Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
It quickly became obvious that emergency ultrasound, or point of care ultrasound (POCUS), has some very interesting aspects in the context of the emergency room (ER), allowing the physician to immediately obtain images of the patient during the first visit and thus rule out major pathologies immediately. Chest pain often is associated with dyspnea or shortness of breath (SOB), which is in itself one of the most common causes of emergency room access. The origin of these symptoms is often sought in heart and lung diseases.
- POCUS
- point of care ultrasound
- emergency medicine
- ultrasound
1. POCUS in Chest Pain: What Role Could It Have?
Over the last twenty years, ultrasound has gained growing importance in the emergency department. Initially, ultrasounds were usually performed on trauma patients to evaluate whether patients needed surgery when CT (computed tomography) scans were not as widely spread as they are now [1].
It quickly became obvious that emergency ultrasound, or point of care ultrasound (POCUS), has some very interesting aspects in the context of the emergency room (ER), allowing the physician to immediately obtain images of the patient during the first visit and thus rule out major pathologies immediately [2].
Ultrasound has gained popularity in many different conditions and clinical presentations, from critically ill patients [3] to patients with musculoskeletal pain [4].
While on the one hand ultrasound presents a number of advantages, it also presents some potential pitfalls, particularly because it is highly influenced by the operator’s ability to perform it [5].
However, particularly in overcrowded ERs, ultrasound can aid the emergency physician in the diagnosis and stratification of patients.
Chest pain is one of the main causes of admission to the emergency room, and it has been estimated that about 1 million people refer to the ER for this reason in Italy every year. It has been estimated that in about half of the cases the cause is cardiac, yet in the other half it is not [6]. While acute coronary syndrome (ACS) is the first cause that needs to be ruled out, there are a number of other conditions that can present with chest pain [7]. Additionally, the characterization of the pain, which should in theory aid the staff towards the correct diagnosis, is not reliable in a large number of patients due to a number of psychosocial and physiological factors [6].
2. Cardiac Causes
As discussed above, chest pain is the second most frequent cause of accessing the emergency room [7]. In case of suspicion of ischemic chest pain, the patient is evaluated with a 12-lead electrocardiogram and troponin dosage, which are necessary for the diagnosis of ACS [8]. In the event of major changes in the ECG (electrocardiogram) or troponin values, the patient is urgently evaluated by the cardiologist.
Once the diagnosis of ACS has been ruled out, there are many other cardiac clinical pictures in which the help of ultrasound can be decisive for the emergency room physician. There are, indeed, many other heart diseases that can occur in the emergency room with chest pain, such as aortic dissection, pericarditis, and pulmonary embolism.
The use of echocardiography by the emergency physician has several advantages, such as a targeted and early evaluation, and is rapid and non-invasive. However, this method, which has been spreading rapidly for several years, does not yet have a good degree of overall accuracy [9].
Another condition in which echocardiography can help the physician is the finding of hypoechoic material between the two layers of the pericardium, which allows researchers to make a diagnosis of pericardial effusion (Figure 1). Another advantage is that the ultrasound performed in the emergency room by the emergency doctor has a very high sensitivity (96%) and specificity (98%) towards this pathology [10].
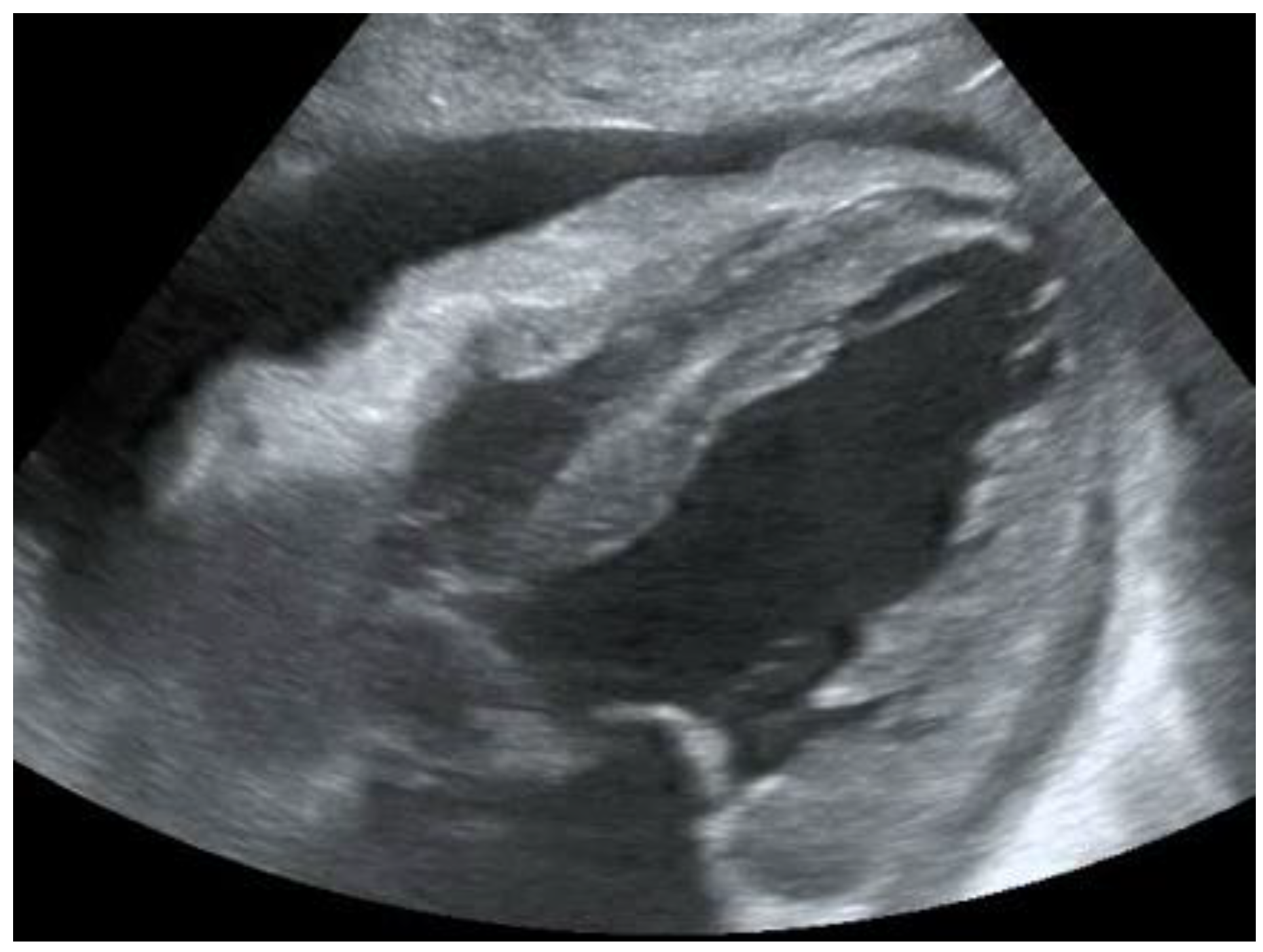 Figure 1. POCUS echocardiography: subcostal projection with pericardial effusion.
