate dehydrogenase, ECP:eosinophil cationic protein, DPP-4:dipeptidyl peptidase-4, FLG:filaggrin, VEGF:vascular endothelial growth factor, IDO1:indoleamine 2,3-dioxygenase-1, CXCL9:C-X-C motif ligand 9, CXCL2:C-X-C motif ligand 2,TSLP: thymic stromal lymphopoietin protein, NMF:natural moisturizing factor, NOS2:nitric oxide synthase 2.
Table 1. Candidate biomarkers in atopic dermatitis.
|
Biomarker
|
Full Name
|
Purpose
|
Grade of Evidence
|
Biologic Origin
|
|
TARC/CCL17 [13,25,27,28,29,30,32,33,34,35,36,37,38,40,53,69]
|
thymus and activation-regulated chemokine/
C-C motif ligand 17
|
severity
predictive
prognostic
|
high
moderate
low
|
serum and skin
|
|
PARC/CCL18 [25,27,28,29]
|
pulmonary and activation-regulated chemokine/C-C motif ligand 18
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
MDC/CCL22 [13,25,27,28,29,30,76]
|
macrophage-derived chemokine/C-C motif ligand 22
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
Eotaxin-3/CCL26 [25,27]
|
eosinophil-attracting chemokine/C-C motif ligand 26
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
IL-13
[9,25,27,77,78,79,80]
|
interleukin-13
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
IL-22
[25,27,28,29,75,77,78,79,80]
|
interleukin-22
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
IL-31
[13,52,53,54,55,56,57,58]
|
interleukin-31
|
severity
predictive
|
moderate
low
|
serum and skin
|
|
CTACK/CCL27 [13,25,27,33,34,82,83,84]
|
cutaneous T-cell-attracting chemokine/
C-C motif ligand 27
|
severity
diagnostic/differential diagnosis from psoriasis
|
moderate
low
|
serum
|
|
sIL-2R
[13,28,29]
|
soluble IL-2 receptor
|
severity
|
moderate
|
serum
|
|
IgE [13,40,41,45,46]
|
immunoglobulin E
|
severity
|
moderate
|
serum
|
|
CRP [39]
|
C-reactive protein
|
severity
|
low
|
serum
|
|
LDH
[13,39,40,41]
|
lactate dehydrogenase
|
severity
|
moderate
|
serum
|
|
ECP
[13,42,43]
|
eosinophil cationic protein
|
severity
|
moderate
|
serum
|
|
Eosinophil count [40,41,43,44]
|
|
severity
|
moderate
|
serum
|
|
Periostin [9,44,48,49,50]
|
|
severity
predictive
|
moderate
low
|
serum
|
|
DPP-4 [9]
|
dipeptidyl peptidase-4
|
predictive
|
low
|
serum
|
|
CXCL9 [76]
|
C-X-C motif ligand 9
|
predictive
|
low
|
skin
|
|
CXCL2 [76]
|
C-X-C motif ligand 2
|
predictive
|
low
|
skin
|
|
TSLP [70]
|
thymic stromal lymphopoietin protein
|
predictive
|
moderate
|
skin
|
|
NMF
[59,71]
|
natural moisturizing factor
|
prognostic
severity
|
moderate
low
|
skin
|
|
FLG [47,59,62,65,66,67]
|
filaggrin
|
prognostic
severity
|
moderate
low
|
serum
|
|
VEGF [73]
|
vascular endothelial growth factor
|
prognostic
|
low
|
serum
|
|
IDO1 [74]
|
indoleamine 2,3-dioxygenase-1
|
prognostic for eczema herpeticum
|
low
|
serum
|
|
NOS2
[82,83,84]
|
nitric oxide synthase 2
|
diagnostic/differential diagnosis from psoriasis
|
low
|
skin
|
This entry is adapted from the peer-reviewed paper 10.3390/jcm11164639