Of the eight essential amino acids, tryptophan has the lowest reserves and is therefore more prone to deficiency during malnutrition or catabolic states than the other seven [
1]. In addition to being a building block in protein biosynthesis, of which as little as 1% of ingested tryptophan is normally used, most of this aromatic substance is metabolised via several pathways to bioactive metabolites of clinical importance [
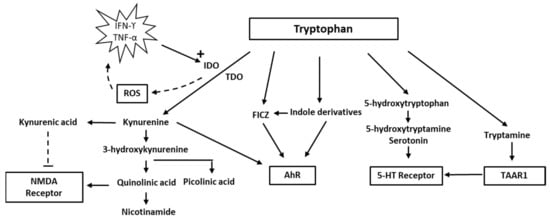
2]. The best known of these pathways is enzymatic conversion to serotonin, of which >90% is normally formed in the distal part of the small intestine and the rest in the central nervous system (CNS). This pathway involves two enzyme complexes. The first and rate-limiting step is the conversion of tryptophan to 5-OH-tryptophan, catalysed by the tryptophan hydroxylase, which is then followed by the amino acid decarboxylation by aromatic-L-amino acid decarboxylase (AADC) to produce serotonin (
Figure 1). Tryptophan hydroxylase catalyses the monooxygenation of tryptophan, using one oxygen atom from O
2; the other oxygen atom is accepted by tetrahydrobiopterin. The reaction requires Fe(II). An alternative pathway is direct decarboxylation to tryptamine by intestinal bacteria or in neurons that express only AADC, and not tryptophan hydroxylase [
3,
4]. Tryptamine belongs to a group of endogenous “trace amines” produced by the decarboxylation of amino acids that have a high turnover rate. They act on the trace amine-associated receptors (TAARs)—a group of G-protein-coupled receptors [
3]. TAAR1 is expressed in the brain, and agonists appear to modulate the classical monoaminergic neurotransmission. In recent years, attention has been increasingly focused on the medical significance of the enzymatic oxidation of tryptophan to form various indole compounds and toxic and protective metabolites within the so-called kynurenine pathway [
5,
6]. The kynurenine pathway leads to the production of kynurenine, and further to quinolinic acid, niacin, and nicotinamide adenine dinucleotide (NAD). The kynurenine pathway occurs mainly in the liver, its initial steps being catalysed by the tryptophan-2,3 dioxygenase (TDO), but also in the brain by the enzymes indoleamine dioxygenase 1 and 2 (IDO1, IDO2), which are more widely expressed [
4]. A rate-limiting step in the kynurenine pathway catalysed by IDO uses molecular oxygen in the oxidation of tryptophan and as cofactor iron in its Fe(II) form [
7]. Reactive oxygen species (ROS) may arise from the enzymatic activity of IDO [
8]. Yet another pathway that occurs in the intestine is the conversion of tryptophan by the bacterial enzyme tryptophanase to indole and indole derivatives, such as indole-3-acetic acid [
4].
The enzymes tryptophan dioxygenase (TDO) and indoleamine dioxygenase (IDO) use dioxygen for oxidation and Fe(II) iron as cofactor in the conversion of tryptophan to kynurenine. IDO expression is increased by TNF-alpha or INF-gamma. The activated Fe(II) forms of IDO may generate reactive oxygen species (ROS). The metabolite quinolinic acid, further down the kynurenine pathway, may act as an agonist of the NMDA receptor, whereas kynurenic acid works as an antagonist. Formation of the neuroprotective picolinic acid is an alternative pathway to quinolinic acid. Other pathways include the formation of serotonin and tryptamine; tryptamine agonises the trace amine associated receptor 1 (TAAR1) that modulates the classical monoaminergic neurotransmission and the indole pathway. Kynurenine, indole derivatives, and 6-formylindolo(3,2-b) carbazole (FICZ) bind to the aryl hydrocarbon receptor (AhR). FICZ may be formed from indole derivatives or upon exposure of tryptophan to H2O2, and it binds with an extremely high affinity to AhR (see text).
