Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Rehabilitation
DEFS (Diagnostic Esthetic Functional Splint), namely CAD/CAM manufactured, “snap-retained”, tooth-colored splints available by materials exhibiting a certain degree of elasticity (like polycarbonates or acetal resins) for restoring function, esthetics and occlusion in several clinical situations, before or as an intermediate alternative to undergoing the final treatment.
- Prosthetic Dentistry
- CAD/CAM
- DEFS
- prosthetic rehabilitation
1. Introduction
Fixed prosthetic treatments in complex rehabilitations have always been the most sought after restorative solution by patients, for the offered functional, esthetic and psychological benefits [1]. However, the conditions for a prompt execution may not be present in all clinical situations: especially in advanced cases with severe stomatognathic and esthetic impairments and necessity of increase the vertical dimension of occlusion (VDO), a middle-term ad interim prosthesis is indicated, as minimally invasive as possible, in order to evaluate the individual functional and psychological response to oral modifications, as a prototype of the final prosthetic restoration [2].
It has always to be considered that, sometimes, the planned and often very relevant modifications of dental arches may not be accepted by patients showing low psychological/emotional compliance. Therefore, the use of “full-reversible” prosthetic solutions could be considered an undeniable must.
In other cases, a fixed prosthesis cannot be immediately indicated (or not feasible at all) for different reasons: for example, when a patient is too young and in full growth or too old, so that for medical reasons a complex, invasive and long-lasting treatment would be quite risky and expensive.
To date, in the scope of prosthetic planning and communication, Digital Dentistry offers many new, overwhelming tools that facilitate and speed up the prosthodontists’ daily practice in a terrific way, from intraoral scanners to a full digital workflow.
An innovative, efficient and versatile restorative approach is offered today by CAD/CAM manufactured, tooth-colored splints, retained by a “snap-on” type of mechanical engagement, available by materials exhibiting a certain degree of elasticity, like polycarbonates or acetal resins and reproducing the occlusal shape, the esthetic morphology and the color of the final restorations [2,3,4]. A certain degree of elasticity of such materials allows positioning onto the dental arch, thanks to a mechanical engagement into the undercuts of teeth, with neither use of luting cements nor subtractive tooth preparations. The idea of using a full-arch tooth colored splint led in the past years to the commercial launch of a novel device, known as “Snap-on-Smile” (DenMat SLR, Antessano, Italy), made of acetal resin, just for esthetic and cosmetic purposes. At the same time, due to its good esthetic and functional performance, the concept of a removable tooth colored splint was introduced by the Munich school as a temporary diagnostic tool or, in selected cases, as an intermediate alternative to conventional fixed prosthetic treatments (the so-called “Munich Splint Concept”) [3,4].
2. CAD/CAM DEFS (Diagnostic Esthetic Functional Splint)
The CAD/CAM DEFS (Diagnostic Esthetic Functional Splint), tooth colored, removable devices can be considered a valuable pre-treatment or definitive restorative option, since they show different promising indications for particular clinical situations.
Nowadays, according to the authors best knowledge, no long-term clinical study is available on such topic, besides technical and clinical case reports [5,6,7]. A 78-yr-old patient with a clinical history of osteonecrosis was treated with the snap-retained device for 5 years, successfully [5]. Several complex clinical cases have been handled satisfactorily with similar CAD/CAM-fabricated temporary appliances, redefining the vertical dimension of occlusion in a minimal invasive manner [6].
The effect of CAD/CAM occlusal devices on teeth and soft tissues health is a paramount aspect that should be further investigated. Removability facilitates oral hygiene daily procedures [8], but further long-term clinical studies are necessary to define the impact of DEFS on oral health.
Furthermore, additional studies should be carried out on the different materials used to fabricate DEFS appliances, in order to investigate the tribological behavior (wear, occlusal surface modifications over time, etc.). Up to now, polycarbonate [3,4,6,9,10] and resin [5,7,8] have been proposed in the currently available literature, but no long-term comparative study has been conducted yet.
This is particularly important if we consider that cases of severe tooth wear, inducing loss of dental hard tissues as a result of attrition, abrasion and erosion, [11] are increasing and increasing over the years: it has been estimated that severe tooth wear affects 3% of the population at 20 years old and 17% at 70 years old [12,13], increasing with the age.
