1. Nutritional Status in Children with Cancer
Nutritional status is the biochemical, structural, and functional state of the body resulting from the level of coverage of energy and nutrient requirements and the action of factors influencing absorption and metabolism [
6]. In children diagnosed with cancer, the nutritional status is one of the prognostic values influencing treatment tolerance, quality of life, drug metabolism, and overall survival [
4,
10,
11,
12]. Malnutrition and overweight may occur at diagnosis or appear during and after oncological therapy but should not be treated as a normal condition at any stage of treatment. Despite the growing interest in this topic, malnutrition among cancer patients remains a serious problem, ranging between 40–90% in lower-middle-income countries and between 0–30% in high-income countries [
3]. This value varies depending on the type and stage of cancer, phase of treatment, and assessment method [
4]. In addition, patients with high-risk treatment protocols are more likely to be malnourished [
13,
14]. During oncological treatment, in some types of cancer, weight gain is also observed. According to Iniesta R. et al. [
15], the prevalence of overnutrition ranged from 8% to 78%. It is believed that the first nutritional status assessment has to be performed at diagnosis and should be repeated regularly during treatment [
4,
13]. The most noticeable changes in the nutritional status occur in the first months after diagnosis [
13,
16]. In a prospective study, Paciarotti et al. [
17] have shown that after the first three months of treatment, the content of adipose tissue in children with leukemia increased to 130% of the norm, while in children diagnosed with other cancer, it decreased from 78% at diagnosis to 70% of the norm after three months of treatment. Furthermore, weight loss of >5% in the first 3 months of treatment and >10% after 6 months were associated with poorer survival [
12].
1.1. Nutritional Disorders in Children Diagnosed with Various Types of Cancer
1.1.1. Leukemia
Leukemia is the most common childhood cancer [
1]. Studies show that obesity and undernutrition are associated with worse survival in children with acute myeloid leukemia (AML) [
18]. Moreover, a higher BMI at diagnosis was associated with worse event-free survival (EFS), poorer overall survival (OS), and higher mortality in children with AML and those with acute lymphoblastic leukemia (ALL) [
19,
20,
21,
22]. On the other hand, Orgel E. et al. [
23] showed that BMI at diagnosis wasn’t as important as underweight and obesity occurring more than half of the time between induction and maintenance. Studies also indicate that obesity during induction increases the risk of persistent minimal residual disease (MRD) [
24]. However, some studies do not confirm the relationship between BMI and EFS [
25], MRD [
26], and increased risk of recurrence [
27,
28].
It is also worth noting that children with leukemia are at risk of low muscle mass. Suzuki D et al. [
29] have assessed the content of skeletal muscle in patients with ALL using CT imaging at the L3 level. Skeletal muscle loss was demonstrated in all patients after the induction, while sarcopenia developed in almost 30% of the study group [
29].
1.1.2. Solid Tumors
It is difficult to unequivocally define the prevalence of nutritional disorders in children with solid tumors due to the varied results of individual studies resulting from different methods and times of nutritional assessment, as well as a different selection of the study group [
3]. It is believed that the risk of malnutrition in children with solid tumors is higher compared to other types of childhood cancers [
13,
30,
31,
32,
33], although not all studies confirm this [
34,
35]. Studies indicate that both too high and low BMI is associated with worse OS [
36,
37], worse response to treatment [
38], and a higher risk of toxicity [
39] and complications [
40]. On the other hand, Sharib JM. et al. [
38] do not point to malnutrition as a factor associated with increased treatment toxicity. Tenardi R et al. [
41] carried out a retrospective assessment of the nutritional status of children with Ewing sarcoma and osteosarcoma, where a high risk of experiencing extreme body changes was observed [
41]. Burke [
42] observed that the loss of >10% of body weight was associated with an increased number of days of hospitalization [
42]. Lifson L.F. et al. [
43] have shown that malnutrition in children with Wilms’ tumor reaches 66%, but no statistically significant relationship was found between nutritional status and survival [
44,
45]. In children with neuroblastoma, malnutrition is noticeable at diagnosis, and BMI decreases after 6 months of treatment, but no relationship has been found between BMI and survival [
45]. In a prospective study by Avarnival et al. [
46], it has been shown that the BMI of children with solid tumors decreased during the first 6 months of treatment and then gradually increased. It should be emphasized that the risk of malnutrition in children with solid tumors differs depending on the type of nutritional assessment method used. Children with solid tumors have a higher risk of malnutrition, regarding the MUAC, TSFT, and AMC indicators, compared to other methods [
47]. This is caused by the tumor mass masking the real body weight, which impairs seemingly correct BMI measurements [
47]. That is why it is so important to use measurements employing arm anthropometry, bioimpedance, or, if possible, DXA for these children. Furthermore, Joffe L. et al. [
48] demonstrated by using single-slice T12-L1 images from routinely obtained chest CT scans that children with solid tumors lose skeletal muscle and fat in the early stages of therapy.
