Regarding the acute responses after leg-press strength training with or without serial stretch-loading stimuli, visible changes were observed in the muscle force, rate of force development, and hormonal concentrations between pre- and postmenopausal women (only one study). Long-term studies revealed different training adaptations after performing leg-press strength training with unique serial stretch-loading stimuli. A positive trend for leg-press strength training with serial stretch-loading was recorded in the young population and athletes; however, more variable training effects favoring one or the other approach were achieved in the older population.
- proprioception
- isokinetic
- strength
- power
- musculoskeletal injuries
1. Introduction
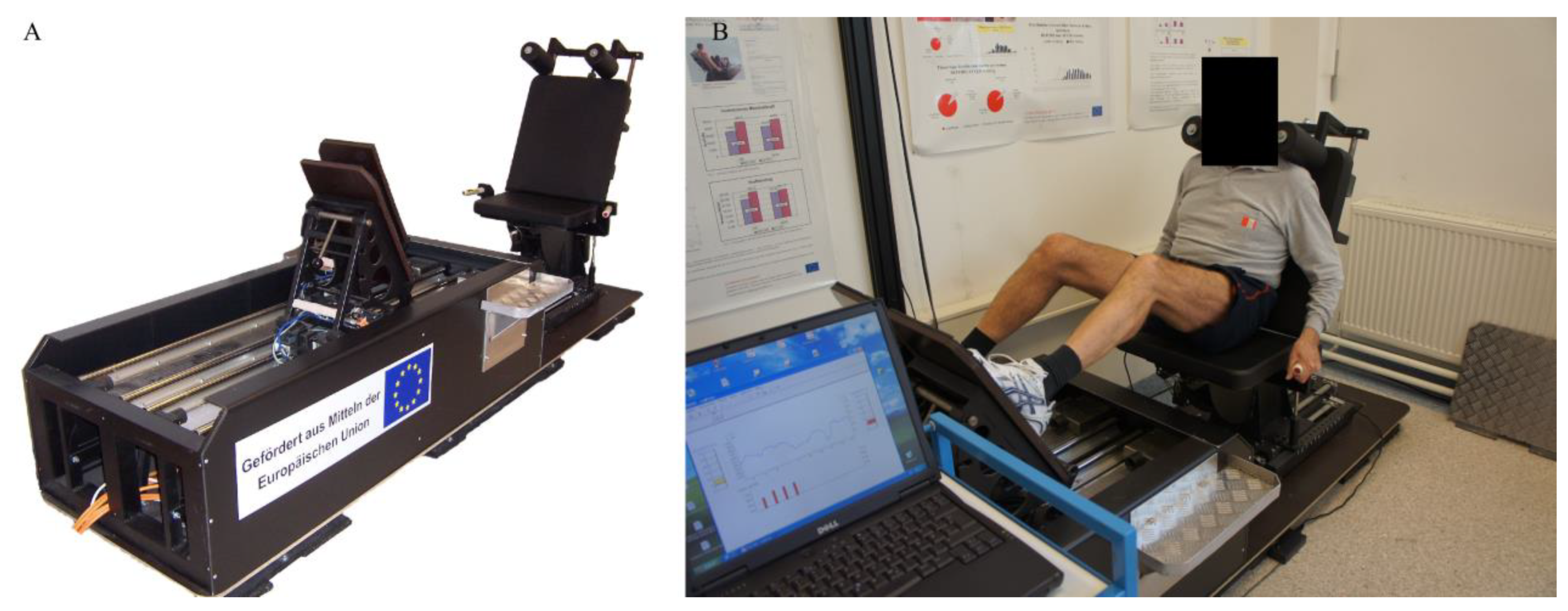
2. Leg Press Used for Testing and Acute Responses
3. Leg Press Used for Training and Its Effect on Various Outcomes
|
Study |
Sample |
Design |
Measures |
Intervention |
Results |
|---|---|---|---|---|---|
|
Cvečka et al. [14] |
Young well-trained males Isokinetic LP SSL group (n = 17, 23.3 ± 2.6 years) Isokinetic LP group (n = 16, 22.6 ± 2.5 years) |
Randomized controlled trial Two groups pre/post design |
Isometric bilateral MVC force on a leg press device Isokinetic bilateral maximal and mean force in concentric and eccentric phase of leg press exercise Isometric bilateral RFD (200 ms) on a leg press device CMJ height |
Duration 8 weeks Trained 3 x/week Isokinetic bilateral LP SSL group
Isokinetic bilateral LP group
|
Both groups showed sig. increases in MVC (LP SSL: 48.1%, p < 0.01; LP group: 24.8%, p < 0.01) RFD (LP SSL: 37.9%, p < 0.05; LP group: 31.4%, p < 0.05) and maximal concentric force (LP SSL: 45.4%, p < 0.01; LP group: 47.0%, p < 0.01). Mean concentric force sig. increased only in LP SSL (47.5%, p < 0.01) Maximal eccentric force sig. increased in both groups (LP SSL: 43.6%, p < 0.01; LP group: 24.7%, p < 0.01) Mean eccentric force sig. increased in both groups (LP SSL: 43.5%, p < 0.01; LP group: 24.9%, p < 0.05) CMJ sig. increased only in the LP SSL group (7.2%, p < 0.05) Isokinetic LP SSL achieved almost double the % increments in MVC, mean concentric force, maximal eccentric force and mean eccentric force compared to the isokinetic LP group only RFD, maximal concentric force and CMJ % improvements were similar between the groups |
|
Kern et al. [15] |
Young male athletes (n = 29, 22.95 ±.2 years) Isokinetic LP SSL group (23.1 ± 2.7 years) Isokinetic LP group (22.6 ± 3.9 years) |
Randomized controlled trial Two groups pre/post design |
Isometric unilateral MVC force and RFD (0–50 ms) on a leg press device SJ height 30-m sprint time Muscle biopsies
Gene expression |
Duration 8 weeks Trained 3 x/week Unilateral or bilateral training is not defined Concentric velocity was 0.3 m/s and eccentric one 0.2 m/s Isokinetic LP SSL group
Isokinetic LP group
|
Both groups showed significantly improved isometric unilateral MVC force (LP SSL: 48.1%, p < 0.01; LP group: 24.8%, p < 0.01) Only the LP SSL group showed sig. improvements in the RFD (30.2%, p < 0.001), SJ height (7.4%, p < 0.005) as well as 30-m sprint time (−1.3%, p < 0.05) No significant differences between the groups in the strength outcomes, jump and sprit time Only the LP SSL group significantly increased fast muscle fiber diameter (9%, p < 0.001)