In such cases, not only it is necessary to restore the appearance of the worn dentition but also mandatory to restore functional parameters, like VDO, centric relation, anterior guidance, anterior teeth phonetic relationship, perioral tissues support, etc. From this point of view, DEFS can be considered as a promising, very versatile and effective solution to evaluate the restorative validity and patient’s acceptance of a complex prosthetic rehabilitation, in a pre-treatment, totally reversible, non-invasive phase. Compared to a classic bis-acrylic resin mock-up, that has a limited duration of about 24 h [14], DEFS made of polycarbonate or acetal resin is a more comfortable and durable option, thanks to the high resistance and flexibility of CAD/CAM-generated high-density polymers used [6]. Pre-treatment with conventional occlusal splints is a well acknowledged step in a structured concept for complex prosthetic rehabilitations [15]; in dysfunctional patients, the short-term use of conventional occlusal splints is widely accepted for the treatment of temporo-mandibular disorders, offering occlusal stability and decreasing of muscular tension [16]. From this perspective, compared to the conventional occlusal stabilization splints, the DEFS could be considered as a possible tool to explore also esthetic and phonetic parameters. However, at the moment there are no available studies on this possible utilization.
Another advantageous indication of the DEFS is the ad interim rehabilitation of young patients with dental anomalies who are in the process of growing, and so cannot be submitted to a final fixed prosthetic treatment yet. Dental anomalies like amelogenesis imperfecta, dentinogenesis imperfecta, and multiple dental agenesis can severely affect self-confidence, especially during adolescence, and from this perspective DEFS can provide affordable esthetics and comfortable function until the definitive treatment is carried out in adulthood [10,17].
The removability of the DEFS in all situations facilitates dental hygiene procedures; for its part, the device can be employed as an effective temporary restoration, particularly versatile, for instance, in cases of single tooth edentulous sites treated with regenerative surgery, in order to not apply any functional load onto the treated ridge, or in multiple preparations for anterior veneers, where the absence of any temporary cement offers, at the time of the adhesive bonding, an excellent response of the marginal soft tissues and the absence of contamination of the enamel substrate.
DEFS also represent an effective, “last resort” prosthetic solution, as an extreme measure in cases of elderly patients, or people affected by severe diseases or disability contraindicating long, expensive and quite invasive treatments, also for an understandable low psychological compliance. To date, it is not possible to define the lifespan of these devices, due to the mechanical characteristics of the used materials, conceived for medium-term service; but such an approach offers a great advantage, compared to the conventional acrylic devices resulting from the digital workflow. Once the file of the project has been stored, DEFS can be reproduced as many times as needed, without any further clinical procedure on the patient (impression, occlusal registrations, etc.).
Hence, DEFS can be considered as a promising component of the prosthetic treatment, showing different indications and contraindications, which the authors would summarize as follows:
2.1. Indications
- TEMPORARY PROSTHESIS: in some clinical situations, removable, tooth colored, “snap-on”-retained splints can be used as temporary restorations, for example in the presence of short-span (e.g., one premolar) edentulous ridges, when, after implant placement or bone graft, the conditions for an immediate loading are not present and the patient is esthetically demanding. In these cases, DEFS can be used for the time period of osseointegration, without the need of modifying the teeth adjacent to the edentulous space, allowing, at the same time, a very easy hygienic access to the site. Moreover, as a temporary device, being removable, the pontic can be modified to provide a good esthetical correction in case of deformed ridge contour [18].
Another possible utilization as temporary restoration is when multiple teeth are prepared for laminate veneers in the anterior sites, offering the advantage of removing the temporary after every meal in order to maintain an excellent gingival health, that is a main prerequisite for the final adhesive cementation of the restorations [8].
- “TEST-DRIVE” approach [9]: this can be an effective solution when a pre-treatment diagnostic phase is needed to test esthetic and functional modifications of dental morphology in the patient’s mouth for a more or less prolonged time. An example is offered by cases of severe tooth wear (Figure 1 and Figure 2) in which, after defining new occlusal relationships, VDO [19,20], phonetics, esthetics and their general effects on the stomatognathic system including the facial muscles should be evaluated, analyzing the acceptance and adaptation by the patient (Figure 3 and Figure 4).
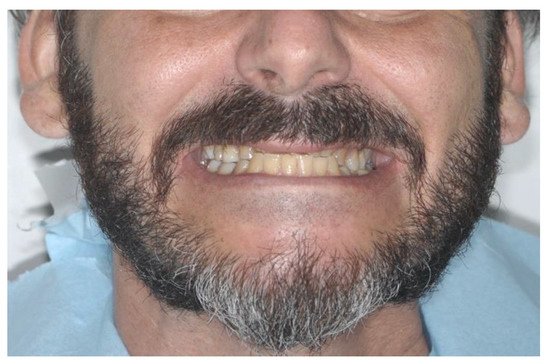
Figure 1. Case 1—Extraoral view of a patient with eating disorders and severe parafunctional habits.
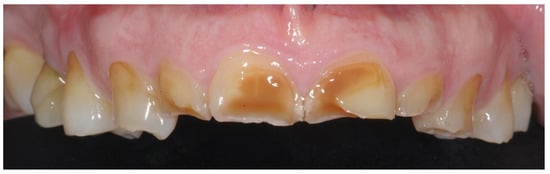
Figure 2. Case 1—Intraoral view of a patient with eating disorders and severe parafunctional habits.

