Medical application materials must meet multiple requirements, and the designed material must mimic the structure, shape. and support the formation of the replacing tissue. Magnesium (Mg) and Zinc alloys (Zn), as a “smart” biodegradable material and as “the green engineering material in the 21st century”, have become an outstanding implant material due to their natural degradability, smart biocompatibility, and desirable mechanical properties. Magnesium and Zinc are recognized as the next generation of cardiovascular stents and bioresorbable scaffolds. At the same time, improving the properties and corrosion resistance of these alloys is an urgent challenge. particularly to promote the application of magnesium alloys. A relatively fast deterioration rate of magnesium-based materials generally results in premature mechanical integrity compromise and local hydrogen build-up, resulting in restricted applicability.
1. Introduction
Over recent years, there has been an exponential rise in the usage of biomaterials in medicine-based applications [
1]. Healthcare professionals and commissioners have been emphasizing early diagnosis and treatment of diseases and enhancing the efficiency of the available treatment strategies. This has been due to the more active lifestyle of the population, which significantly transformed the treatment of fatal diseases and conditions. However, there exists a requirement of affordable healthcare resources for the active aging generation. The longevity of an implanted biomaterial depends on the anchorage and integration between the implant and the living bone [
2]. There are various factors that determine the success of an implanted biomaterial, namely the form and structural characterization, stability, mechanical-loading, material property, location of the implanted site, and host response [
3,
4]. The key outcome is to finally derive a matrix that matches the bone in composition, structure, and properties [
5]. Biocompatibility and mechanical strength are the essential pre-requisite characteristics of any implanted biomaterial to be employed for biomedical, orthopedic, and dental applications [
6,
7,
8,
9,
10].
The inert metals, such as stainless steel, titanium, and cobalt alloys, having superior corrosion resistance and mechanical properties (concerning biological tissues) have been traditionally used as implant materials for cardiovascular and orthopedic applications [
11,
12,
13]. Liu et al. [
14] constructed a novel stromal cell-derived factor-1α (SDF-1α)/laminin-loaded nanocoating on the 316 L stainless steel (SS) surface to provide improved function in the modulation of vascular remodeling. The modified surface was found to control the delivery of biomolecules and exhibit promising potential to provide stage-adjusted treatment after injury. Furthermore, an in vitro biocompatibility study suggested that the constructed layer may effectively prevent thrombosis formation by inhibiting platelet adhesion and activation, while accelerating endothelium regeneration by inducing endothelial cell (EC) migration and endothelial progenitor cell (EPC) aggregation. An in vivo animal test further demonstrated that the nanocoating may prevent thrombus and neointimal hyperplasia after implantation for 3 months [
14]. Presently, these metallic implants are mainly designed for permanent tissue replacement, but they do not account for cases where only temporary support is required. There have been numerous difficulties involved, some of which are the stress-shielding effect over a while, which then leads to bone-weakening and distortion of diagnostic images. Finally, additional surgery is required for removal of the implant when these permanent metallic implants are used [
15,
16]. Extensive research efforts are ongoing to develop materials that can be used as temporary implants in the human body to perform multiple functions, depending on the nature of the ailment. Among the metals, Zinc (Zn)- and Magnesium (Mg)-based materials have garnered significant attention in recent years to serve as temporary implants [
17]. Magnesium and its alloys exhibit superior strength, ductility, and degradability compared to its biodegradable counterparts, Zinc and Iron [
17]. The elastic modulus (∼45 GPa) of magnesium is close to that of human bone (∼10–20 GPa), and this helps to avoid stress shielding effects compared to other metallic biomaterials [
18,
19]. The magnesium in plasma exists as Mg
2+ in a concentration of 1.2–1.4 mM and is excreted in urine [
20,
21]. Increased local degradation of Mg (and its alloys) causes increased hydrogen gas release from the implanted site, leading to an increase in pH [
20]. This increase in hydrogen gas evolution and pH causes localized cell death and cytotoxic reactions, which further leads to failure [
22,
23,
24]. For implanted devices, such as in orthopedics, where it is poorly vascularized, the accumulation of hydrogen gas is a safety concern as a gas embolism may potentially block the bloodstream, causing fatalities [
25]. For coronary stents, the gas generated is of not a large concern, as it can be removed by convective transport phenomena due to a high amount of blood flow at the implantation site [
26]. Nevertheless, it has been reported that the addition of Zn to Mg can significantly decrease the amount of hydrogen generated.
