2. Conventional Therapy of ALL
As treatment of leukemia has improved over the past several decades, research has focused on looking for prognostic factors that influence a patient’s final response to treatment. Prognostic factors determine the assignment to a given risk group and thus the selection of the appropriate intensification of therapy. In developed countries, different protocols are used to treat ALL, and each of them distinguishes risk groups and prognostic factors: minimal residual disease (MRD), response to steroids therapy, immunophenotype, genetic factors, age of patient, white blood counts (WBC) at diagnosis used to qualify patients [
17]. One of the most important prognostic factors in patients with ALL remains MRD status which is defined as persistent malignant cells resistant to the chemotherapy that is used. Detection of 1 neoplastic cell per 10,000 healthy cells (0.01%) is sufficient for a positive MRD result. Minimal residual disease informs about the effectiveness of the applied treatment and the patient’s chemosensitivity, which allows for determining the residual burden of the disease and the risk of relapse [
18,
19]. Detection of persistent leukemic cells is based on two methods: multiparametric flow cytometry (FC-MRD) and molecular methods based on polymerase chain reaction (PCR-MRD) [
20]. FC-MRD and PCR-MRD status are determined at assigned time points (TP) during treatment. Multiparametric FC, based on the detection of leukemia-specific immunophenotypes using different combinations of fluorochrome-labeled monoclonal antibodies, is the fastest and most sensitive of approximately 10
−4 methods [
21]. Flow cytometry is applicable in about 90–98% of patients with ALL, but its sensitivity is lower as compared to methods based on real-time quantitative polymerase chain reaction (RQ-PCR) that is 10
−4–10
−6. The analysis of immunoglobulin (Ig) and the T-cell receptor (TCR) gene rearrangements are used as MRD markers in this technique (Ig/TCR-RQ-PCR) [
22]. Recently, the Euro Clonality-NGS Working Group developed a method for next-generation sequencing (NGS)-based IG clonality analysis. The study by van den Brand et al. showed that NGS-based IG clonality analysis is a high interlaboratory concordance (99%) and high concordance with conventional clonality analysis (98%) for the molecular conclusion [
23]. Another prognostic factor is the response to steroid therapy, which can be measured by testing the presence of peripheral blasts. It is measured after one week of steroid pro-phase. The group with the better results and, therefore, a greater chance of survival includes those who have a peripheral blast count less than 1000/mm
3 (good response to steroids). Patients with a poor response to steroids with peripheral blasts ≥ 1000/mm
3 are assigned a higher risk. Patients between 1 and 10 years old also have a significantly better overall prognosis [
24]. High WBC count at diagnosis is also an adverse factor, as patients with WBC count ≥50,000/mm
3 show worse response to treatment. In contrast to patients with pre-B-ALL, age and WBC count play less of a role in determining prognosis in patients with T-cell ALL (T-ALL) [
25]. Genetic abnormalities in a cancer cell also affect a patient’s prognosis. Hyperdiploid karyotype or
ETV6::
RUNX1 rearrangements are associated with a good prognosis. Hypodiploid karyotype,
BCR::
ABL1,
KMT2A rearrangement,
TCF3::
HLF fusion gene, or Ph-ALL-like subtype are connected with the poor prognosis. Intermediate prognosis is associated with
TCF3::
PBX1 fusion or newly identified
ETV6::
RUNX1-like rearrangement. Some of them are suitable candidates for molecular targeted therapy.
First-line treatment of pediatric ALL is conducted in several phases such as induction, consolidation, intensification (reinduction, delayed intensification in some protocols), and remission maintenance therapy. Induction of remission is based on steroid therapy accompanied by administration of cytostatic. Prednisone and dexamethasone were among the first drugs used in the treatment of ALL and remain an essential part of therapy. Consolidation of remission and maintenance therapy in most protocols is based on systemic and intrathecal cytostatic administration. Steroids have the ability to bind to the glucocorticoid receptor, resulting in inhibition of cytokine production, altered oncogene expression, cell cycle inhibition, and eventually cell apoptosis [
26]. The general principle of cytostatic agents is to disrupt the cell cycle and cause cell death or inhibit cell growth and division. The most commonly used are methotrexate, daunorubicin, doxorubicin, vincristine, cytarabine, cyclophosphamide, thioguanine, and 6-mercaptopurine. The entire therapy usually takes about 2–3 years. Over the years, many research groups have undertaken studies to determine the effectiveness of specific protocols and their modifications in treating pediatric ALL patients. A large study, AIEOP-BFM ALL 2000, involving 127 centers, took place between July 2000 and July 2006. The study enrolled 4839 children and adolescent patients from the ages of 1 to 17 years and diagnosed with ALL. The 5-year EFS was 83.9%, and OS was 90.5%. Multiple toxicities, including life-threatening events, were registered in this study. The most frequent one was the development of bacterial infection (43%) during the induction phase. As many as 43% of these infections turned out to be fatal [
5,
27].