Figure 3. Case 1—Digital project of the DEFS, limited to the maxillary arch.

Figure 4. Case 1—The DEFS, made of acetal resin.
This solution offers the important advantage of a complete, comfortable reversibility of the treatment plan (Figure 5 and Figure 6), if the result is not accepted by the patient: compared to the conventional composite “middle-term mock-up” adhesively bonded to the teeth surfaces, in fact, no removal of restorative materials is needed, neither will the patient be able to assert that his/her occlusion has changed, as sometimes it happens after the elimination of bonded diagnostic composite restorations.

Figure 5. Case 2—Dental arches of a patient with parafunctions.

Figure 6. Case 2—Intraoral view of a patient wearing DEFS, made of polycarbonate.
- TRANSITIONAL PROSTHESIS: in young patients affected by severe dental anomalies, such as amelogenesis imperfecta, dentinogenesis imperfecta or dental agenesis [10,17], DEFS can be very useful as ad interim, medium-term prosthesis, aimed at waiting for the achievement of growth, before a final restoration project can be performed, being periodically replaced, according to the ongoing growth (Figure 7, Figure 8, Figure 9, Figure 10, Figure 11, Figure 12, Figure 13, Figure 14 and Figure 15).

Figure 7. Case 3—Dental arches of a young patient with amelogenesis imperfecta.
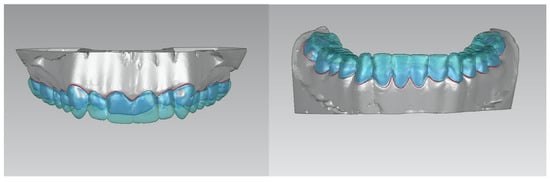
Figure 8. Case 3—Digital project of the upper and lower dental arches.

Figure 9. Case 3—DEFS are employed as transitional prosthesis.
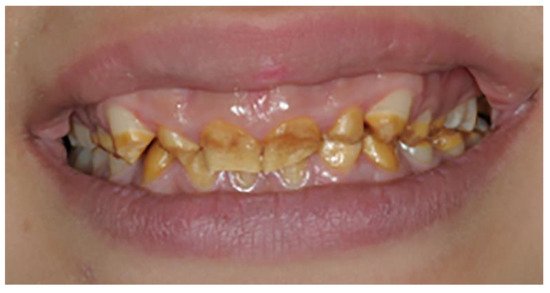
Figure 10. Case 3—Extraoral view of the patient with amelogenesis imperfecta.

Figure 11. Case 3—Extraoral view of the patient with amelogenesis imperfecta wearing DEFS.

Figure 12. Case 4—Extraoral view of a young patient with multiple dental agenesis.

Figure 13. Case 4—Dental arches of a young patient with multiple dental agenesis.

Figure 14. Case 4—Extraoral view of a young patient wearing DEFS, made of acetal resin.

