Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread over the world, having a huge impact on people’s lives and health. The respiratory system is often targeted in people with the coronavirus disease 2019 (COVID-19). The virus can also infect many organs and tissues in the body, including the reproductive system.
- SARS-CoV-2
- COVID-19
- ACE2
- RAS
- fertility
- reproduction
1. Does COVID-19 Affect Male Fertility? What Is the Possible Role of RAS?
The interaction of the SARS-CoV-2 viral spike protein with angiotensin converting enzyme 2 (ACE2) on cells co-expressing ACE2 and the cellular transmembrane protease serine 2 (TMPRSS2) has been identified as the SARS-CoV-2 virus’s cellular entry mechanism. Since the testes express ACE2 receptors, researchers are investigating the effects of COVID-19 on male fertility [16]. Endocrinologically, the hypothalamic–pituitary–gonadal (HPG) axis connects the brain and the testes. The production of gonadotropins and testosterone, as well as the HPG feedback loop, are responsible for this connection. The effects of COVID-19 on the hypothalamic–pituitary–gonadal axis are still under investigation; however, aberrant gonadotropin levels have been reported in COVID-19 patients [17].
Maintaining a normal testosterone production requires a healthy HPG axis. Several studies reported that COVID-19 influences testicular hormone production. In fact, researchers discovered high luteinizing hormone (LH) levels and reduced testosterone to LH ratios in COVID-19 patients. These findings were linked to systemic inflammation in the patients examined [18]. Moreover, when compared to more moderate cases, 12.9 percent of patients who died or had severe COVID-19 had reduced total and free testosterone and raised LH [19].
Researchers related circulating gonadotropin levels in COVID-19 patients to neuropathology. Neuroimaging of a single patient indicated hyperintense signals, which could indicate hypothalamic abnormalities as well as an expanded pituitary gland [20]. Even though these data are preliminary, they suggest that hypothalamic perturbation in COVID-19 patients may disrupt gonadotropin release regulation, resulting in a drop in testosterone levels.
Furthermore, it has been proven that SARS-CoV-2 can cross the blood–brain barrier and infect ACE2-expressing cells, causing neuroinflammation [17,21]. Normal physiologic activities like temperature regulation and hormone balance can be disrupted by inflammation [20,22]. Fever is the body’s reaction to systemic inflammation and one of the most reported symptoms of COVID-19 [23]. A temperature higher than 39 °C for more than three days has been linked to a considerable drop in semen concentration and motility [24]. Therefore, the possible effect of COVID-19 on male fertility can be an indirect consequence of associated fever.
The blood–testes barrier offers the testicles special immunity. Inflammation, both systemic and local, can enhance permeability and allow immune cells to invade [25]. A SARS-CoV-2 infection generates a proinflammatory response in the body and can trigger cell pyroptosis, a programmed cell death associated with the production of proinflammatory cytokines. Inflammatory cytokines induce immune cell recruitment, which might lead to a cytokine storm and uncontrolled systemic inflammation affecting various organ systems [26]. Inflammatory markers such as interleukine-6 (IL-6), IL-8, and tumor necrosis factor-alpha (TNF-α) have been detected in semen samples from individuals recovering or suffering from COVID-19 [27,28]. Inflammatory cytokines and oxidative stress have both been shown to harm testes’ biological components [29]. In fact, oxidative stress damages Leydig cells, impairing testosterone synthesis and spermatogenesis [30]. Therefore, the testicular damage reported in COVID-19 patients has been linked to oxidative stress as a possible cause. For example, in an autopsy investigation of COVID-19 patients, a statistically significant increase in reactive oxygen species (ROS) and a reduction in glutathione disulfide (GSH) levels [31].
Furthermore, the membrane-bound ACE2, a significant component of the RAS, is the human gate that allows the SARS-CoV-2 virus to enter host cells [32,33]. Since RAS appears to have various effects on male fertility, it could be possible that COVID-19 consequences on male fertility is linked to RAS impairment. In fact, in human and mammalian animal models, typical components of the RAS have been identified in the testis and epididymis [34,35,36] (Figure 1A). In humans, ACE2 expression is high in the spermatogonia, Leydig, and Sertoli cells of adult human testis in the testes [37,38]. In addition, an abnormal expression of genes implicated in mitochondrial function and testicular steroidogenesis was observed in knockout mammalian models of RAS components [34,39]. Together, the RAS and its ACE2 receptor play an important role in male reproduction by regulating steroidogenesis, testosterone production, and spermatogenesis in the testis in human males (Figure 1B). Since COVID-19 impairs these pathways, it is not surprising that male fertility is affected after SARS-CoV-2 infection. In addition, since ACE2 is expressed on endothelial cells, the SARS-CoV2 infection of these cells can lead to endothelial dysfunction and inflammation affecting male fertility (inducing erectile dysfunction) [40].