1.1.3. Central Nervous System (CNS) Tumors
Brain tumors are the second most common cancer in children after leukemia [
1]. Tsutsumi et al. [
49] have estimated that at diagnosis, 6.7% of children with CNS tumors were malnourished, while 23.3% were overweight. Iniesta R. et al. [
13] confirm that patients with brain tumors had the highest risk of being overweight and obese compared to other types of cancer. In a prospective study, Brinksma A. et al. [
16] have shown that in the first three months of treatment, most children with brain tumors increased the rate of WFA, BMI, and had a higher content of adipose tissue and lower lean body mass compared to children with solid tumors and hematological neoplasms. Musiol K. et al. [
50] observed that in children with brain tumors, BMI was the lowest during the maintenance and was significantly different compared to the control group. After the end of treatment, BMI increased significantly [
50].
1.2. Bone Health in Children with Cancer
The effect of treatment on the bone mineral content is also a very important issue because 40% of bone mass is formed in childhood [
51]. Children treated for cancer show worse bone formation and higher bone resorption [
52]. Added to the causes of bone structure disorders should be anti-cancer drugs like methotrexate, ifosfamide, cyclosporine, doxorubicin, cisplatin, and glucocorticosteroids, as well as radiotherapy, bone marrow transplantation, and decreased physical activity [
52].
Children with cancer have a higher risk of developing nutritional disorders than healthy children. Children with solid tumors are believed to be at greater risk of malnutrition than children with leukemia, who are more likely to be overweight and obese. Both malnutrition and obesity have a negative impact on survival, the occurrence of treatment toxicity, and EFS. The nutritional status assessment should be carried out regularly during therapy, and the assessment methods should be adapted to the type of tumor and the child’s age. During treatment, it is also necessary to remember and counteract the long-term effects of anti-cancer therapy, e.g., the occurrence of osteopenia and osteoporosis in cancer survivors, because this group has a significantly increased risk of their occurrence.
2. Regulation of Appetite in Children with Cancer
2.1. Appetite Regulation
The regulation of appetite in humans is a complex mechanism influenced by many factors [
69]. In the CNS, the hypothalamus is a key area influencing the regulation of appetite [
69]. The starvation center is in the lateral hypothalamic area (LHA), and the satiety center is in the ventromedial hypothalamus (VMH) [
69,
70]. They are influenced by neuropeptides and hormonal signals from tissues and organs [
71]. The integration of circulating signals of hunger and satiety takes place in the arcuate nucleus (ARC), within which there are two opposing neuronal systems [
71]. The first of them is the orexigenic system, which stimulates appetite through neuropeptide Y (NPY) and agouti-related peptide (AgRP) [
72]. The second one is the anorexigenic system suppressing appetite through a proopiomelanocortin (POMC) and the amphetamine-regulated transcript (CART) [
72]. Then, signals are transmitted to the paraventricular hypothalamic nucleus (PVN), where they are integrated and modified [
73]. The neurons of PVN send axons that secrete corticoliberin (CRH), thyroliberin (TRH), and oxytocin (OXT) [
73]. The arcuate nucleus also communicates with VMH, which secretes mainly anorexigenic brain-derived neurotrophic factor (BDNF) [
73], and LHA, which secretes the appetite-stimulating peptides orexin-A (OxA), orexin-B (OxB), and melanin-concentrating hormone (MCH) [
71].