Figure 15. Case 4—Intraoral view of the patient wearing DEFS.
- “LAST RESORT”: in elderly patients with several missing teeth, people affected by serious illnesses, requiring challenging therapies or suffering from particular diseases (e.g., osteonecrosis of the jaw) or in patients non-cooperating for severe disabilities (Figure 16, Figure 17 and Figure 18), DEFS can be considered as an acceptable, economically viable solution, alternative to a fully edentulous condition or to complex, invasive and costly fixed restorative treatments [5,21].

Figure 16. Case 5—Extraoral view of a patient with cerebral palsy.

Figure 17. Case 5—Intraoral view of the maxillary arch of the patient.
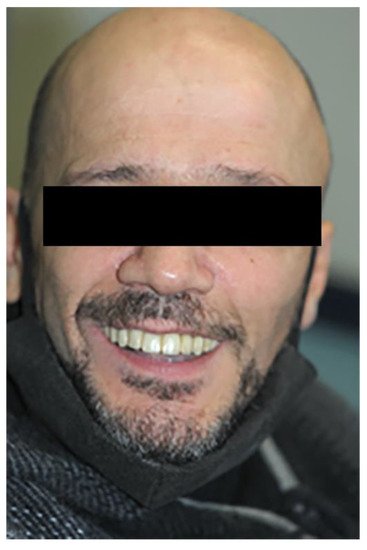
Figure 18. Case 5—Patient wearing DEFS, made of acetal resin.
2.2. Contraindications
The presence of four stable teeth at least is an indispensable factor to support a full-arch DEFS. The presence of periodontally compromised teeth, with advanced tooth mobility, negatively affects the retention of the splint due to a harmful biomechanical overload. Consequently, full-arch DEFS is contraindicated in case of presence of a severe periodontal disease, even if stabilized after a surgical treatment.
In other cases, tooth shape anomalies, frequently found, for instance, in some forms of amelogenesis imperfecta, can impair the “snap-on” retention mechanism of the splint, especially when natural undercuts are not sufficient. In those cases, a previous contour reshaping with composite resin can be effective to solve the problem.
Similarly, the presence of short teeth could render the mechanical mechanism of retention of DEFS less effective. Furthermore, an accurate initial evaluation and diagnosis of the patient are strongly suggested. DEFS devices are not recommended in those clinical cases where additive procedures could affect the aesthetic and functional parameters.
For instance, DEFS employment is not advisable in case of vestibularized teeth, since such type of device may induce the worsening of the aesthetics of the patient.
2.3. DEFS Workflow
Before starting a treatment with DEFS, a careful check of the oral health status is needed: dental, periodontal, mucosal and hygienic conditions have to be evaluated and, if necessary, preliminary restorative/periodontal treatments have to be performed in order to optimize the support.
The fabrication of this kind of splints is performed utilizing digital technologies, according either to a full or a mixed digital workflow (Figure 19).
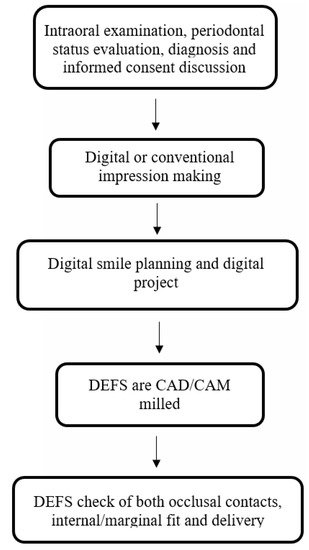
Figure 19. DEFS workflow.
The first step is an accurate impression procedure of dental arches, that can be performed by means of an intra-oral scanner, if a full-digital workflow is preferred (direct digitization), otherwise a conventional precision impression (with polyvinylsiloxanes or polyethers), properly made and poured in extra-hard, precision stone and finally digitalized with a laboratory scanner is equally valid (indirect digitization).
Centric relation, protrusive and lateral interocclusal registrations have to be carefully recorded, for setting a mechanical articulator or for uploading into the planning software (digital articulator), in order to proceed with the final project.
After defining the new morphology of the dental arch, carrying out a visual pre-visualization of the desired final outcome is strongly suggested, by means of the so-called “digital smile”, performed by dedicated software; this is paramount to get an initial, informed acceptance of the treatment plan by the patient [22,23].
In the following step, a conventional intra-oral mock-up is preferably made [14], based on the newly defined treatment goal, shown in the digital smile pre-visualization: silicone templates are modelled on the diagnostic wax-up (on the gypsum casts, in case of “mixed” workflow) or on the 3D printed cast of the final project (in the “full-digital” workflow) to transfer the new volumes, morphologies and, if needed, shades, onto the patient’s arches, without any tooth modification. For this purpose, some composite or bis-acrylic resin is poured into the silicone guide, then such a template is positioned onto the patient’s dental arch and removed after the material polymerization. A precise mock-up, transferring intra-orally the planned restorative project, offers a worthwhile tool to check dynamically the esthetic and functional modifications of the new draft, that can be shown to the patient and in case adjusted, if needed, in real time.