The favorable degradation behavior of Zn has led to the emergence and development of Zn-based alloys in recent years [
22,
27]. Being an essential element, Zn is involved in various biological processes, including being a metabolite for nucleic acid, signal transduction, and gene expression, and it takes part in interactions with a range of organic ligands and apoptosis coordination [
28]. Zn does not corrode as quickly as Mg and the corrosion of pure Zn is known to be moderate [
29]. However, Zn on its own has inferior mechanical properties with a tensile strength as low as 20 MPa, Vicker hardness of 3.7 and elongation of 0.2%. and these translate to relatively lower material strength as compared to its metallic counterparts [
22]. Thus, alloying of Zn is crucial for its application in load-bearing implants. There have been several new opportunities and difficulties in the development of Mg and Zn alloys for cardiovascular applications and to overcome the drawbacks of hydrogen gas evolution [
29].
2. Driving Force for Temporary Implants
There are broadly two types of implants that are used in the body: permanent implants and temporary implants. Permanent implants refer to implants that are intended to stay in the body throughout life, such as the one used for hip and knee replacement sand artificial tooths and their fixation. Then, there are temporary implants, which are not required in the body after a certain period when the injury is healed. This is applicable for orthopedics fixation purposes (plates and screws) and in cardiovascular (stents) application. The use of temporary implants helps in:
-
Avoiding revision surgery for the patient.
-
Minimizing medical costs for the patient.
-
Minimizing patient trauma inflicted during the second surgery.
-
Saving the doctor’s time.
-
Avoid long-term toxicity effects if a permanent implant material is used instead.
Commonly used implant materials used in the past as both temporary and permanent implant applications are [
30]
Given the disadvantages associated with using permanent implants for temporary functionality required by the human body, extensive research has been carried out to develop Magnesium- and Zinc-based materials in recent years. For any biodegradable materials to serve as a temporary implant, it must meet the following requirements [
30,
31,
32]
-
Biocompatible with acceptable or zero cytotoxicity.
-
No chronic deleterious effect.
-
To maintain mechanical integrity during the healing time.
-
Minimal stress-shielding effect.
-
Acceptable degradation time, synchronized closely with healing time.
The body should be able to metabolize or excrete corrosion products arising from temporary implants.
3. Cardiovascular Applications of Biodegradable Magnesium and Zinc Based Materials
3.1. Criteria for Biodegradable Vascular Stents
Stents are the most common cardiovascular application of biodegradable metals. The three significant conditions that need to be satisfied by a bioresorbable vascular scaffold (BVS) are mechanical properties, vascular biocompatibility, and degradation [
58]. The stent should not fail during service, and elastic recoil on expansion must be avoided from the mechanical outlook [
59]. Biocompatibility is also dependent on the solubility of the material in bio-fluids and the toxicity of the degradation products. The stent must also be conducive to cell attachment while simultaneously inhibiting excessive cell growth. This might cause in-stent restenosis (ISR). Furthermore, there should not be any release of toxic ions from the implant surface, as these toxic ions lead to severe inflammatory reactions. Ideally, the stent must degrade by less than 0.2 mm/yr to avoid the excessive release of degradation products, which may have long-term effects [
60].
3.1.1. Traditional Stents
From a purely mechanical standpoint, traditional materials such as 316 L stainless steel, Co-Cr alloys are ideal choices for stent materials. However, when these metallic systems were uncoated, it was reported that it could lead to ISR [
61] due to the release of Ni ions, leading to the inflammatory response [
62]. This scenario was commonly observed where repeated procedures were conducted [
63]. To reduce the occurrence of ISR, drug-eluting stents (DES) were designed, which eluted an antiproliferative drug from its surface. Despite the coating, incidences of late stent thrombosis were reported [
64]. The mechanical support in the artery may not be essential for more extended periods, as the remodeling of the artery takes place six months after implantation [
65]. A device which can assure mechanical support during the initial six months after implantation and get absorbed by the body [
66] will significantly reduce any post-operative complications.
3.1.2. Required Mechanical Properties
The essential mechanical criteria for qualifying a stent for favorable clinical results are biocompatibility, flexibility, easy deployability, greater radial strength, minimal crossing profile, low metallic surface area, and acceptable tractability. In the case of metallic stents, the following decisive factors are to be considered: construction, geometry, and strut thickness. The construction of metallic stents is of three types: (a) the coil type, (b) the tubular mesh type, and (c) the plain tubular type. The plain tubular type can be a modular tube or a slotted tube. On the other hand, coil stents are made of metallic stripes wound in a coil-like shape. Finally, the tubular mesh stent is made using a mesh in a tubular shape employing metallic wires. Slotted tube stents are made using metal tubes with a laser-cut design. Among the above-mentioned stent construction types, the slotted tube stent construction shows better radial strength and clinical outcomes compared to coil and mesh type stents. The modular stent construction is also suitable, as it possesses the optimum characteristics of the flexibility of coil type and the radial strength of the slotted tube design [
67,
68].