The UKALL 2003 trial was going on between October 2003 and June 2011. This study enrolled 3207 children and young adults (to 25 years old) with ALL. The 5-year EFS was 87%, and the 5-year OS was 91.5%. In this study, 1101 serious adverse events were reported, and 16% of them were serious infections. Bacterial infections were the most common, followed by fungal infections. During the induction phase, 17 deaths were reported, mainly due to infection [
28]. The study of Children Oncology Group (COG) AALL0331 included 5377 patients between the age of 0 and 10 and took place between April 2005 and May 2010. The 6-year EFS was 88.96%, and OS rates were 95.54%. The rate of grade 3 and 4 neutropenia was 62%, while neutropenic fever was 29%. Infections accounted for 23% of reported adverse events [
29]. From August 2002 to October 2009, a total of 150 patients with B-cell ALL aged from 15 to 24 years were enrolled in the Japan Association of Childhood Leukemia Study (JACL’s) ALL202-U. The EFS and OS at 5 years for all patients were 67% and 73%. About 100% of patients developed grade 4 neutropenia during induction. A total of 46.5% experienced neutropenic fever, and nearly 5% developed sepsis as a result of infection [
30]. Currently, there are several protocols for the treatment of pediatric ALL, and more than a dozen studies are ongoing.
Table 1 shows the differences between the selected protocols used in developed countries.
Table 1. Comparison of selected treatment protocols in regard to prognostic factors, time points, and new approaches for treatment in clinical trials.
| Protocol |
Prognostic Factors |
New Approaches for Treatment in Clinical Trials |
Reference |
| AIEOP-BFM ALL 2017 |