This step is of high importance in the process of acceptance of the final restorative project, allowing the patient to get a “physical” perception of the occlusion, phonetics and of the real integration in the total harmony of the facial esthetics (analysis and acceptation of shape and color of teeth, smile line, lip position and support) [23,24,25].
The DEFS concept is polyhedric and versatile, showing more indications if compared to the conventional resin direct mock-up.
The DEFS is milled with a CAD/CAM production software from a pre-polymerized disk of different high-density polymers and is retained by means of a snap-on mechanism, not requiring preparations or bonding of the tooth structures. The complete removability of DEFS allows the daily patients’ oral hygiene. Furthermore, DEFS devices can be employed to test functional, phonetic and aesthetic parameters in disfunctional patients. They can act as medium-term transitional prosthesis in young patients or represent a valuable alternative prosthetic treatment for elderly patients or patients with severe disabilities.
Differently, the conventional direct bis-acrylic resin mock-up can be a pre-treatment or post-preparation restoration or long-term provisional solution until further treatment can be completed [22]. It is a valid prosthetic expedient to test aesthetics and functions in case of prosthetic rehabilitations and allows a pre-visualization of the final result, but has a limited duration of about 24 h and is bonded to prepared teeth [22].
Conversely, thanks to the versatile technopolymers used, DEFS can offer new function and esthetics in a very short production time, especially when made according to a full-digital workflow and can be used as a test device for a medium/long time [9].
Actually, discs of acetal resin or polycarbonate can be CAD/CAM milled for producing these splints. Such technopolymers are fabricated under industrially standardized conditions, characterized by homogeneity, biocompatibility, stability, flexibility and good resistance to wear [6].
Acetal resin, for its part, is a homopolymer of highly crystalline polymerized formaldehyde [26] and has been used in dentistry since 1986 for the manufacturing of clasps, partial denture frameworks, temporary bridges, implant abutments, occlusal splints [27] and screw-retained temporary fixed prostheses [28]. According to studies conducted on acetal resin as full denture material, it shows good fracture resistance and acceptable color stability [29,30].
Polycarbonate is a polymer of carbonic acid and is used in dentistry for making brackets or temporary crowns [31]. Several studies have been carried out on its mechanical properties, showing: mean modulus of elasticity = 2500 MPa, flexural strength = 89.4–109.8 MPa, hygroscopicity = 2.43–11.43 μg/mm³, solubility = 0.11–0.30 μg/mm³, good behavior at transverse strength test, and good color stability [32,33]. Moreover, a study on surface roughness after loading has evidenced very low micro porosities [34].
Thanks to their good mechanical properties, both materials allow the fabrication of low thickness devices: the recommended minimum thickness for acetal resin is 0.7 mm, for polycarbonate is 0.3 mm, that is a highly valuable pre-requisite for any non-invasive treatment option [9].
At any time, DEFS can be replaced with a definitive treatment, based on the conventional restorative systems, like crowns, fixed dental prostheses, veneers, occlusal onlays, etc.
After obtaining informed consent from the patient, the DEFS is milled with a CAD/CAM production software from a pre-polymerized disk. Before delivering the device to the patient, a careful check of both occlusal contacts and internal/marginal fit has to be carried out by articulation paper and fit-checker paste.
Naturally, patient’s instruction, motivation and training for the management of the device are mandatory: the DEFS can be worn all day, up to 24 h, also during mastication and very carefully during food uptake, and should be easily inserted and removed by the patient, to be carefully cleansed after every meal, at the tooth-brushing times.
This entry is adapted from the peer-reviewed paper 10.3390/prosthesis4010014
This entry is offline, you can click here to edit this entry!