LP SSL group showed sig. increases in IGF-1Ec (2-fold change, p < 0.05) and PGC-1α (228%, p < 0.05)
|
|
Kern et al. [16] |
Seniors (gender not defined)Group 1 (Vienna): 2 subgroups
(n = 16, 74.93 ± 5.48 years)
Group 2 (Bratislava): 2 subgroups -Isokinetic LP SSL group (n = 9, 71.12 ± 3.34 years)
(n = 9, 70.41 ± 3.74 years) |
Randomized controlled trial Four groups pre/post design |
Unilateral knee extension
10 m fasted walking Chair raise TUG Stair test Dynamic balance Muscle biopsies
|
8–10 weeks of training (10 in Group 1, 8 in Group 2) Bilateral training Two subgroups (isokinetic LP SSL groups) performed a ST on the LP device with SSL mode One subgroup from each group (ES groups) performed home-based electrical stimulation Detailed training program is not specified |
Group 1: LP SSL subgroup showed sig. improvements in all functional tests except for MVC force. ES subgroup showed sig. improvements in all functional tests except for dynamic balance Group 2: LP SSL subgroup showed sig. improvement in only the chair raise test (from 12.52 ± 1.98 to 10.12 ± 1.41 s, p = 0.041) while others remained unchanged. ES subgroup showed sig. improvements in also chair rise test (from 13.12 ± 2.60 to 11.25 ± 1.66 s, p = 0.018) Both groups and their subgroups showed sig. increases in myofiber diameter |
|
Šarabon et al. [17] |
Sedentary seniors (gender not defined) 74.3 ± 7.0 years Three groups:
(n = 28)
|
Randomized controlled trial Three groups pre/post design |
30 s static balance
|
Duration 9 weeks Trained 3 x/week Bilateral training Isokinetic LP SSL group
CON group: continued in their normal daily activities |
The Isokinetic LP SSL group showed sig. improvements in CoP velocity in anterior-posterior (from 14.4 ± 1.5 to 11.4 ± 1.1 mm/s, p < 0.05), medial-lateral (from 7.5 ± 0.7 to 6.1 ± 0.5 mm/s, p < 0.05) and total direction (from 17.6 ± 1.6 to 15.2 ± 1.2 mm/s, p < 0.05) as well as anterior-posterior amplitude (from 5.6 ± 0.5 to 4.9 ± 0.5 mm, p < 0.05) The ES group showed sig. improvements in medial-lateral CoP velocity (from 6.9 ± 0.7 to 5.6 ± 0.4 mm/s, p < 0.05) The CON group sig. worsened CoP anterior-posterior velocity (from 14.6 ± 1.7 to 16.1 ± 1.5 mm/s, p < 0.05) |
|
Cvečka et al. [18] |
Sedentary seniors Gender and age are not defined Two groups:
|
Randomized controlled trial Two groups pre/post design |
Isometric MVC torque on a chair dynamometer
Chair rising test TUG 10 m walk test |
Duration 8 weeks Bilateral or unilateral training is not defined Isokinetic LP SSL group
ES group
|
The LP SSL group showed sig. improvements in MVC torque (from 222 to 236 Nm, p < 0.05), chair rising test (from 12.5 to 10.4 s, p < 0.05), TUG (from 6.29 to 5.68 s, p < 0.05), 10 m walk test (from 5.06 to 4.80 s, p < 0.05), and postural stability test (data not shown) The ES group showed sig. improvements in MVC torque (from 232 to 248 Nm, p < 0.05), chair rising test (from 13.10 to 10.80 s, p < 0.05), TUG (from 7.61 to 6.96 s, p < 0.05), and 10 m walk test (from 5.96 to 5.52 s, p < 0.05) No sig. differences between the groups |