Figure 1. POCUS echocardiography: subcostal projection with pericardial effusion.Knowing how to identify a pericardial effusion also allows researchers to diagnose much more dangerous clinical pictures, such as cardiac tamponades [11].
Another condition characterized by chest pain which can often be similar to ischaemic pain is pulmonary embolism. Researchers will further discuss the role of POCUS in the diagnosis of pulmonary embolism in the chapter on thoracic ultrasound.
While researchers will discuss heart failure further in the chapter on thoracic POCUS, it is worth noting that the evaluation of the IVC (Figure 2) can help researchers in several respects, as its diameter and collapsibility reflect the systemic volume state (Table 1) [12][13].
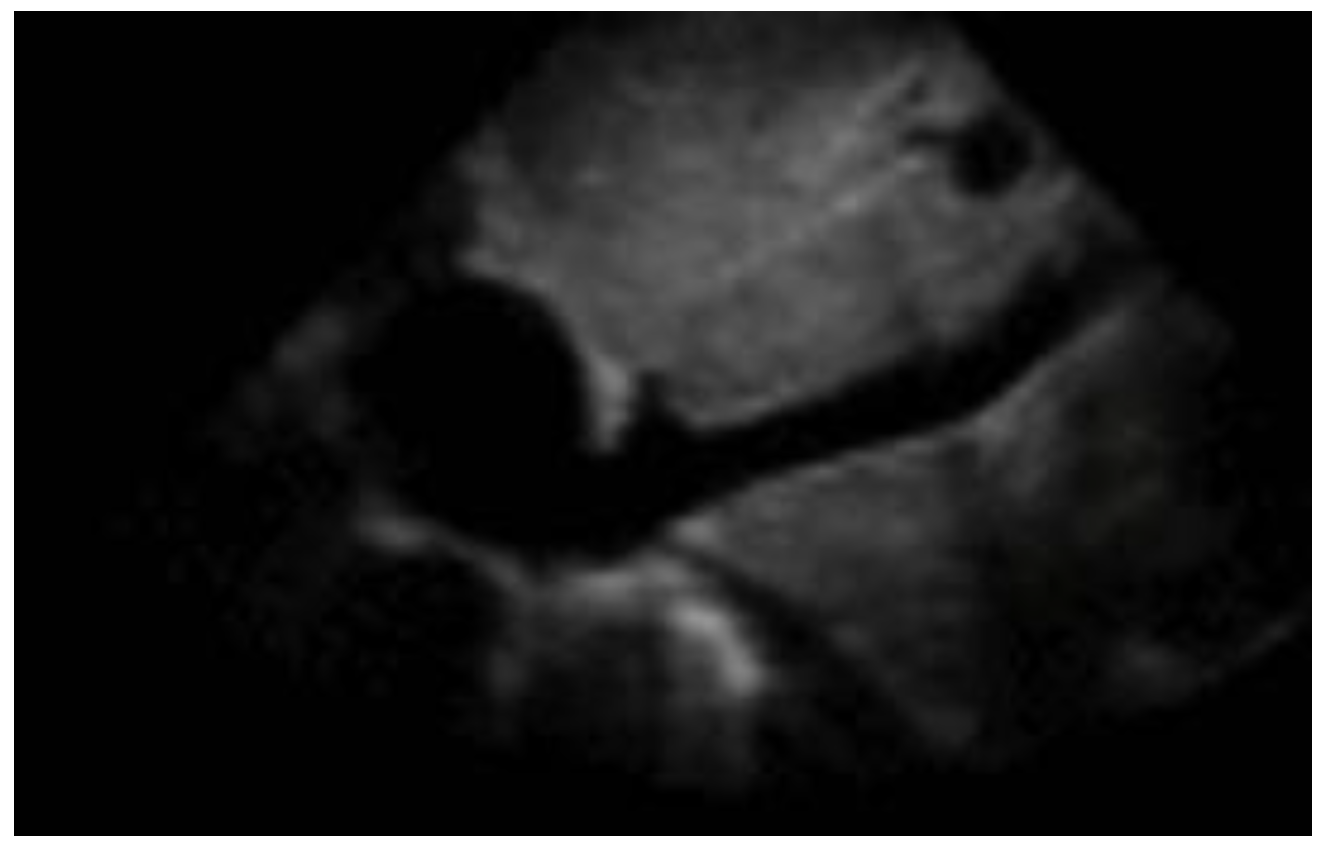 Figure 2. Subcostal longitudinal view: normal IVC.
Figure 2. Subcostal longitudinal view: normal IVC.Table 1. Relation between inferior vena cava diameter, inspiratory collapse and right atrium pressure.
| IVC Diameter | Inspiratory Collapse | Right Atrium Pressure |
|---|---|---|
| <2.1 cm | >50% | 3 mm Hg (range 0–5 mm Hg) |
| >2.1 cm | <50% | 15 mm Hg (range 10–20 mm Hg) |
A reduction in diameter accompanied by an increase in collapsibility orients us, for instance, towards a state of hypovolemia, while an increase in caliber and a smaller excursion during inspiration indicates congestion. For this reason, finding a congested IVC may suggest fluid overload and lead to a diagnosis of heart failure [14] (Figure 3).