Age at diagnosis < 1 year old
Response to steroids on 8th Day of Protocol 1
FC-MRD in BM on 15th Day of Protocol 1
PCR-MRD in BM (TP1) on 33th Day of Protocol 1
PCR-MRD in BM (TP2) at 12 weeks of treatment
genetic aberrations: KMT2A-AFF1, TCF3-HLF, IKZF1, ETV6-RUNX1, TCF3-PBX1, hypodiploidy |
Patients with detectable resistance to chemotherapy and high risk of relapse may be candidates for treatment with blinatumomab (NCT03643276) |
[31] |
| UK ALL 2011 |
WBC at diagnosis
Age at diagnosis
FC-MRD in BM on 8th,15th, and 29th Day of Protocol 1
PCR-MRD in BM at 9 and 14 weeks of treatment
genetic aberrations: iAMP21, t(17;19) q(22,p13), KMT2A rearrangement, hypodiploidy |
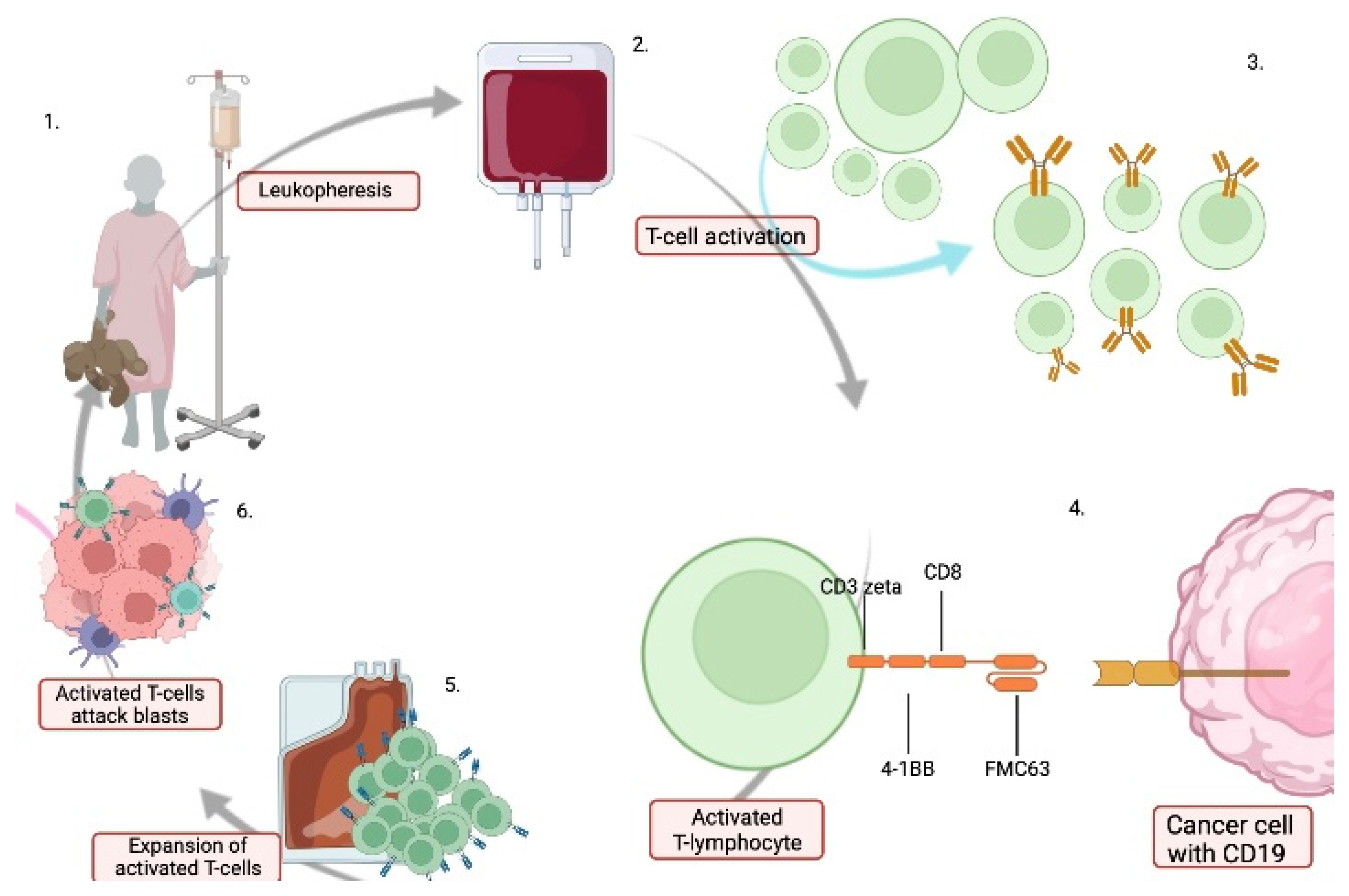
Patients with high risk may be candidates for chimeric antigen receptor T-cell therapy (CAR-T) as an alternative to HR blocks and HSCT (NCT03911128) |
[32,33] |
| COG-AALL |
WBC at diagnosis
Age at diagnosis
FC-MRD and PCR-MRD in BM on 15th and 29th Day of Protocol 1
genetic aberrations:
ETV6-RUNX1, KTM2A gene rearrangements, t(4,11) |
Patients with high risk may be candidates for a new drug called inotuzumab (AALL1732) |
[34,35] |
| Patients with high risk may be candidates for a blinatumomab (NCT03914625) |
AIEOP-BFM ALL 2017—International Collaborative Treatment Protocol for Children and Adolescents with Acute Lymphoblastic Leukemia, UK ALL 2011—United Kingdom National Randomized Trial For Children and Young Adults with Acute Lymphoblastic Leukemia and Lymphoma 2011, COG-AALL—Children Oncology Group Protocol; TP1—Time Point 1, TP2—Time Point 2, FC-MRD—flow cytometry minimal residual disease, PCR-MRD—polymerase chain reaction minimal residual disease, WBC—white blood cells, HR—high risk, BM—bone marrow.