2. Tryptophan and Indolamine Dioxygenase
Indoleamine 2,3-dioxygenase belongs to the family of oxidoreductases, which also includes tryptophan 2,3-dioxygenase (TDO), sometimes referred to as tryptophan oxygenase. Both TDO and IDO contain a non-covalently bound Fe(II) heme unit per monomer. TDO is usually tetrameric, whereas IDO is monomeric. Several researchers [
14,
15] have discussed the mechanisms of tryptophan oxidation. It is assumed that it involves catalytic activity of the Fe(II) heme moiety of the enzymes and that TDO and IDO react by similar mechanisms. Because the interaction of tryptophan with oxygen appears to include the formation of an intermediary ferryl compound that may act as a strong oxidant [
16], the IDO reaction may contribute to oxidative stress [
17,
18]. ROS may lead to increased production of inflammatory cytokines (TNF-alpha and IL-6, i.e., from macrophages), further upregulating IDO and thereby instigating a vicious circle [
19]. The harmful effects of ROS formed from the IDO reaction may be counteracted by such endogenous antioxidants as the glutathione (GSH)/GSH-peroxidase system and presumably also by such exogenous antioxidants as polyphenols.
Increased production of peroxide and ROS resulting from IDO activation may conceivably disrupt the finely tuned interaction between intracellular oxidants and antioxidants, concurrent with a change in the tryptophan/kynurenine ratio. Overexpression of IDO, leading to an accelerated tryptophan–kynurenine pathway and ROS production, may cause a depressed intracellular concentration of reduced GSH and disrupt the intracellular redox balance [
20]. Upon interaction with ROS, intracellular GSH is rapidly oxidised to its disulfide form GSSG [
21], which can either be reduced again enzymatically to GSH intracellularly or expelled from the cells [
22,
23], where it may form S-glutathionylated plasma proteins [
24] or lead to increased extracellular levels of its amino acid constituents [
25], which can be detected in blood [
26]. Under the redox conditions existing in circulating blood, not only oxidised GSH, but also cysteine and homocysteine, will exist predominantly as mixed disulfides with albumin or other plasma proteins [
27,
28]. Kynurenine and its breakdown products, such as quinolinic acid, have diverse biological impacts, including immunological and psychological effects [
11,
29,
30]. In addition, the interferon (IFN-α) treatment for hepatitis C may precipitate depressive symptoms, due to activation of the kynurenine pathway [
31,
32]. Of relevance also is the fact that kynurenine by the enzyme kynurenine-3-hydroxylase can be converted to 3-hydroxy-kynurenine, which, in addition to being a redox reactive metabolite, appears to act as a neurotoxin through its ability to induce protein modifications [
33]. In addition, activation of the kynurenine pathway appears to enhance the development of cardiovascular disease [
34,
35].
Until recent years, medical interest in tryptophan has focused mainly on its role in serotonin synthesis. In the CNS, serotonin modulates mood and cognition. Several neuropsychiatric problems have been attributed to changes in the availability of serotonin. The focus has currently changed, however, to other aspects of tryptophan metabolism such as the indole and kynurenine pathways. There is a delicate balance between different tryptophan pathways. It is now realised that only about 1–2% of tryptophan intake is metabolised into serotonin and approximately 95% is metabolised via the kynurenine pathway. Because the two metabolic pathways of serotonin and kynurenine compete for the substrate, tryptophan, increased metabolism of tryptophan via the kynurenine pathway may result in a relative deficiency of serotonin in the CNS. Thus, people vulnerable to stress may benefit from tryptophan supplements [
36].
Notably, immune activation accompanied by increased production of INFγ will increase both TDO and IDO activity and thereby channel the tryptophan metabolism into the kynurenine pathway. IDO oxidation stimulated by immune activation is apparently of significance for a variety of disorders, including neuropsychological impairments and diseases with vascular pathology [
11,
35].
3. Quinolinic Acid
Quinolinic acid [
37], also known as pyridine-2,3-dicarboxylic acid, is a dicarboxylic acid with a pyridine backbone—a downstream product of the kynurenine pathway (
Figure 1 and
Figure 2). It is known that quinolinic acid can act as an
N-methyl-
d-aspartate (NMDA) receptor agonist [
38,
39].
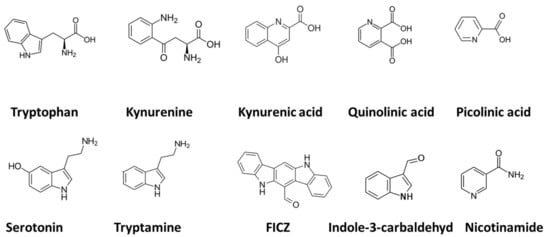
Figure 2. Chemical structures of tryptophan and derivatives mentioned in Figure 1. The term FICZ denotes the compound 6-formylindolo(3,2-b) carbazole.
Through its interaction with the NMDA receptor, quinolinic acid has potent neurotoxic effects. Studies have demonstrated that quinolinic acid may be involved in neurodegenerative processes in the brain, in addition to playing a role in mood disorders [
40,
41].