Peripheral appetite regulators include gastrointestinal and adipose tissue hormones reaching the CNS via the bloodstream [
70,
74] but not all of them can cross the blood-brain barrier [
75]. Gut peptides also affect the brain via vagal afferent fibers [
71]. Leptin is a peptide produced mainly by white adipose tissue, and its concentration in the body positively correlates with the BMI and the amount of adipose tissue [
76]. The action of leptin in the human body is multidirectional, but best known is its participation in the regulation of hunger and satiety, where it stimulates the POMC/CART system and inhibits the secretion of NPY [
69,
71]. Ghrelin, a gastrointestinal hormone produced in humans mainly in the stomach by type A enteroendocrine cells, has the opposite effect as leptin [
77]. Stimulation of the starvation center is the main function of ghrelin, which negatively correlates with the BMI and concentration of leptin and insulin [
70,
74,
78]. The lesser known functions of ghrelin are modulation of taste sensation, glucose metabolism, and gut motility [
70]. Ghrelin level positively correlates with the severity of anorexia and cancer cachexia in adult patients [
79,
80,
81]. Another important regulator is insulin, a long-term signal of satiety that can cross the blood-brain barrier [
71]. Insulin stimulates leptin synthesis and inhibits NPY/AgRP neurons [
69,
71]. Glucagon-like peptide 1 (GLP-1) inhibits gastric emptying and reduces appetite, and stimulates the pancreas to secrete insulin [
82]. This hormone has an important role in glucose metabolism [
82]. Another peptide inhibiting food intake is peptide tyrosine-tyrosine (PYY), secreted in the distal intestine after a meal, especially after a protein-rich one [
83]. Cholecystokinin (CCK) is synthesized mainly in the duodenum and jejunum, but also in the CNS [
84]. It suppresses appetite and stimulates intestinal motility and secretion of insulin, glucagon, and pancreatic enzymes [
85].
Moreover, genetic factors also play a role in regulating the level of intestinal hormones and thus the appetite. This was confirmed by Czogała et al. [
86], who assessed the importance of FTO and PLAG1 gene expression in the context of gastrointestinal and adipose tissue hormone levels. The results indicate that the level of FTO and PLAG1 expression positively correlated with the concentration of leptin in the blood serum and negatively with CCK and GLP-1, while the expression and methylation of FTO negatively correlated with the levels of resistin and visfatin [
86].
2.2. The Causes of Appetite and Nutritional Status Disorders in Children with Cancer
During cancer treatment, the action of neurohormones, gastrointestinal, and adipose tissue hormones also may change [
88]. Only a few studies have shown gastrointestinal peptide dysfunction in children with cancer, and most have been conducted in children with leukemia. Fayh et al. [
90] carried out a systematic review, which showed a wide variation in results. Most of the included studies [
90] looked at the concentration of leptin, but in only one research was a higher level of leptin observed in children with cancer [
91], while the remaining studies found lower concentration or no difference compared with the control group [
90]. Only two studies looked at ghrelin concentration, and one of them indicated lower ghrelin levels in children with cancer, which increased in later stages of treatment [
91]. As the causes of the varied results, the authors indicate different types of cancers, treatments, and ages of children [
90]. Agyrou et al. [
92] (2019) presented an overview of research on ghrelin, leptin, and adiponectin levels in children with ALL. They noticed that in most studies, the leptin level was higher and the adiponectin level was lower at diagnosis [
92]. Furthermore, Carvalho Gomes CC et al. [
93] assessed the levels of appetite-regulating hormones in children with ALL during the induction at three-time points. Statistically significant changes have been observed in the level of ghrelin, which positively correlated with food consumption [
93]. The concentration of leptin, insulin, and cortisol did not change significantly during the 28 days of the study [
93]. Barbosa-Corte et al. [
94] have shown that malnourished children with solid tumors and lymphomas have a lower leptin concentration than well-nourished children. Musial et al. [
50] observed no statistically significant differences between leptin levels in children with CNS tumors and the control group and no correlation between leptin concentration and BMI. Statistically, an insignificant lower leptin level at diagnosis was observed in patients with brain tumors compared to the control group (7.04 vs. 16.38 ng/mL) and malnourished children [
50]. Changes in gastrointestinal peptides have also been indicated by Skoczeń et al. [
95], who observed that the concentration of CCK, ghrelin, and GLP-1 and the expression of their genes were significantly lower before bone transplant compared to 6 months after transplantation. Moreover, the concentrations of peptides in the test group were significantly lower than in the control group of healthy children [
95]. The authors indicate that it may be caused by damage to the gastrointestinal mucosa, and the measurement of the concentrations of selected peptides may be a marker of gastrointestinal regeneration [
95].