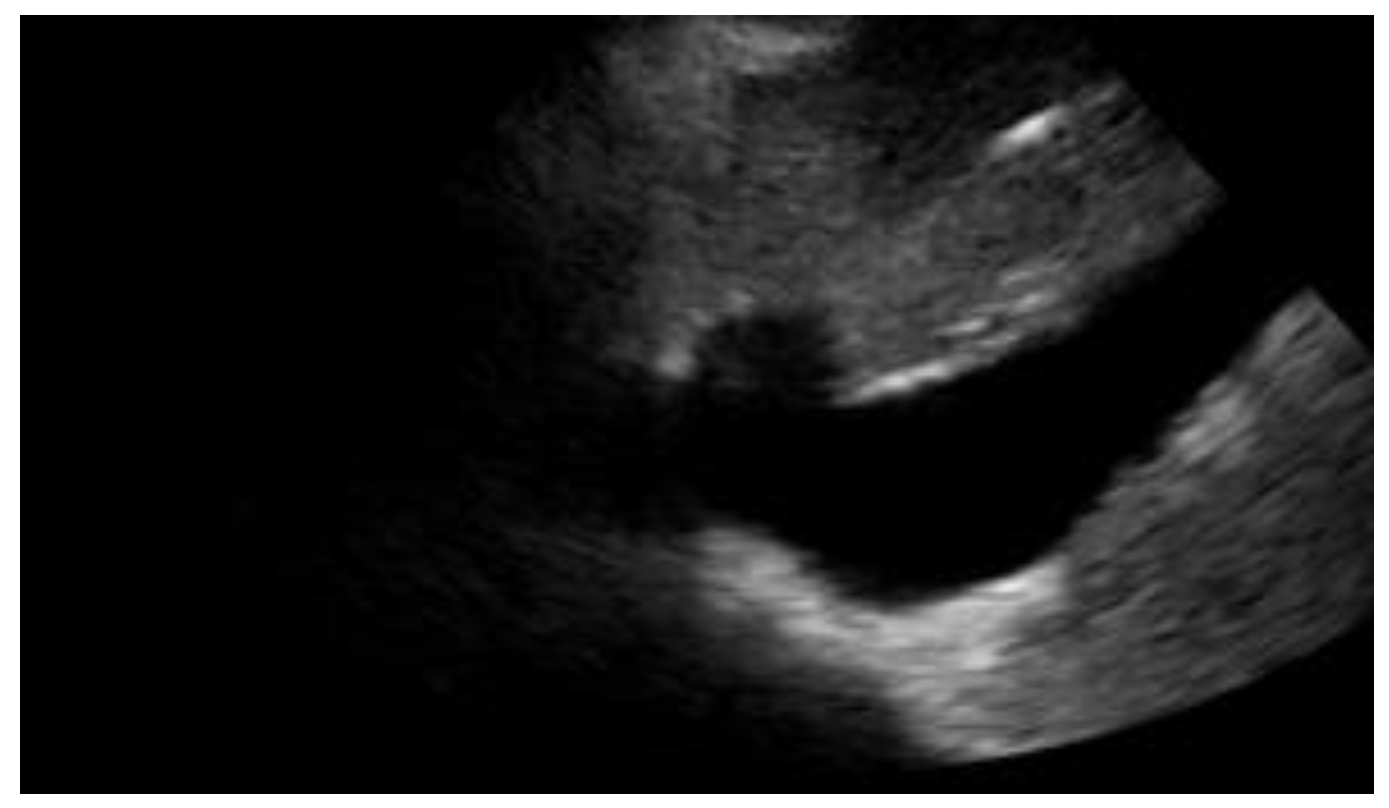 Figure 3. Subcostal longitudinal view: plethoric IVC. This finding suggests a state of fluid overload.
Figure 3. Subcostal longitudinal view: plethoric IVC. This finding suggests a state of fluid overload.Additionally, IVC volume can help the clinician in evaluating the patient’s response to a fluid challenge [15].
Cardiac POCUS can also aid physicians who examine patients with chest pain who go into cardiac arrest [16]. Indeed, ACS is not the only possible underlying cause in this research, and properly trained emergency room doctors should be able to conduct an appropriate ultrasound examination in patients experiencing cardiac arrest [17].
In this situation, conducting an ultrasound examination is of fundamental importance for several reasons, in particular because researchers could identify some reversible causes of the arrest, such as the presence of cardiac tamponade or pulmonary embolism [18].
In researchers' opinion, the use of POCUS (point-of-care ultrasound) by the emergency room physician therefore represents the future of emergency medicine.
In recent years, its use has progressively increased [19] and researchers have seen how fundamental it is in the evaluation of chest pain, in the differential diagnosis of cardiac pathologies, and in the correct management of cardiac arrest.
For the proper use of POCUS, the emergency physician must also be aware of its limitations, such as being a highly operator-dependent examination which does not possess the same diagnostic accuracy as more advanced imaging techniques such as CT and MR.
The primary care physician should not make the mistake of overestimating his or her own capabilities, but should interpret POCUS as a tool that can help him or her in the initial framing of the patient, relying on more accurate imaging techniques and specialist consultation in more complex cases.
Overall, cardiac POCUS can help the physician in evaluating the presence of pericardial effusion, the overdistension of the right ventricle, the presence of aortic dissection, and also the degree of collapse of the IVC and the ejection fraction [20] (Table 2).
Table 2. POCUS application in cardiac clinical pictures.
| Uses of Cardiac POCUS in the Emergency Department | |
|---|---|
| Disease | Assessment |
| Pulmonary embolism | Ejection fraction |
| Heart failure | Inferior vena cava filling |
| Aortic pathologies | |
| Pericardial effusion and cardiac tamponade | |
3. Chest Pain and Its Respiratory Causes
Chest pain often is associated with dyspnea or shortness of breath (SOB), which is in itself one of the most common causes of emergency room access. The origin of these symptoms is often sought in heart and lung diseases [21].
Patients presenting with these symptoms are routinely subjected to a chest X-ray examination, although in recent years researchers have witnessed the rapid growth and spread of thoracic POCUS, in which the physician himself, no longer the radiologist, performs the diagnostic examination.
One of the advantages includes knowing first-hand the clinical picture and, consequently, the symptoms reported by the patient. For this reason, it is easier to orientate towards the correct differential diagnosis [22].
It has been known for some time now that the application of this method also presents many advantages for the patient when it is applied for the research of the thorax, including a lower exposure to ionizing radiation, a greater speed of execution, and a reduction in cost [23].
One of the most well-established aspects of this approach is that integrating ultrasound into the normal diagnostic tests for patients who come to the emergency room for dyspnoea and chest pain improves diagnostic accuracy [24].