|
Zampieri et al. [19] |
Sedentary seniors (M/F) Isokinetic LP SSL group (n = 9, M = 5, F = 4, 71.8 ± 7.1 years) ES group (n = 16, M = 8, F = 8, 70.6 ± 2.8 years) |
Randomized controlled trial Two groups pre/post design |
Isometric MVC torque on a chair dynamometer Functional tests using “SFT battery”
Muscle biopsy including myofiber diameter Unilateral or bilateral testing is not specified |
Duration 9 weeks Isokinetic LP SSL group
ES group
Detailed training program is not specified in both groups Unilateral or bilateral training is not specified |
The isokinetic LP SSL group showed sig. improvements in chair rise test (from 10.95 ± 1.75 to 9.54 ± 1.92 s, p < 0.05) and 10 m fast walking test (from 1.90 ± 0.19 to 2.01 ± 0.23 s, p < 0.005) The ES group showed sig. improvements in isometric MVC torque (from 1.42 ± 0.34 to 1.51 ± 0.38 Nm, p < 0.05), TUG (from 8.42 ± 1.95 to 7.04 ± 1.09 s, p < 0.0005), chair rise test (from 13.85 ± 3.33 to 10.53 ± 3.63 s, p < 0.005), 10 m habitual walking test (from 1.20 ± 0.19 to 1.26 ± 0.18 s, p < 0.05) and 10 m fast walking test (from 1.58 ± 0.28 to 1.66 ± 0.24 s, p < 0.05) The isokinetic LP SSL group showed sig. decreases in slow (from 55.43 ± 17.33 to 53.12 ± 16.06 μm, p < 0.001) and fast type myofiber diameter (from 48.96 ± 16.18 to 46.43 ± 15.96 μm, p < 0.001) The ES group showed sig. decreases in slow type myofiber diameter (from 50.30 ± 14.78 to 48.48 ± 16.67 μm, p < 0.001) but sig. increases in the fast type myofiber diameter (from 46.53 ± 14.04 to 47.54 ± 15.79 μm, p < 0.001) |
|
Billy et al. [20] |
Sedentary seniors (M/F) Total knee arthroplasty Isokinetic LP SSL group (n = 26, M = 9, F = 17, 64.9 ± 6.0 years) Physiotherapy group (n = 29, M = 9, F = 20, 68.3 ± 6.7 years) |
Randomized controlled trial Two groups pre/post design |
Isometric unilateral MVC peak force of leg extension on a leg press device Isometric unilateral MVC torque of knee extension on a force chair TUG Stair test Pain and function Active and passive range of motion |
Duration 6 weeks Trained 2 x/week Unilateral training-involved and uninvolved leg Isokinetic LP SSL group
Physiotherapy group
|
The LP SSL group showed sig. improvements in MVC force on a leg press device with involved leg (from 8.9 ± 0.77 to 10.3 ± 1.06 N/kg, p < 0.05), MVC on force chair with involved (from 0.8 ± 0.06 to 1.0 ± 0.09 Nm/kg, p < 0.01) and uninvolved leg (from 1.2 ± 0.09 to 1.2 ± 0.11 Nm/kg, p < 0.01)
Physiotherapy group showed sig. improvements in MVC force on a leg press device with involved leg (from 6.7 ± 0.54 to 9.1 ± 0.70 N/kg, p < 0.05), MVC on force chair with involved (from 0.7 ± 0.06 to 0.9 ± 0.06 Nm/kg, p < 0.00) and uninvolved leg (from 1.1 ± 0.08 to 1.2 ± 0.07 Nm/kg, p < 0.01)
No sig. differences between the groups after training were recorded in any of the examined outcomes |
|
Zampieri et al. [21] |
Sedentary seniors (M/F) Isokinetic LP SSL group (n = 7, M = 4, F = 3, 70.1 ± 2.9 years) ES group (n = 10, M = 5, F = 5, 71.4 ± 7.1 years) |
Randomized controlled trial Two groups pre/post design |
Isometric MVC torque on a force chair Time to raise from a chair Muscle biopsies Gene expression Mitochondrial dynamics Unilateral or bilateral testing is not specified |