Appetite is also altered by disturbed gastrointestinal tract motility, taste, and smell disturbances, occurring at 45–84% for taste and 5–60% regarding the smell of adult cancer patients [
8]. Cancer patients also exhibit increased protein catabolism and lipolysis, as well as inhibition of lipoprotein lipase [
8,
87]. The deterioration of the body condition leads to the development of cachexia characterized by unintentional weight loss, including muscle and fat tissue, marked weakness, dysfunctional immunity, decreased intestinal peristalsis, and abnormal functioning of the heart and other key organs and systems of the body [
89].
Appetite regulation in humans is very complex and involves both CNS centers and peripheral factors. During oncological treatment, the action of hunger and satiety centers is disturbed by the action of proinflammatory cytokines, substances secreted by cancer, and metabolic disorders. In children with cancer, changes in the level of gastrointestinal peptides such as CCK, ghrelin, leptin, and GLP-1 are also observed. However, the results of individual studies are contradictory, and this issue requires further research.
3. The Role of Endocannabinoids System in Childhood Cancer
3.1. Physiology of ECS
ECS is a system of endogenous cannabinoids, receptors, enzymes, and transport proteins, discovered in the 90s [
9,
96]. It is found in mammals, other vertebrates, and some invertebrates [
9,
97]. In humans, it is already present in the embryo, while cannabinoid receptors in the brain are detected in the 14th week of fetal life [
98]. Moreover, blocking CB1 receptors in mice in the first 24 h of life inhibited the suckling of milk [
99]. Added to the best known and first discovered ECS ligands should be included anandamide (AEA) and 2-arachidoyl glycerol (2-AG) [
100,
101]. Both endocannabinoids are formed “on-demand” [
102]. They are lipid derivatives of arachidonic acid (AA) belonging to omega-6 polyunsaturated fatty acids [
9]. The precursor of AEA is N-acylphosphatidylethanolamine (NAPE), from which in the brain, kidneys, liver, lungs, spleen, and heart, anandamide and phosphatidic acid are formed using N-acyl phosphatidylethanolamine phospholipase D (NAPE-PLD) [
9,
97,
103]. The 2-arachidonoyl glycerol is formed from diacylglycerol (DAG) using diacylglycerol lipase (DAGL) and phospholipase C [
104,
105,
106,
107]. Endocannabinoids have to leave the cell to fulfill their function, and due to their polar nature, the eCB membrane transporter must be involved. The termination of endocannabinoid signaling is intracellular [
108]. AEA is mainly degraded by fatty acid amide hydrolase (FAAH) to ethanolamine and arachidonic acid, while 2-AG is hydrolyzed by monoacylglycerol lipase (MAGL) to arachidonic acid and glycerol [
109]. It is worth noting that arachidonic acid formed due to hydrolysis is a substrate for the production of prostaglandins [
9].
In the ECS, there are two main types of receptors—CB1 and CB2, which are G protein-coupled receptors (GPCRs) [
96]. CB1 receptors are located primarily in the brain—most of them in the basal ganglia, cerebellum, hippocampus, and cortex [
108]. They are also located in endocrine glands, thyroid and adrenal cells, ovaries, testes, uterus, and placenta, in the gastrointestinal tract, and in adipose tissue, where endocannabinoids activate lipoprotein lipase and fat deposition [
110]. In addition, CB1 receptors are also found in the vagus nerve endings [
110]. CB2 receptors are located mainly in cells of the immune system—on the surface of B lymphocytes, macrophages, monocytes, and NK cells. Moreover, they are also in the spleen, tonsils, and hematopoietic cells [
111], and in the CNS they are located mainly in microglia [
92]. Anandamide has a high affinity for the CB1 receptor and low affinity for CB2, while 2-AG can bind to both receptors [
96].
3.2. The Role of the ECS in the Regulation of Appetite
The ECS in the human body works in a multidirectional way, and its role is still being investigated [
9]. The best-known function of ECS is the regulation of energy balance and food consumption [
9]. Other known functions of the ECS include pain control, thermogenesis, sleep cycle regulation, embryogenesis, neurogenesis, learning, and memory, as well as regulation of lipid and glucose metabolism [
9,
109,
111].