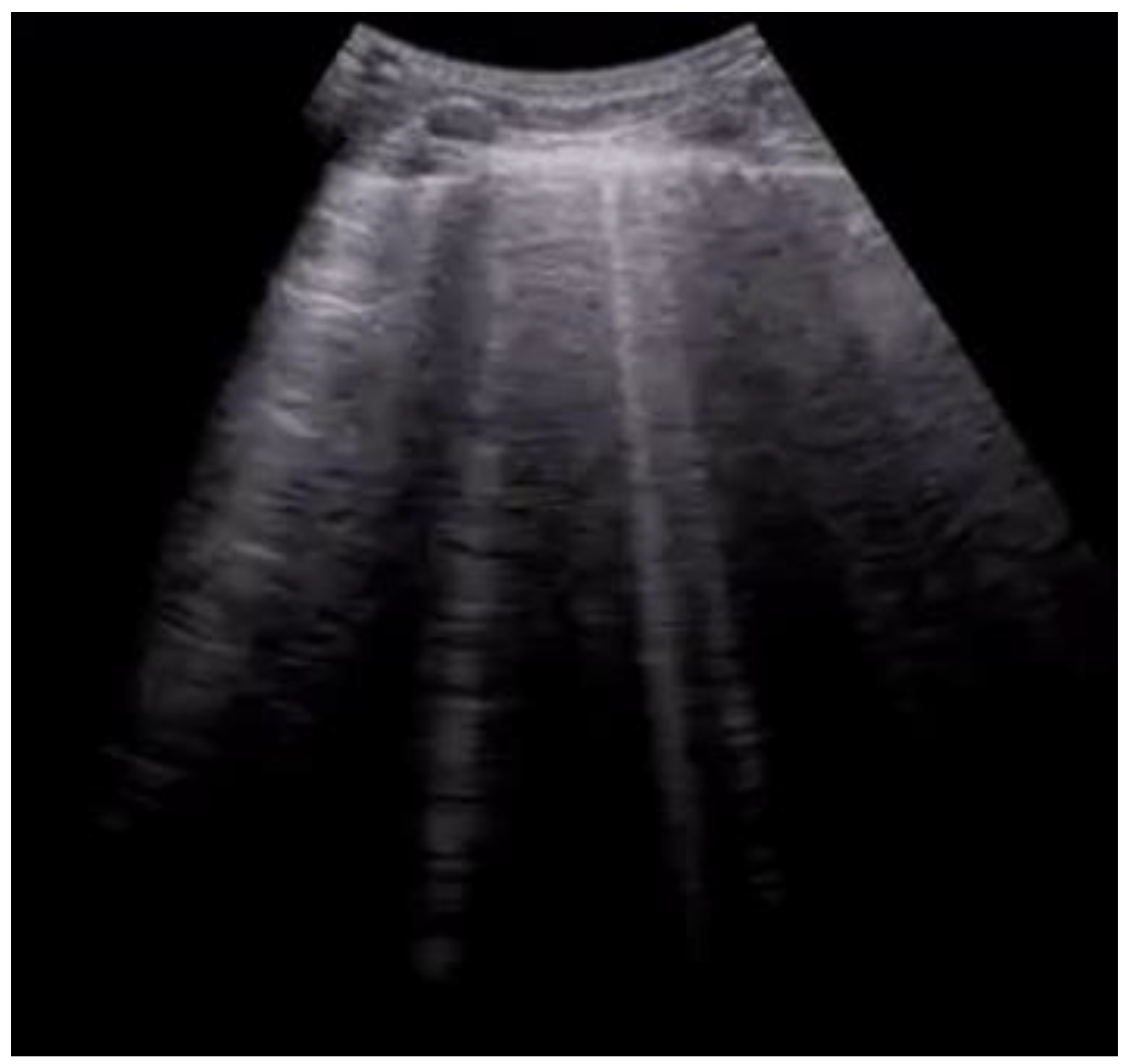 Figure 4. Longitudinal scan with evidence of B-lines: vertical artifacts perpendicular to the pleural line are indicative of inflammation or interstitial edema.
Figure 4. Longitudinal scan with evidence of B-lines: vertical artifacts perpendicular to the pleural line are indicative of inflammation or interstitial edema.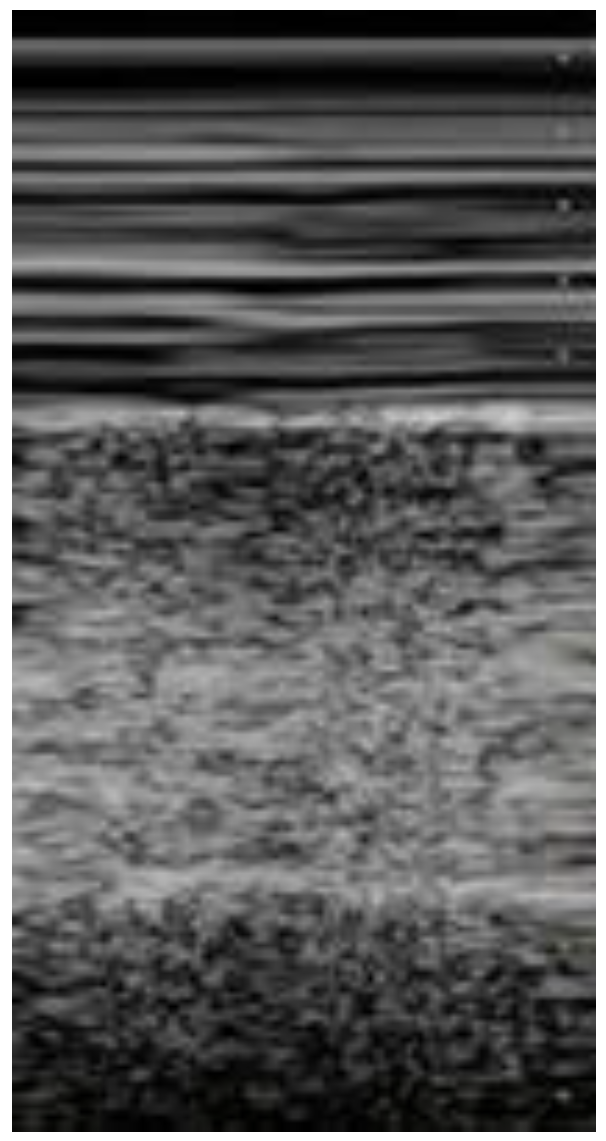 Figure 5. Lung ultrasonography, signs in motion mode (M-mode): seashore sign, indicative of the physiological sliding of the pleural line.