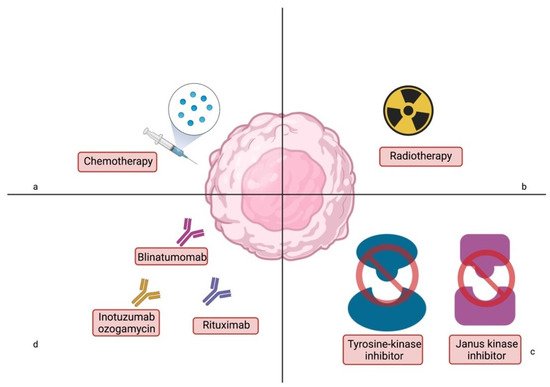
In addition to chemotherapy, radiation is used to treat acute lymphoblastic leukemia in select groups of patients. Formerly, craniospinal irradiation was a crucial departure point in the treatment of leukemia. Currently, eligibility for radiation therapy depends on a specific central nervous system (CNS) status at diagnosis. The criteria for CNS involvement are, subsequently: status 1—absence of CNS involvement; status 2—pleocytosis ≤ 5/µL with clearly identified blasts on cytospin of cerebro-spinal fluid (CSF) contaminated with blood; status 3—non-traumatic lumbar puncture with pleocytosis >5/µL or damage to the brain/meninges seen in imaging studies or the presence of neurological symptoms [
36]. Due to CNS involvement in ALL predisposition to poor treatment outcomes, cranio-spinal irradiation is used to control CNS recurrence [
37]. CNS irradiation is usually used in high-risk ALL patients with CNS status 3 [
38]. Due to the high toxicity, research has begun on reducing the radiation dose, the time at which the patient receives radiotherapy, or whether radiotherapy should be included in treatment at all. The concept behind the ALL-BFM trial protocols conducted between 1981 and 2000 was to minimize therapy to the point where disease control could be achieved without overwhelming side effects. Since 1981, irradiation doses have been reduced. In the ALL-BFM 83 study, prophylactic cranial radiotherapy (pCRT) was used at doses of 12 Gy and 18 Gy. The results indicated the efficacy of the lower irradiation dose. In ALL-BFM 95, pCRT was no longer used in patients with non-T-ALL, except for HR patients [
39]. In protocol ALL IC BFM2002, only patients with T-ALL and HR at 1 year of age received cranial prophylaxis radiotherapy (12 Gy) [
36]. The aforementioned trial focused on infant ALL, INTERFANT-99 did not use the cranial irradiation on its subjects due to proven neurocognitive repercussions of high severity. In this case, young age is considered a crucial factor predisposing to the adverse effects [
40,
41,
42]. The results from the AALL02P2 study conducted by the Children Oncology Group (COG) were published in 2021. The aim of the study was to perform intensified systemic treatment using drugs that penetrate highly into the CNS (dexamethasone, high doses of cytarabine, and MTX), which allowed delaying CRT by 12 months and reducing the irradiation dose to 12 Gy. The outcome of the study was for patients with B-ALL and isolated central nervous system relapse (
n = 112). In previous studies conducted by COG-POG 9061 and POG 9412, patients received radiotherapy at doses of 24 and 18 Gy and delayed radiotherapy for 6 to 12 months. The 3-year EFS and OS for patients on COG AALL02P2 (
n = 118) were 64.3% ± 4.5% and 79.6% ± 3.8%. Compared to late CNS-R B-ALL patients (
n = 50) on POG 9412 (previous study conducted by the COG), the 3-year EFS for COG AALL02P2 was significantly inferior (64.3% ± 4.5% compared to 79.9% ± 5.8%;
p = 0.03). The 3-year cumulative recurrence rate was 26.7%, with a higher incidence in HR patients. These studies demonstrate that CNS involvement is still a challenge in the treatment of ALL, and radiotherapy significantly improves outcomes in these patients. However, dose reduction and delayed radiotherapy should be continuously pursued to reduce toxicity [
43]. For patients with high-risk features in first complete remission (CR1), refractory, or relapsed disease, the highly effective treatment option remains allogeneic hematopoietic stem cell transplantation (HSCT). This group of selected patients includes children who have genetic anomalies that are associated with poor prognosis, for example: t(9;22)
BCR::
ABL1, t(4;11)
KMT2A::
AFF1, intra-chromosomal amplification of chromosome 21 [
44]. Most children, prior to allogeneic hematopoietic stem cell transplantation, receive conditioning that includes total body irradiation (TBI). Since TBI is associated with huge complications that affect the adult life of patients (i.e., growth impairment, hypothyroidism and delayed puberty, infertility), studies have been initiated on the necessity of TBI. So far, it has not been proven that TBI can be successfully replaced by chemotherapy exclusively. The most recent report by Styczynski et al. on the issue of using TBI or chemotherapy before transplantation was published in 2020. A total of 139 cases were analyzed: 55 patients underwent conditioning with TBI, and the remaining 84 patients were initially treated with chemotherapy alone. The 2-year OS was achieved by 84% after TBI, compared with only 60.5% after chemotherapy conditioning [
45]. The results were confirmed by the outcome of a study published in 2021 involving 3045 patients. Patients were divided into two groups: patients in complete remission 1 (CR1) and in complete remission 2 (CR2). Out of group 1 (
n = 1498), 1285 patients received TBI, and 213 patients received chemotherapy before HSCT. Among group 2 (
n = 1556), 1345 patients received TBI, and 211 patients received chemotherapy before HSCT. The EFS rate in both groups was higher in patients who received TBI than in patients who received chemotherapy; in the CR1 group, 63.8% vs. 61.4%, and in the CR2 group, 53.7% vs. 29.4% [
46]. The phase III, randomized, controlled, open-label, international, multicenter For Omitting Radiation Under Majority age (FORUM) study recruited 417 pediatric high-risk ALL patients in CR prior to the HSCT. Patients were randomly assigned into two groups. The first group received busulfan-based chemoconditioning, whereas the second group underwent TBI. TBI was proven to be more beneficial, as the 2-year OS of patients who were assigned to the TBI group was significantly higher than the 2-year OS of the remaining participants (91% vs. 75%,
p < 0.0001). Similarly, 2-year EFS was also higher in the TBI group than in the patients who were given conditioning chemotherapy (86% vs. 58%,
p < 0.0001). TBI conditioning was also associated with a lower risk of relapse, as the 2-year cumulative incidence of relapse (CIR) rate was lower in this group (12% vs. 33%,
p < 0.0001) [
47].