In the appetite control process, CB1 receptors in appetite-regulating regions of the hypothalamus are involved, as well as CB1 receptors located in the limbic system, digestive tract, and adipose tissue [
109]. It is worth noting that by the presence of these receptors in the limbic system, ECS takes part in the hedonic evaluation of food [
70]. The ECS also decreases gastric acid secretion and gastrointestinal motility [
112]. A study on an animal model confirms the role of endocannabinoids in regulating the energy balance. Mice with knockout CB1 receptors had lower body weight, were resistant to hyperphagia [
113], and were insensitive to the action of leptin [
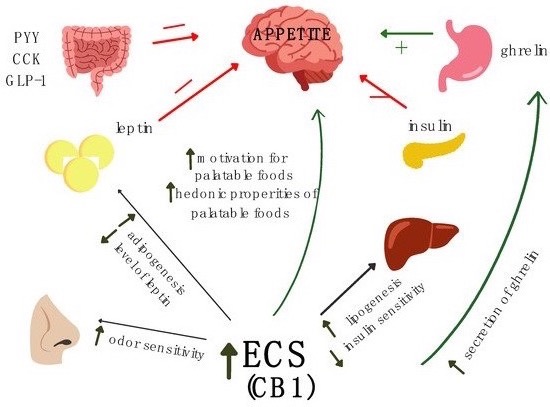
114]. Activation of the CB1 receptors in OUN leads to increasing motivation for palatable foods and increasing odor sensitivity, which leads to a reduction of satiety feeling and increased food intake (
Figure 1) [
115,
116]. ECS also interacts with gastrointestinal peptides. Activation of the ECS leads to ghrelin secretion, which increases appetite (
Figure 1) [
102]. This is a two-way action because the ECS system stimulates the secretion of ghrelin in the digestive system, while ghrelin stimulates the synthesis of 2-AG [
116]. Furthermore, in CB1 knockout mice, ghrelin didn’t show an anorexigenic effect [
117]. It has also been known that leptin levels negatively correlate with endocannabinoid concentration [
110,
118] (
Figure 1). Activation of CB1 receptors also leads to an increase in insulin secretion, somatostatin, glucagon, and visfatin [
110]. Furthermore, cholecystokinin reduces the expression of CB1 receptors [
119].
Figure 1. The role of endocannabinoid system (ECS) and gastrointestinal peptides in the regulation of appetite.
A high-fat and high-calorie diet can also modulate the ECS. Tagliamonte et al. [
120] have shown that overweight and obese people have lower plasma AEA levels after switching from the Western to the Mediterranean diet, possibly due to increased intake of polyunsaturated fatty acids and decreased consumption of saturated fatty acids. In another study, Tagliamonte et al. [
121] have shown that fat and energy intake can influence the concentration of endocannabinoids, NAE, and NAPE.
3.3. The Role of ECS in Childhood Cancer
The potential role of ECS in the development and course of diseases is still being investigated. It is currently known that in children it plays a role in the pathogenesis of such diseases as immune thrombocytopenia, juvenile idiopathic arthritis, type 2 diabetes, inflammatory bowel disease, celiac disease, obesity, and inflammation of the nervous system [
122]. There is no data in the literature on the role of ECS in oncological diseases in children. Most of the research is carried out among adults, where the anti-cancer properties of cannabinoids have been demonstrated in breast and pancreatic cancer, melanoma, lymphoma, and brain tumors [
111]. Among children, there are single studies assessing the importance of the cannabinoid system and synthetic cannabinoids. Andradas [
111] points out that most of the conducted studies concern acute lymphoblastic leukemia, which indicates that cannabinoids destroy cancer cells both in vivo and in vitro and that cannabinoids THC and CBD interact with vincristine, cytarabine, and doxorubicin in vitro [
123,
124]. It has also been shown that synthetic cannabinoids inhibit rhabdomyosarcoma growth [
125] and reduce the viability and invasiveness of neuroblastoma cells [
126]. Furthermore, synthetic cannabinoids induced cell cycle arrest of osteosarcoma cells [
127]. In the case of brain tumors, it has been shown that in the group of children with low-grade gliomas, the level of CB1 expression was a predictor of spontaneous involution [
128].
The role of ECS in children’s oncology is still little known. In vitro studies indicate the anti-cancer effects of cannabinoids on leukemia, neuroblastoma, rhabdomyosarcoma, and osteosarcoma cells. Furthermore, cannabinoids can enhance the toxic effects of drugs. Another interesting issue is the interaction of endocannabinoids with gastrointestinal peptides. Endocannabinoids correlate positively with ghrelin secretion and negatively with leptin secretion. This topic also requires future research, especially in children with cancer.
This entry is adapted from the peer-reviewed paper 10.3390/ijms23095159