The geometry and physical construction of the stent plays a vital role in restenosis. The greater the number of strut-strut intersections, the greater is the rise in the neointimal region. Hence a lower number of intersections is preferred to minimize vascular injuries. In addition to these considerations, the stents also are designed considering restenosis for better clinical results. The thickness of the stent strut is an essential parameter in the stent design. The stents are categorized based on thickness as (a) thick (>120 μm), (b) intermediate (101–120 μm), (c) thin (81–100 μm), and (d) ultrathin (60–80 μm). Among them, the thinner struts have lower restenosis rates and better deliverability. To improve radial strength, arterial wall support, and radio-visibility, the intermediate thickness struts can be chosen. However, this would cause more intimal hyperplasia and vascular injuries resulting in a higher risk of restenosis when compared to thinner struts. For optimum radial strength and radio-visibility with better scaffolding properties, new materials and processes are needed [
67,
68].
The standard vascular stent is made of Stainless Steel (SS) 316 L, which gives optimum performance. The permanent SS-316L stent lasts for 10 years, with about 400 million cycles. The BVS requirements are satisfied by a biodegradable stent that retains its mechanical properties for six months, with 20 million cycles before failure [
69,
70,
71]. The mechanical characteristics of the candidate stent material should be comparable to that of SS 316 L, which includes Young’s modulus (YM), ultimate tensile strength (UTS), yield strength (YS), and elongation. These basic mechanical properties manifest into radial strength, axial and radial flexibility, acute and chronic recoil, profile, deliverability, and integrity during its lifetime [
72]. Materials having a lower YS and higher UTS are preferred for cardiovascular stents. Low yield strength is required to allow the balloon to expand at lower pressures, while a higher yield strength with high elastic deformation may result in acute recoil during the balloon expansion. Usually, materials having a high UTS also have a high YS. There have also been no criteria set thus far for cyclic fatigue for BVS materials [
73].
3.2. Magnesium Stents
Magnesium plays a crucial role in the functioning of the human body, as it is involved in various regulatory mechanisms [
74]. The poor mechanical properties of pure Mg relative to pure iron and its poor corrosion resistance make it a less favorable candidate [
58,
75]. The studies on AE21 and WE43 alloys showed that these alloys degrade in vivo and in pre-clinical studies very rapidly. as they exhibit localized corrosion caused by the disintegration of the passive protective film [
76]
3.2.1. Mechanical Properties
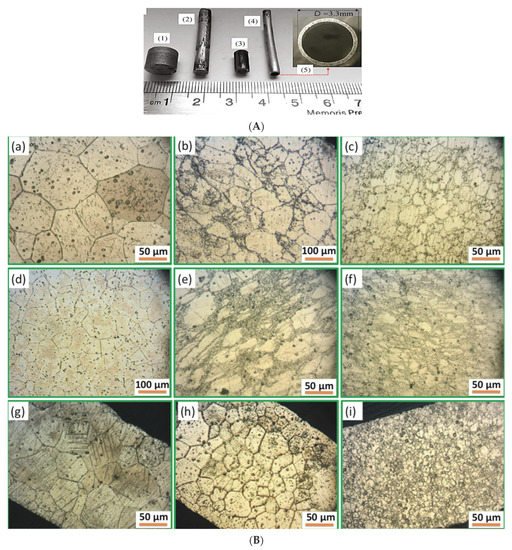
Magnesium alloys are mechanically inferior to 316L SS. Consequently, processing methodologies, such as deformation and alloying, must be used to enhance the mechanical characteristics. Alloying elements like Nd, Zr, Y, Zn, Al, and Ca can be used in small amounts for improving mechanical behavior. Mg alloys typically exhibit a hexagonal close-packed (HCP) structure with three slip planes and, hence, are difficult to deform. However, once deformed, they exhibit better mechanical properties. Hence, deformation techniques, such as extrusion and drawing, have also been explored (
Figure 1,
Table 2) [
68].