Quinolinic acid is produced in the brain by immune activation of microglia and macrophages, which contain the IDO enzyme that initiates the kynurenine pathway [
18,
42,
43,
44,
45]. According to Schwarcz et al. (2012), elevated quinolinic acid levels could also lead to axonal degeneration. Its neuroactive properties have been ascribed to its NMDA receptor agonism [
46]. It also acts as a pro-inflammatory mediator and as a pro-oxidative molecule [
47].
Quinolinic acid formed in the CNS is unable to escape through the blood–brain barrier (BBB). In contrast, the precursor of quinolinic acid, kynurenic acid (produced primarily in the liver), and tryptophan do pass, and can increase the CNS production of quinolinic acid. The ability of quinolinic acid to stimulate NMDA receptors may lead to excitatory neurotoxicity [
46]. In response to inflammation in the brain with the activation of microglia and macrophages, quinolinic acid may reach neurotoxic levels, which can lead to neuronal dysfunction. In addition to its NMDA receptor agonism, quinolinic acid can induce lipoperoxidation and cytoskeletal destabilisation [
48,
49]. Its toxicity specifically affects neurons located in the hippocampus, striatum, and neocortex, due to the selectivity of quinolinic acid toward NMDA receptors residing in these locations [
50].
When neuroinflammation flares up, quinolinic acid is produced in excessive amounts through the activated kynurenine pathway, leading to over-excitation of the NMDA receptors, secondarily leading to neuronal influx of Ca
2+. High levels of Ca
2+ in neurons trigger an activation of apoptotic pathways and cell death [
50].
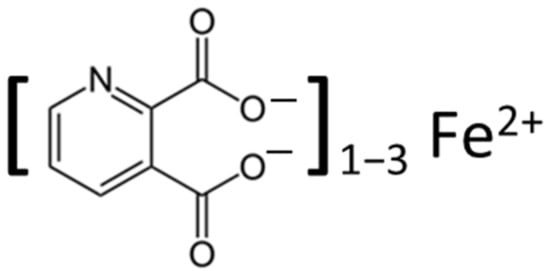
Through its interaction with Fe(II) (
Figure 3), with the formation of Fe(II)-quinolinate complexes (i.e., 1:1, 1:2, and 1:3 complexes), a subsequent interaction with oxygen and H
2O
2 can induce the formation of ROS, including the highly toxic hydroxyl radical
•OH [
49,
51]. This free radical causes significant oxidative stress, leading to increased glutamate release, and resulting in DNA damage and lipid peroxidation.
Figure 3. Chemical structure of the quinolinic acid iron complex. Vicinal oxygen groups (electron donors) in the molecule accounts for its coordination of Fe(II) [
52], and the Fe(II)-complex can, through interaction with dioxygen and H
2O
2, lead to ROS generation [
51,
52].
3.1. Mood Disorders: Depression
In post-mortem brains of patients who had suffered from major depression, the levels of quinolinic acid in the prefrontal cortex have been found to be greater than in post-mortem brains of patients without depression [
53]. Because NMDA receptor antagonists possess antidepressant properties, it is tempting to propose that increased levels of quinolinic acid in patients with depression may serve a causal or aggravating role in the mood disorder through the activation of NMDA receptors. Following INFα therapy, researchers have found increased concentrations of quinolinic acid in the cerebrospinal fluid (CSF) and have noted that the concentrations correlate with the severity of depressive symptoms [
53]. In addition, increased levels of quinolinic acid could play a role in impairment of the glial–neuronal network, which could be associated with the recurrent and chronic nature of bipolar depression [
54]. Based on results of a meta-analysis, Marx and co-workers (2021) have suggested that there is a shift in the tryptophan metabolism from serotonin to the kynurenine pathway in psychiatric diseases and that patients with mood disorders are characterised by a higher quinolinic-acid/kynurenic-acid ratio than people without mood disorders [
55]. Moreover, Brundin and co-workers (2016) found a higher quinolinic-acid/picolinic-acid ratio in the CSF of 137 patients who were exhibiting suicidal behaviour, as compared with the values in 71 healthy controls [
56]. They ascribed their observation to a reduction of an alternative kynurenine pathway metabolite, picolinic acid, that counteracts the neurotoxic action of quinolinic acid [
57]. The reduced concentrations of the protective metabolite, picolinic acid, in CSF were sustained over two years after a suicide attempt in depressive patients. Although kynurenic acid, another metabolite of kynurenine, was not assessed in the latter study [
57], it might have worked to counteract excessive NMDA receptor activation and exert a neuroprotective action [
58,
59,
60,
61]. An antidepressant effect of kynurenic acid is in accordance with the results from an experimental study in a rat model [
62].