Duration 9 weeks Trained 2–3 x/week Isokinetic LP SSL group
ES group
Unilateral or bilateral training is not specified |
The isokinetic LP SSL group showed sig. improvements in chair raise test (p = 0.050) but no sig. changes in MVC torque The ES group showed sig. improvements in MVC torque (p = 0.026) and chair raise test (p = 0.036) The ES group showed sig. increases in myofiber size (from 49.16 ± 15.80 to 51.01 ± 16.38 μm, p < 0.0001) The isokinetic LP SSL group showed sig. decreases in myofiber size (from 57.87 ± 19.17 to 55.21 ± 18.13 μm, p < 0.0001) Only the ES group showed sig. decreases in the atrophy factor (p = 0.031) The ES group showed sig. upregulation of IGF1 pan (p = 0.001), IGF-1a (p = 0.001), IGF-1b (p = 0.014), IGF-1c isoforms (p = 0.013) The Isokinetic LP SSL group showed sig. induction of IGF1b isoforms (p = 0.002) Only the ES group showed sig. increases in mitochondria size (from 72.3 ± 1.9 to 80.4 ± 2.5 μm2, p = 0.009), although the mitochondria number sig. decreased (from 48.3 ± 1.3 to 38.6 ± 1.2 μm2, p = 0.0001)
|
This entry is adapted from the peer-reviewed paper 10.3390/ijerph19084445
References
- Yong-Seok, J. Usefulness of measuring isokinetic torque and balance ability for exercise rehabilitation. J. Exerc. Rehabil. 2015, 11, 65–66.
- Mavroidis, C.; Nikitczuk, J.; Weinberg, B.; Danaher, G.; Jensen, K.; Pelletier, P.; Prugnarola, J.; Stuart, R.; Arango, R.; Leahey, M.; et al. Smart portable rehabilitation devices. J. Neuroeng. Rehabil. 2005, 2, 18.
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46.
- Hamar, D. Universal linear motor driven Leg Press Dynamometer and concept of Serial Stretch Loading. Eur. J. Transl. Myol.-Basic Appl. Myol. 2015, 25, 215–219.
- Wang, E.; Nyberg, S.K.; Hoff, J.; Zhao, J.; Leivseth, G.; Tørhaug, T.; Husby, O.S.; Helgerud, J.; Richardson, R.S. Impact of maximal strength training on work efficiency and muscle fiber type in the elderly: Implications for physical function and fall prevention. Exp. Gerontol. 2017, 91, 64–71.
- Caserotti, P.; Aagaard, P.; Larsen, J.B.; Puggaard, L. Explosive heavy-resistance training in old and very old adults: Changes in rapid muscle force, strength and power. Scand. J. Med. Sci. Sports 2008, 18, 773–782.
- Sedliak, M.; Zeman, M.; Buzgó, G.; Cvecka, J.; Hamar, D.; Laczo, E.; Okuliarova, M.; Vanderka, M.; Kampmiller, T.; Häkkinen, K.; et al. Morphological, molecular and hormonal adaptations to early morning versus after-noon resistance training. Chronobiol. Int. 2018, 35, 450–464.
- Billy, W.; Sarabon, N.; Löfler, S.; Franz, C.; Wakolbinger, R.; Kern, H. Relationship between strength parameters and functional performance testsin patients with severe knee osteoarthritis. PM R. 2019, 11, 834–842.
- Sedliak, M.; Zeman, M.; Buzgó, G.; Cvečka, J.; Hamar, D.; Laczo, E.; Zelko, A.; Okuliarová, M.; Raastad, T.; Nilsen, T.S.; et al. Effect of time of day on esistance exercise-induced anabolic signaling in skeletal muscle. Biol. Rhythm Res. 2013, 44, 756–770.
- Kovárová, J.; Hamar, D.; Sedliak, M.; Cvečka, J.; Schickhofer, P.; Böhmerová, Ľ. Acute Response of Bone Metabolism to Various Resistance Exercises in Women. AFEPUC 2015, 55, 11–19.