Figure 5. Lung ultrasonography, signs in motion mode (M-mode): seashore sign, indicative of the physiological sliding of the pleural line.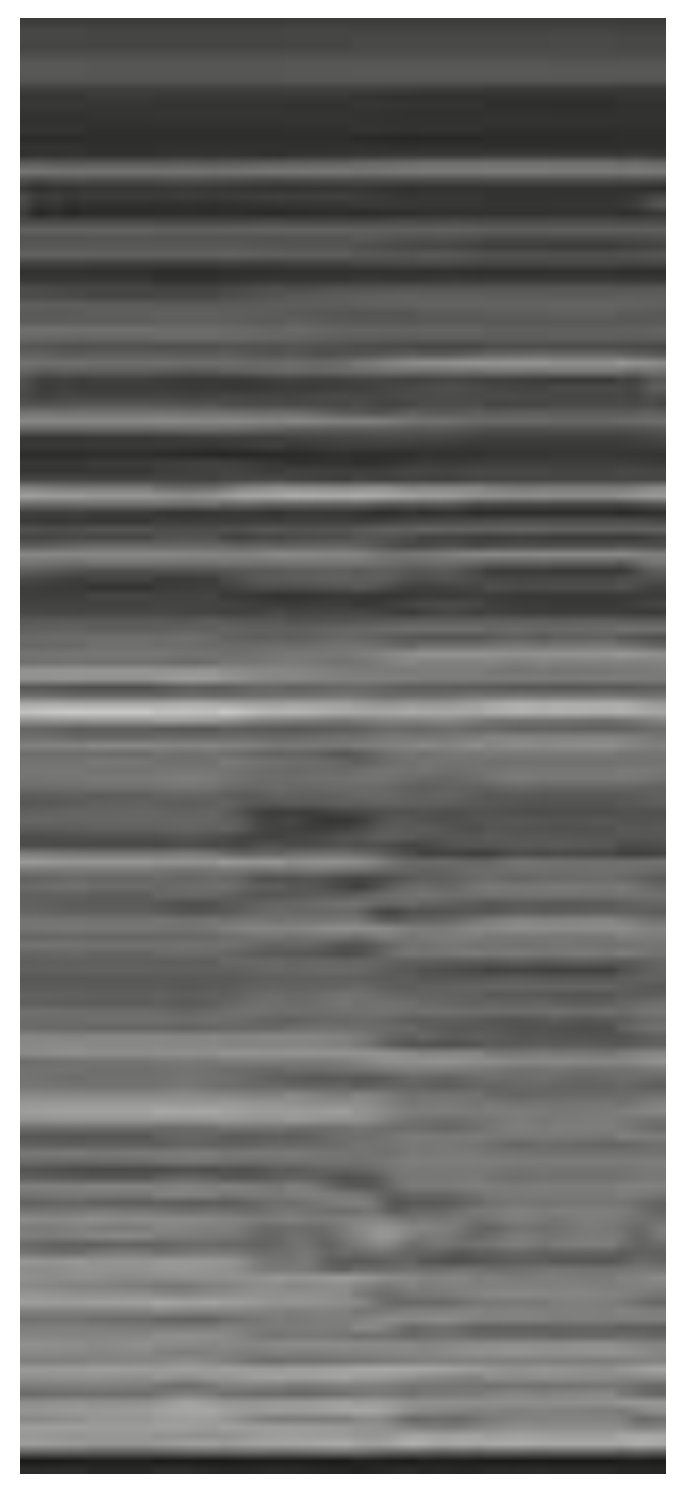 Figure 6. Lung ultrasonography, signs in motion mode (M-mode): barcode sign (sign of the stratosphere), no evidence of pleural sliding, a sign suggestive of pneumothorax.
Figure 6. Lung ultrasonography, signs in motion mode (M-mode): barcode sign (sign of the stratosphere), no evidence of pleural sliding, a sign suggestive of pneumothorax.There are numerous thoracic pathologies that can be identified with thoracic ultrasounds such as: pneumothorax, pleural effusion, pneumonia, pulmonary oedema and diaphragm dysfunction [25].
As discussed above, chest X-rays are routinely performed in the diagnostic evaluation of patients who come to the emergency room for chest pain and dyspnea, but numerous studies have shown that ultrasound is even superior to traditional radiology for the diagnosis of some clinical pictures [26][27][28][29].
With regard to pleural effusion, for instance, the greater diagnostic accuracy of thoracic ultrasound compared to X-rays in certain situations has been known for several years, both in terms of detecting it and quantifying it [28]. The most common method used in researchers' emergency department to estimate the amount of pleural effusion present is to calculate 90 mL for each centimeter of cranio-caudal extension of the effusion with the probe oriented longitudinally in the dorso-lateral wall in the patient in the standing or sitting position (first Goecke formula) [30].
The accuracy of the ultrasound method for the diagnosis of pneumothorax and haemothorax is also supported by numerous pieces of evidence; many of these studies were conducted in patients who came to the emergency room for trauma and then underwent E-FAST (Extended Focused Assessment with Sonography for Trauma).
FAST ultrasound examination was initially designed to evaluate free intra-abdominal effusions in trauma patients and quickly spread in all trauma centers; it was then integrated with further scans to assess the presence of pneumothorax and haemothorax, becoming E-FAST [31]. Thus, ultrasound has had a significant impact on the diagnosis of post-traumatic complications such as pneumothorax and haemothorax. The possible use of thoracic ultrasound for the identification of injuries such as post-traumatic haemothorax and pneumothorax was also carefully analyzed in a meta-analysis, which established its accurate diagnostic validity [32].
Thoracic POCUS has also gained importance in non-traumatic patients with a number of different conditions. A dangerous and prevalent condition in which the importance of POCUS is now consolidated with numerous pieces of evidence is the diagnosis of acute pulmonary oedema [33].
Ultrasound findings supporting the diagnosis of pulmonary embolism include the findings of subpleural infarction, the dilation of the right heart cavities or the presence of thrombus within them, and the presence of deep vein thrombosis. While the ultrasound cannot lead researchers to the diagnosis of pulmonary thromboembolism, the gold standard of which is recognized as angio-CT [34], it can still be useful in properly stratifying patients to determine if they need to undergo CT angiography [35].
Ultrasound is also extremely useful in patients presenting with chest pain, cough, fever and dyspnea. These symptoms, associated with the presence of risk factors and an increase in inflammatory markers, can guide researchers towards the diagnosis of pneumonia, for which ultrasound has a high sensitivity, specificity and accuracy [36]. In particular, in very young or pregnant patients, ultrasound represents a valid option in diagnosing pneumonia [37].
Chest ultrasounds in emergency departments were immediate and valuable aids in the clinical management of interstitial pneumonia due to COVID-19 [38]. Ultrasound could be useful to isolate both patients with suspected acute respiratory failure due to COVID-19 pending the outcome of the nasopharyngeal swab and those with suspected infection with a suspected false-negative molecular swab [39].