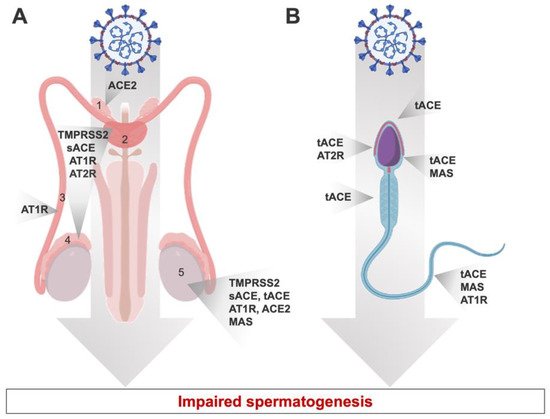
Figure 1. Expression of RAS components in different localizations of the human male reproductive system (A) and throughout spermatozoa (B). tACE: testicular angiotensin converting enzyme; AT1R: angiotensin II type 1 receptor; AT2R: angiotensin II type 2 receptor; MAS: Mas receptor; TMPRSS2: transmembrane protease serine 2; ACE: angiotensin-converting enzyme; sACE: somatic ACE. 1: vas deferens; 2: prostate; 3: epididymis; 4: seminal plasma; 5: Testis.
2. The Effect of COVID-19 on Female Fertility
Women that were infected by SARS-CoV-2 reported changes in menstrual cycle frequency and regularity, altered menstrual duration and volume, worsening premenstrual syndrome, and increased dysmenorrhea. Therefore, questions were raised about the impact of COVID-19 on female reproduction after the viral infection.
The abundance of RAS components in the female reproductive system suggests its vulnerability to SARS-CoV-2 infection. ACE2 is widely expressed in the ovary, uterus, vagina, and placenta [15]. ACE2 controls follicular development and ovulation, as well as luteal angiogenesis and degeneration, along with endometrial tissue alterations and embryo development [15]. Other components of RAS are abundant in the female reproductive system such as the Ang1-7 that is expressed in theca-interstitial cells. The presence of ACE2 and Ang1-7 in all phases of follicular development suggests that they may play an important role in fertility [15,36]. Based on these evidence, SARS-CoV-2 infection may disrupt female fertility by damaging ovarian tissue, granulosa cells, and endometrial epithelial cells [41]. By downregulating ACE2 levels, the infection results in higher levels of AngII, which has been linked to proinflammatory, profibrotic, and proapoptotic effects. Consequently, this could influence ovarian function and lead to an increase in ovarian oxidative stress [42]. Of note, SARS-CoV-2 was not identified in vaginal fluid and cervical exfoliated cells, suggesting that the lower female genital tract may not be a transmission route for SARS-CoV-2 [43]. These findings were contradicted in another study in which SARS-CoV-2 was detected using vaginal RT-PCR in some patients [44]. Whether there is a link between viral load and the detection threshold of the virus vaginal levels should be investigated further. Taken together, the findings suggest that the female reproductive system, which expresses ACE2, is vulnerable to SARS-CoV-2 infection, and thus fertility could be affected.
The dynamic expression of RAS in the stromal and epithelial cells of the endometrium during the cycle could explain the changes in the menstrual cycle observed during SARS-CoV-2 infection [15,45,46]. In fact, the RAS is effective for controlling menstrual cycles, enabling blood vessel renewal, and triggering menstruation [15]. The balanced expression of the stimulatory factor AngII and the inhibitory factor Ang1-7 regulates these processes [15]. Since SARS-CoV-2 infection affects RAS, complications touching RAS-regulated physiological systems are possible.
SARS-CoV-2 encodes proteins that can activate the NOD-, LRR-, and pyrin domain-containing protein 3 (NLRP3) inflammasome assembly [47,48]. In fact, one of the first defenses against viral infections is the inflammasome, which is a key player of the innate immunity. When NLRP3 is activated, it attracts Caspase-1, which boosts the expression of interleukins IL-1β and IL-18 [49,50]. Since women with a history of recurrent miscarriages have higher levels of NLRP3 and proinflammatory cytokines in their endometrium [51], it is possible that SARS-CoV-2-associated inflammation affects female fertility.
This entry is adapted from the peer-reviewed paper 10.3390/biomedicines10081775
This entry is offline, you can click here to edit this entry!