- Vajda, M.; Kovarova, J.; Okuliarova, M.; Cvecka, J.; Schickhofer, P.; Bohmerova, L. Acute hormonal and neuromuscular response to various loading in young pre- and middle-aged postmenopausal women. Gazz. Med. Ital. Arch. Sci. Med. 2017, 177, 443–451.
- Scott, J.P.; Sale, C.; Greeves, J.P.; Casey, A.; Dutton, J.; Fraser, W.D. The role of exercise intensity in the bone metabolic response to an acute bout of weight-bearing exercise. J. Appl. Physiol. 2011, 110, 423–432.
- Avin, G.K.; Law, F.L. Age-related differences in muscle fatigue vary by contraction type: A meta-analysis. Phys. Ther. 2011, 91, 1153–1165.
- Cvecka, J.; Hamar, D.; Trimmel, L.; Vogelauer, M.; Bily, W. Einfluss von serial stretch loading auf die Effektivität des isokinetischen. BAM 2009, 19, 175–180.
- Kern, H.; Pelosi, L.; Coletto, L.; Musaro, A.; Sandri, M.; Vogelauer, M.; Trimmel, L.; Cvecka, J.; Hamar, D.; Kovarik, J.; et al. Atrophy/hypertrophy cell signaling in muscles of young athletes trained with vibration-al-proprioceptive stimulation. Neurol. Res. 2011, 33, 998–1009.
- Kern, H.; Loefler, S.; Hofer, C.; Vogelauer, M.; Burggraf, S.; Grim-Stieger, M.; Cvecka, J.; Hamar, D.; Sarabon, N.; Protasi, F.; et al. FES Training in Aging: Interim results show statistically significant improvements in mobility and muscle fiber size. Eur. J. Transl. Myol. 2012, 22, 61–67.
- Nejc, S.; Loefler, S.; Cvecka, J.; Sedliak, M.; Kern, H. Strength training in elderly people improves static balance: A randomized controlled trial. Eur. J. Transl. Myol. 2013, 23, 85–89.
- Cvecka, J.; Tirpakova, V.; Sedliak, M.; Kern, H.; Mayr, W.; Hamar, D. Physical activity in elderly. Eur. J. Transl. Myol. 2015, 25, 249–252.
- Zampieri, S.; Mosole, S.; Löfler, S.; Fruhmann, H.; Burggraf, S.; Cvečka, J.; Hamar, D.; Sedliak, M.; Tirptakova, V.; Šarabon, N.; et al. Physical exercise in Aging: Nine weeks of leg press or electrical stimulation training in 70 years old sedentary elderly people. Eur. J. Transl. Myol. 2015, 25, 237–242.
- Bily, W.; Franz, C.; Trimmel, L.; Loefler, S.; Cvecka, J.; Zampieri, S.; Kasche, W.; Sarabon, N.; Zenz, P.; Kern, H. Effects of Leg-Press Training with Moderate Vibration on Muscle Strength, Pain, and Function After Total Knee Arthroplasty: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2016, 97, 857–865.
- Zampieri, S.; Mammucari, C.; Romanello, V.; Bardberi, L.; Pietrangelo, L.; Fusella, A.; Mosole, S.; Gherardi, G.; Höfer, C.; Löfler, S.; et al. Physical exercise in aging human skeletal muscle increases mitochondrial calcium uniporter expression levels and affects mitochondria dynamics. Physiol. Rep. 2016, 4, e13005.
- Shaw, I.; Shaw, S.B.; Brown, A.G.; Shariat, A. Review of the Role of Resistance Training and Muscu- loskeletal Injury Pre-vention and Rehabilitation. Gavin J. Orthop. Res. Ther. 2016, 1, 1–5.
- Nguyen Ch Lefèvre-Colau, M.M.; Poiraudeau, S.; Rannou, F. Rehabilitation (exercise and strength training) and osteoar-thritis: A critical narrative review. Ann. Phys. Rehabil. Med. 2016, 5, 190–195.
- Jakobsen, T.L.; Kehlet, H.; Husted, H.; Petersen, J.; Bandholm, T. Early Progressive Strength Training to Enhance Recovery After Fast-Track Total Knee Arthroplasty: A Randomized Controlled Trial. Arthritis Care Res. 2014, 66, 1856–1866.
- Husby, S.V.; Foss, A.O.; Husby, S.O.; Winther, B.S. Randomized controlled trial of maximal strength training vs. standard rehabilitation following total knee arthroplasty. Eur. J. Phys. Rehabil. Med. 2018, 54, 371–379.