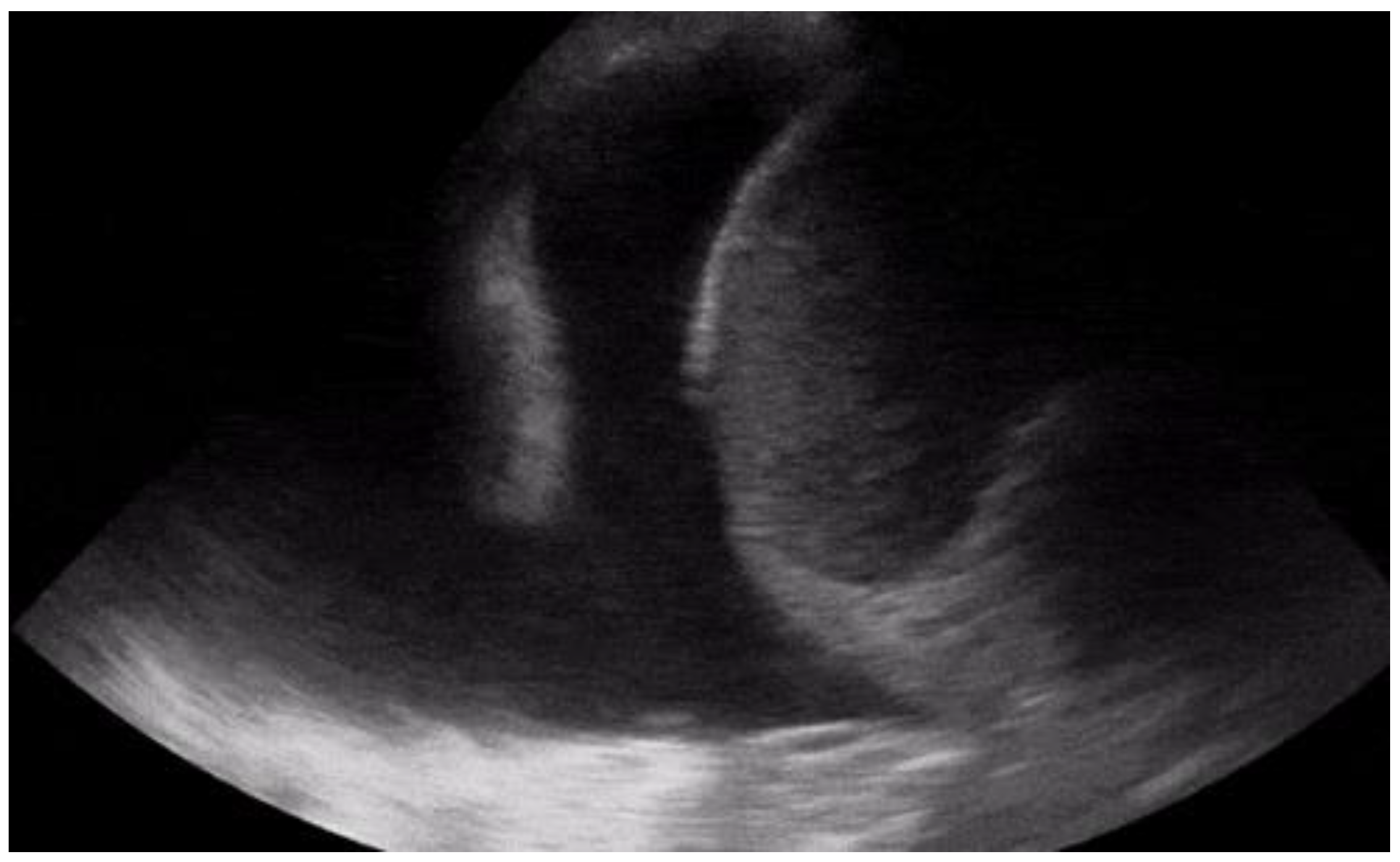 Figure 7. Longitudinal scan with presence of massive pleural effusion above the diaphragmatic line in pleural cavity, with atelectasis of adjacent lung parenchyma.
Figure 7. Longitudinal scan with presence of massive pleural effusion above the diaphragmatic line in pleural cavity, with atelectasis of adjacent lung parenchyma.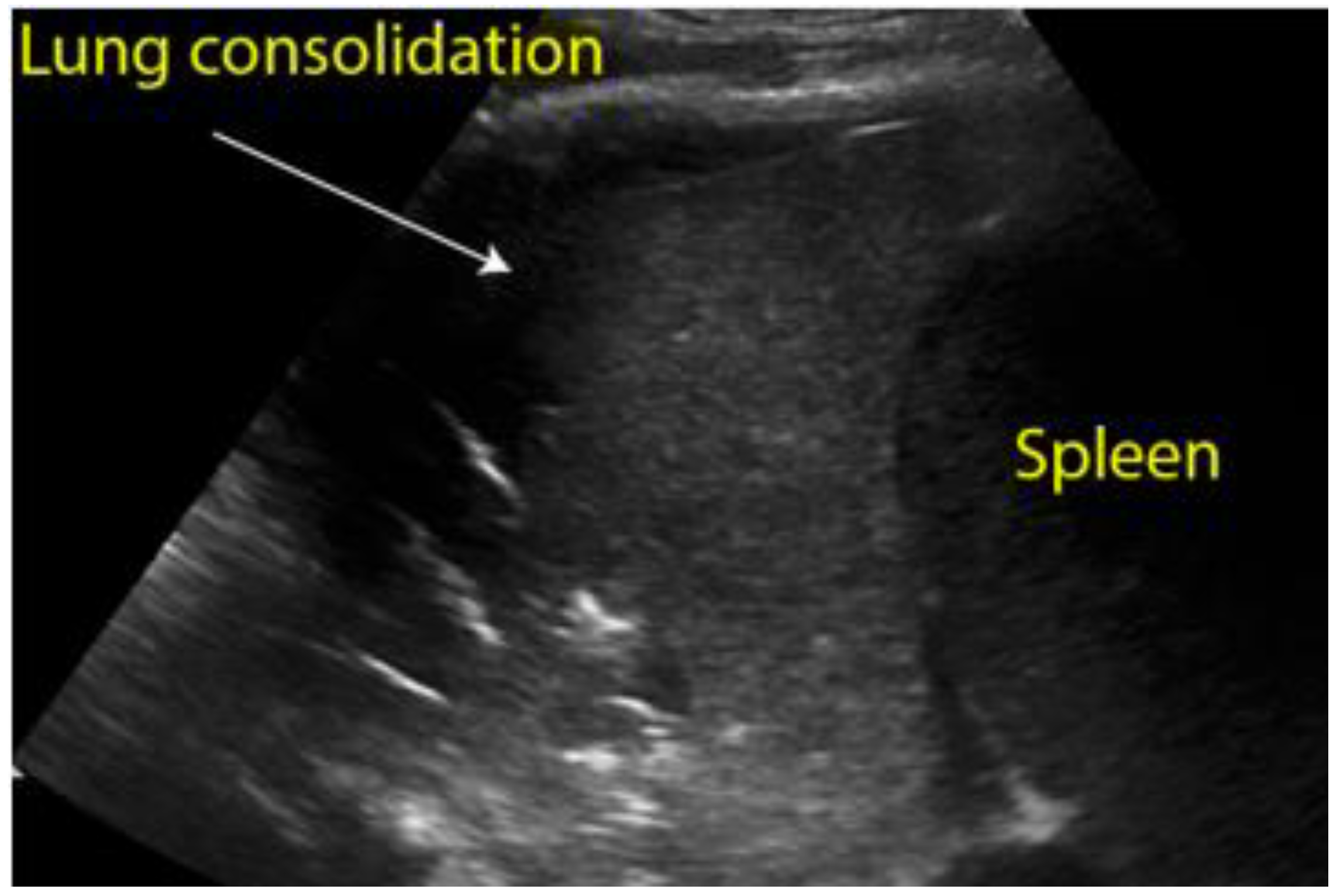 Figure 8. Longitudinal scan of left hypochondrium with presence of lung consolidation suggestive of pneumonia.