The effectiveness of HSCT has been demonstrated in many studies. For example, in 2018, a study report of 119 patients aged 1 to 18 years who received HSCT at AIEOP transplant centers was published. The aim of the study was to quantify MRD in patients immediately after transplantation as well as in the third trimester after bone marrow transplant. After HSCT, 61 patients from the study group achieved disease-free status, which allowed for the estimation of EFS and the 10-year OS at the level of 50% and 54%, respectively. Forty-eight patients relapsed after transplantation, with a median duration of 7 months after transplantation [
48]. In light of the emergence and increasing use of new therapeutic approaches (i.e., blinatumomab, CART-cell) in the context of post-HSCT or TBI-alone complications, the role of HSCT in ALL treatment should be re-examined.
The genetic characterization of ALL has revolutionized clinical treatment approaches. Currently, childhood ALL can be divided into more than 30 genetic subgroups that are associated with individual patient prognosis. Several groups in which the presence of a mutation or chromosome translocation leads to activation of particular metabolic pathways can be distinguished. This is usually associated with a poor diagnosis, as these pathways are commonly associated with increased cell survival. Nevertheless, over the years, methods of targeting those overactivated cascades in ALL have been developed. Mitigating consequences of overexpressed pathways significantly improve prognosis in previously HR groups. Furthermore, agents targeting signaling cascades contribute to decreased treatment toxicity.
The interleukin-7 (IL-7)/Janus kinase (JAK)/signal transducer and activator of transcription (STAT) signaling pathway is involved in both T and B-cells’ development [
56,
57,
58,
59]. Furthermore, STAT proteins play a vital role in cells’ survival, as they increase the synthesis of antiapoptotic Bcl-2 protein [
60,
61]. The IL-7/JAK/STAT pathway has been shown to be activated in T-ALL in both patient-derived leukemic cells and T-ALL cell lines, which was associated with increased cancer cell survival [
62,
63,
64,
65]. Therefore, JAK1/2 inhibitor ruxolitinib was tested during the preclinical studies. In a study by Maude et al., patient-derived xenografts models of early T-cell precursor (ETP) ALL have been established in NOD/SCID mice. Ruxolitinib significantly (
p < 0.01) reduced blast count in 5 of 6 xenograft models. Importantly, the efficiency of ruxolitinib was independent of the presence of JAK/STAT activating mutations; thus, it was suggested that this drug can be used in a larger group of patients than it was expected [
66]. In a study by Böhm and colleagues, the results of ruxolitinib treatment in Ph-like ALL preclinical models have been evaluated. Overactivation of JAK/STAT occurs in most of the Ph-like ALL cases. Of particular importance are rearrangements that overexpress the cytokine receptor-like factor 2 (CRLF2) gene, resulting in inappropriate activation of JAK signaling. The combination treatment with vincristine, dexamethasone, L-asparaginase, and ruxolitinib of mice engrafted with CRLF2-rearranged Ph-like ALL patient-derived xenografts decreased leukemic infiltration of various organs and prolonged time to remission, as compared to chemotherapy or ruxolitinib alone [
67]. Ruxolitinib is currently involved in a number of studies, such as Total Therapy Study XVII, which includes ruxolitinib for the induction phase in the patients with activation of the JAK/STAT pathway (NCT03117751). Currently, ruxolitinib in cotreatment with consolidation chemotherapy is also being tested in the treatment of children with HR CRLF2-rearranged and/or JAK pathway-mutant Ph-like pre-B-ALL (NCT02723994). Moreover, the phase II study of ruxolitinib in combination with chemotherapy for relapsed/remitting Ph-like ALL has been completed, and the results are yet to be posted (NCT02420717).