3.2.2. Biocompatibility and Degradation
Since Mg alloys have a higher rate of degradation, coatings with poly(carbonate urethane) urea (PCUU), poly(ester urethane) urea (PEUU), and poly(lactic-co-glycolic acid) (PLGA) are effective in controlling the degradation rate. Magnesium itself is an essential element for human metabolism, with a tolerance level of up to 121 mg/L in blood [
68]. Gao et al. [
77] evaluated the corrosion and biocompatibility of magnesium alloys by depositing a Chitosan-Functionalized Graphene Oxide/Heparin (GOCS) bioactive multilayer coating on the magnesium alloy surface layer-by-layer to construct the positively charged GOCS and negatively charged heparin. The results showed that the corrosion resistance of the magnesium alloy was significantly improved by GOCS/Heparin multilayers. The GOCS/Heparin multilayer coating had good blood compatibility and significantly reduced the homolysis rate of magnesium alloy [
77]. Zhang et al. [
78] surface-modified magnesium alloys by treating them with NaOH to form a passive chemical conversion layer followed by 16-Phosphonohexadecanoic acid (16-Pho) introduction on the modified surface to improve the acute corrosion resistance. Further, the biocompatibility of the magnesium alloys was improved by Poly (ethylene glycol) (PEG), fibronectin (Fn), and fibronectin/heparin (FH). The results of the study showed improvement in corrosion resistance and hydrophilicity by alkali heat treatment. Better corrosion resistance was clearly observed after the following immobilization of the molecules. Surface modifications with Fn and FH effectively enhanced cell attachment and growth and showed good cytocompatibility to endothelial cells [
78]. Pan et al. [
79] surface-modified a magnesium alloy (AZ31B) modified by the alkali heating treatment followed by the self-assembly of 3-phosphonopropionic acid, 3-aminopropyltrimethoxysilane (APTMS), and dopamine representatives to control the corrosion rate of Mg-based alloys and to enhance the biocompatibility. The results showed excellent hydrophilic surface, and the water contact angle increased to some degree after the self-assembly of dopamine, APTMS, and 3-phosphonopropionic acid. The alkali heating treatment formed a passivation layer, thereby forming the corrosion resistance of the magnesium [
79].
3.3. Zinc Stents
3.3.1. Degradation
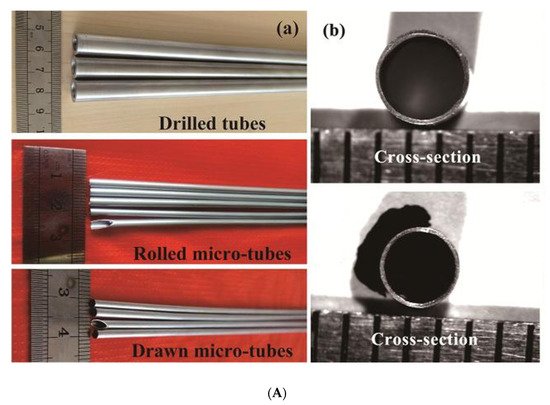
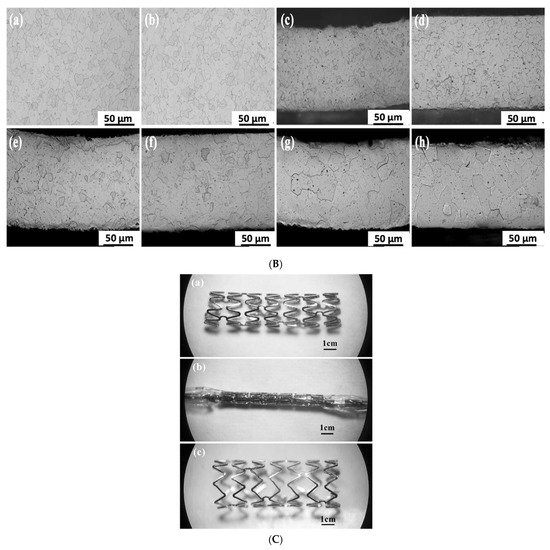
The research interest of Zinc alloys as a suitable cardiovascular stent material is relatively recent, compared to Mg and Fe. The degradation behavior of Zinc alloys is highly favorable. In a study, the abdominal aorta of rats was implanted with Zinc wires. The wires exhibited increasing degradation with time, as is required [
81]. For up to 20 months, the cross-sectional area of the wire decreased steadily [
82]. A new experiment revealed that in adult rabbits, the degradation of Zn stents was about 42 ± 30% over 12 months [
83]. Despite such promising degradation data, the mechanical properties of pure Zinc are not suitable for use as cardiovascular stents [
84,
85] (
Figure 2).
3.3.2. Mechanical Properties
The strength of pure Zinc is unfavorable for use as a cardiovascular stent. Since Zn has a hexagonal close-packed (HCP) structure, it is hard to deform. Consequently, the addition of alloying elements is a suitable strengthening method for Zn. The addition of several alloying elements like Mg [
86,
87,
88], Ca and Sr [
89,
90], Al [
85], and Mn [
91] to Zn was investigated to overcome the mechanical deficiencies. However, the main drawback of these systems is the strain-softening exhibited within the plastic range. This is a well-known occurrence in Zn and its alloys [
92]. The residual strength of alloys is reduced due to strain softening, which can increase the chances of late recoil in the implants. Ag is a possible candidate for an alloying element in Zinc, as it has been reported to increase both ductility and strength, with a reduction in strain-softening [
88]. There are avenues for further research with regards to hemocompatibility and cytocompatibility to check the effects of Ag [
88].
This entry is adapted from the peer-reviewed paper 10.3390/met12060999