Figure 8. Longitudinal scan of left hypochondrium with presence of lung consolidation suggestive of pneumonia. Figure 9. Transverse scan, presence of diffuse B-lines over all fields (white lung) indicative of acute pulmonary edema.
Figure 9. Transverse scan, presence of diffuse B-lines over all fields (white lung) indicative of acute pulmonary edema.4. Abdominal Causes
Chest pain can sometimes be a manifestation of abdominal pathology. A common example of this is gastritis, which can present itself in a similar fashion to cardiac ischaemia, as epigastric tenderness or as pain resolution after the administration of proton pump inhibitors (PPIs). In association with a lack of risk factors, POCUS is often used to determine whether gastric disturbances can be the cause of chest pain. However, although uncommon, there have been cases of patients suffering from more severe diseases and conditions who were discharged with the diagnosis of gastritis, only to return shortly after to the attention of the emergency physicians [40][41].
Another condition in which chest pain can be the main symptom is esophagitis. The most common cause is gastroesophageal reflux disease (GERD), but infections and autoimmune diseases can also determine this disease. Similarly to gastritis, endoscopy cannot be replaced by ultrasound in the diagnosis, nor can it rule out the diagnosis; however, the presence of a thickened oesophageal wall can support the diagnosis [42].
Ultrasound may not be conclusive for the diagnosis of inflammatory disorders of the oesophagus and the stomach, but it can offer significant help in other more severe disorders; in particular, oesophageal perforation can result in the non-visualization of the heart on an ultrasound due to the presence of air, and free fluid may also be present in the upper abdominal quadrants [43]. A similar presentation may also be present in the case of gastric rupture, in which the hyper echogenicity of the right anterior extrarenal tissue (renal rind sign) may also be present [44].
This entry is adapted from the peer-reviewed paper 10.3390/diagnostics12071620
References
- Gleeson, T.; Blehar, D. Point-of-Care Ultrasound in Trauma. Semin. Ultrasound CT MR 2018, 39, 374–383.
- Sahlani, L.; Thompson, L.; Vira, A.; Panchal, A.R. Bedside ultrasound procedures: Musculoskeletal and non-musculoskeletal. Eur. J. Trauma Emerg. Surg. 2016, 42, 127–138.
- Perera, P.; Mailhot, T.; Riley, D.; Mandavia, D. The RUSH exam: Rapid Ultrasound in SHock in the evaluation of the critically lll. Emerg. Med. Clin. N. Am. 2010, 28, 29–56.
- Arnold, M.J.; Jonas, C.E.; Carter, R.E. Point-of-Care Ultrasonography. Am. Fam. Physician 2020, 101, 275–285.
- Wong, A.; Vieillard-Baron, A.; Malbrain, M. Emergency bedside ultrasound: Benefits as well as caution—Part 1. General. Curr. Opin. Crit. Care 2019, 25, 613–621.
- Lenfant, C. Chest pain of cardiac and noncardiac origin. Metabolism 2010, 59 (Suppl. 1), S41–S46.
- Chang, A.M.; Fischman, D.L.; Hollander, J.E. Evaluation of Chest Pain and Acute Coronary Syndromes. Cardiol. Clin. 2018, 36, 1–12.
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177.
- Tang, A.; Euerle, B. Emergency department ultrasound and echocardiography. Emerg. Med. Clin. N. Am. 2005, 23, 1179–1194.
- Chenkin, J.; Atzema, C.L. Contemporary Application of Point-of-Care Echocardiography in the Emergency Department. Can. J. Cardiol. 2018, 34, 109–116.
- Azarbal, A.; LeWinter, M.M. Pericardial Effusion. Cardiol. Clin. 2017, 35, 515–524.
- Ciozda, W.; Kedan, I.; Kehl, D.W.; Zimmer, R.; Khandwalla, R.; Kimchi, A. The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure. Cardiovasc. Ultrasound 2016, 14, 33.
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for Cardiac Chamber Quantification by Echocardiography in Adults: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14.
- Darwish, O.S.; Mahayni, A.; Kataria, S.; Zuniga, E.; Zhang, L.; Amin, A. Diagnosis of Acute Heart Failure Using Inferior Vena Cava Ultrasound: Systematic Review and Meta-analysis. J. Ultrasound Med. 2020, 39, 1367–1378.
- Orso, D.; Paoli, I.; Piani, T.; Cilenti, F.L.; Cristiani, L.; Guglielmo, N. Accuracy of Ultrasonographic Measurements of Inferior Vena Cava to Determine Fluid Responsiveness: A Systematic Review and Meta-Analysis. J. Intensive Care Med. 2020, 35, 354–363.
- Soar, J.; Böttiger, B.W.; Carli, P.; Couper, K.; Deakin, C.D.; Djärv, T.; Lott, C.; Olasveengen, T.; Paal, P.; Pellis, T.; et al. European Resuscitation Council Guidelines 2021: Adult advanced life support. Resuscitation 2021, 161, 115–151.
- Balderston, J.R.; You, A.X.; Evans, D.P.; Taylor, L.A.; Gertz, Z.M. Feasibility of focused cardiac ultrasound during cardiac arrest in the emergency department. Cardiovasc. Ultrasound 2021, 19, 19.
- Whitson, M.R.; Mayo, P.H. Ultrasonography in the emergency department. Crit. Care 2016, 20, 227.
- Amini, R.; Stolz, L.A.; Kartchner, J.Z.; Thompson, M.; Stea, N.; Hawbaker, N.; Joshi, R.; Adhikari, S. Bedside echo for chest pain: An algorithm for education and assessment. Adv. Med. Educ. Pract. 2016, 7, 293–300.
- Kennedy Hall, M.; Coffey, E.C.; Herbst, M.; Liu, R.; Pare, J.R.; Andrew Taylor, R.; Thomas, S.; Moore, C.L. The “5Es” of emergency physician-performed focused cardiac ultrasound: A protocol for rapid identification of effusion, ejection, equality, exit, and entrance. Acad. Emerg. Med. 2015, 22, 583–593.
- Shrestha, A.P.; Shrestha, R.; Shrestha, S.K.; Pradhan, A. Prevalence of Dyspnea among Patients Attending the Emergency Department of a Tertiary Care Hospital: A Descriptive Cross-sectional Study. JNMA J. Nepal. Med. Assoc. 2019, 57, 302–306.
- Bowra, J.; Duong, M.T. Point-of-care ultrasound in emergency department: Tips, tricks and controversies. Emerg. Med. Australas. 2020, 32, 155–157.
- De Luca, C.; Valentino, M.; Rimondi, M.R.; Branchini, M.; Baleni, M.C.; Barozzi, L. Use of chest sonography in acute-care radiology. J. Ultrasound 2008, 11, 125–134.
- Pirozzi, C.; Numis, F.G.; Pagano, A.; Melillo, P.; Copetti, R.; Schiraldi, F. Immediate versus delayed integrated point-of-care-ultrasonography to manage acute dyspnea in the emergency department. Crit. Ultrasound J. 2014, 6, 5.
- Wallbridge, P.; Steinfort, D.; Tay, T.R.; Irving, L.; Hew, M. Diagnostic chest ultrasound for acute respiratory failure. Respir. Med. 2018, 141, 26–36.
- Chan, K.K.; Joo, D.A.; McRae, A.D.; Takwoingi, Y.; Premji, Z.A.; Lang, E.; Wakai, A. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department. Cochrane Database Syst. Rev. 2020, 7, Cd013031.
- Ebrahimi, A.; Yousefifard, M.; Kazemi, H.M.; Rasouli, H.R.; Asady, H.; Jafari, A.M.; Hosseini, M. Diagnostic Accuracy of Chest Ultrasonography versus Chest Radiography for Identification of Pneumothorax: A Systematic Review and Meta-Analysis. Tanaffos 2014, 13, 29–40.
- Eibenberger, K.L.; Dock, W.I.; Ammann, M.E.; Dorffner, R.; Hörmann, M.F.; Grabenwöger, F. Quantification of pleural effusions: Sonography versus radiography. Radiology 1994, 191, 681–684.
- Maw, A.M.; Hassanin, A.; Ho, P.M.; McInnes, M.D.F.; Moss, A.; Juarez-Colunga, E.; Soni, N.J.; Miglioranza, M.H.; Platz, E.; DeSanto, K.; et al. Diagnostic Accuracy of Point-of-Care Lung Ultrasonography and Chest Radiography in Adults with Symptoms Suggestive of Acute Decompensated Heart Failure: A Systematic Review and Meta-analysis. JAMA Netw. Open 2019, 2, e190703.
- Ibitoye, B.O.; Idowu, B.M.; Ogunrombi, A.B.; Afolabi, B.I. Ultrasonographic quantification of pleural effusion: Comparison of four formulae. Ultrasonography 2018, 37, 254–260.
- Montoya, J.; Stawicki, S.P.; Evans, D.C.; Bahner, D.P.; Sparks, S.; Sharpe, R.P.; Cipolla, J. From FAST to E-FAST: An overview of the evolution of ultrasound-based traumatic injury assessment. Eur. J. Trauma Emerg. Surg. 2016, 42, 119–126.
- Staub, L.J.; Biscaro, R.R.M.; Kaszubowski, E.; Maurici, R. Chest ultrasonography for the emergency diagnosis of traumatic pneumothorax and haemothorax: A systematic review and meta-analysis. Injury 2018, 49, 457–466.
- Wang, Y.; Shen, Z.; Lu, X.; Zhen, Y.; Li, H. Sensitivity and specificity of ultrasound for the diagnosis of acute pulmonary edema: A systematic review and meta-analysis. Med. Ultrason. 2018, 1, 32–36.
- Estrada, Y.M.R.M.; Oldham, S.A. CTPA as the gold standard for the diagnosis of pulmonary embolism. Int. J. Comput. Assist. Radiol. Surg. 2011, 6, 557–563.
- Nazerian, P.; Vanni, S.; Volpicelli, G.; Gigli, C.; Zanobetti, M.; Bartolucci, M.; Ciavattone, A.; Lamorte, A.; Veltri, A.; Fabbri, A.; et al. Accuracy of point-of-care multiorgan ultrasonography for the diagnosis of pulmonary embolism. Chest 2014, 145, 950–957.
- Orso, D.; Guglielmo, N.; Copetti, R. Lung ultrasound in diagnosing pneumonia in the emergency department: A systematic review and meta-analysis. Eur. J. Emerg. Med. 2018, 25, 312–321.
- Giannella, L.; Catania, A.; Provaroni, A.; Cerami, L.B.; Chesi, G. The value of chest ultrasound along with inflammatory biomarkers in the management of pneumonia in a non-compliant pregnant woman. J. Matern. Fetal Neonatal Med. 2012, 25, 1830–1832.
- Smith, M.J.; Hayward, S.A.; Innes, S.M.; Miller, A.S.C. Point-of-care lung ultrasound in patients with COVID-19—A narrative review. Anaesthesia 2020, 75, 1096–1104.
- Jackson, K.; Butler, R.; Aujayeb, A. Lung ultrasound in the COVID-19 pandemic. Postgrad. Med. J. 2021, 97, 34–39.
- Boccardi, L.; Bisconti, C.; Camboni, C.; Chieffi, M.; Putini, R.L.; Macali, L.; Spina, A.; Lukic, V.; Ciferri, E. Chest pain in women: A multicenter study of the National Association of Hospital Cardiologists (ANMCO) of the Lazio Region. Ital. Heart J. Suppl. 2002, 3, 1034–1041.
- Ohtani, N.; Kiyokawa, K.; Asada, H.; Kawakami, T. Stanford type A acute dissection developing acute myocardial infarction. Jpn. J. Thorac. Cardiovasc. Surg. 2000, 48, 69–72.
- Mohammadi, A.; Sadreddini, M.; Sepehrvand, N.; Pedram, A.; Yarmohammadi, N.; Mladkova, N.; Ghasemi-Rad, M. Lack of utility of transabdominal ultrasound in the detection of gastroesophageal reflux disease-induced esophagitis in comparison with endoscopy. Ultrasound Q. 2011, 27, 121–125.
- Derr, C.; Drake, J.M. Esophageal rupture diagnosed with bedside ultrasound. Am. J. Emerg. Med. 2012, 30, 2093.e1–2093.e3.
- Coppolino, F.F.; Gatta, G.; Di Grezia, G.; Reginelli, A.; Iacobellis, F.; Vallone, G.; Giganti, M.; Genovese, E.A. Gastrointestinal perforation: Ultrasonographic diagnosis. Crit. Ultrasound J. 2013, 5, S4.
This entry is offline, you can click here to edit this entry!