Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is an old version of this entry, which may differ significantly from the current revision.
Subjects:
Clinical Neurology
Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal and often repetitive, movements, postures, or both. Dystonic movements are typically patterned, twisting, and may be tremulous. Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation. Because of its wide clinical spectrum, dystonia is often underdiagnosed or misdiagnosed. In clinical practice, dystonia could often present in association with other movement disorders. An accurate physical examination is essential to describe the correct phenomenology.
- dystonia
- clinical diagnosis
- classification
1. Introduction
Dystonia is a hyperkinetic movement disorder characterized by sustained or intermittent muscle contractions causing abnormal movement or posture. Dystonia has distinct clinical features; however, a wide spectrum of phenomenological presentations may be recognized. Dystonia can present in isolation or in combination with other movement disorders like chorea, myoclonus, tremor, and parkinsonism [1]. Dystonia is one of the most underdiagnosed and misdiagnosed movement disorders. The most common misdiagnosis is between [2]: dystonic tremor and essential tremor, parkinsonian tremor, or psychogenic tremor; dystonic jerks and myoclonus; tic-like dystonia and Tourette syndrome. To aid clinicians in reaching the proper diagnosis, several classifications have been proposed over time. The first classification of dystonia was presented in 1976 [3], and during subsequent years it was modified several times [4][5][6]. The last classification was proposed in 2013 and distinguishes two main axes: axis 1, clinical characteristics, and axis 2, etiology [1]. The classification of dystonia in a single patient should be considered as a dynamic process, subject to re-evaluation in the light of the progression of clinical history and new advances in dystonia research.
2. Definition of Dystonia
The last definition of dystonia (proposed by a consensus of the Movement Disorder Society expert members) is articulated in these three sub-definitions [1]:
- Dystonia is a movement disorder characterized by sustained or intermittent muscle contractions causing abnormal and often repetitive, movements, postures, or both.
- Dystonic movements are typically patterned, twisting, and may be tremulous.
- Dystonia is often initiated or worsened by voluntary action and associated with overflow muscle activation.
3. Classifications of Dystonia
Once a movement disorder has been defined as dystonic in nature, further characterization according to current classification should be attempted. Starting with the first classification in 1976 [3], many classifications have followed [4][5][6]. Current classification of dystonia was proposed by a consensus of the Movement Disorder Society expert members in 2013 [1] (Table 1).
Table 1. Classifications of dystonia.
| Year | Reference |
|---|---|
| 1976 | (Fahn and Eldridge) [3] |
| 1987 | (Fahn, Marsden et al.) [4] |
| 1998 | (Fahn, Marsden et al.) [5] |
| 2011 | (Albanese, Asmus et al.) [6] |
| 2013 | (Albanese, Bhatia et al.) [1] |
The new classification system proposes an innovative view on how to classify dystonia [1]. The classification distinguishes two main axes [1][7]:
- Axis 1: Clinical characteristics (Figure 1)
- Axis 2: Etiology (Figure 2)
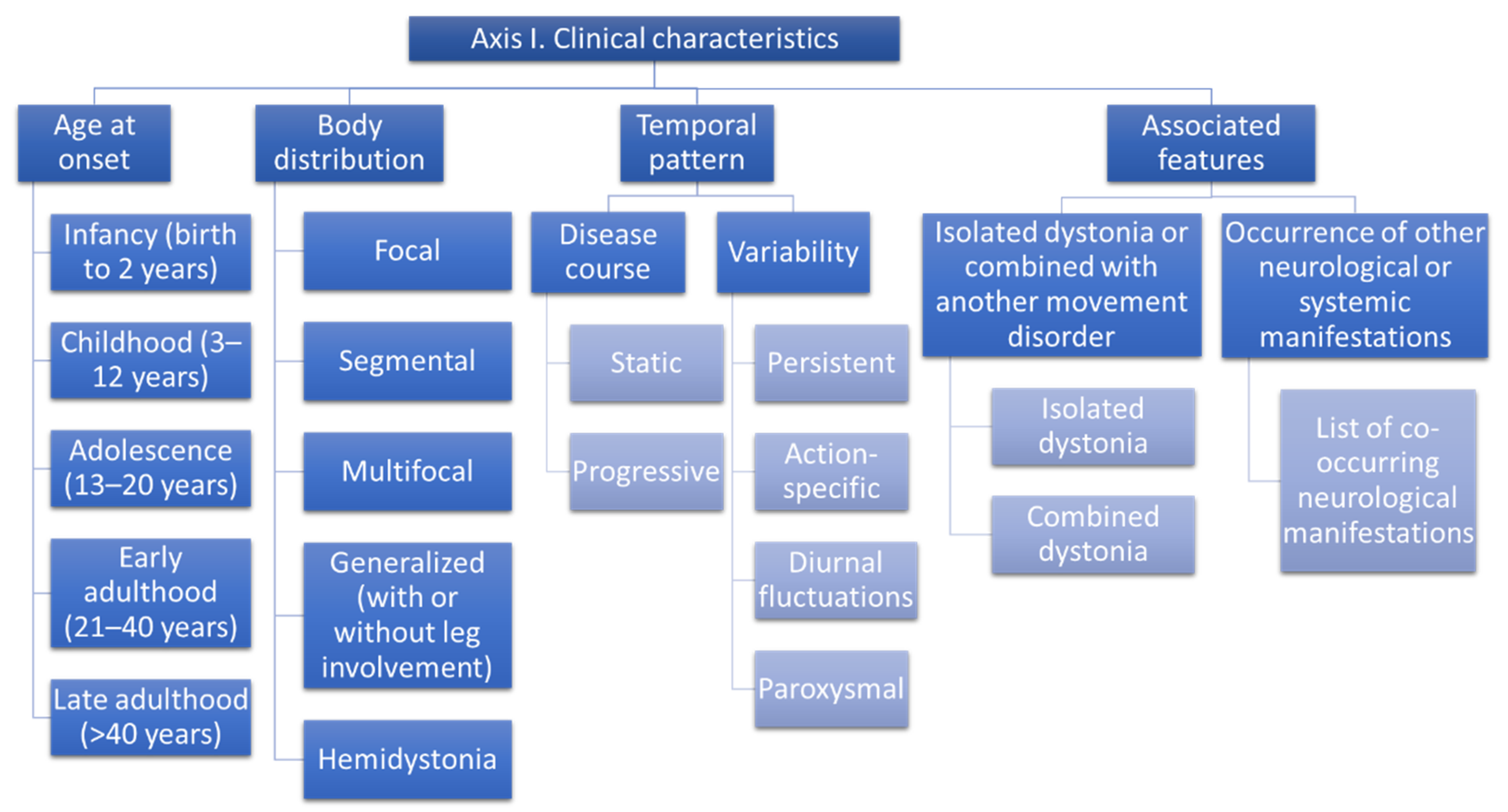
Figure 1. Classification of dystonia. Axis 1 Clinical characteristics.
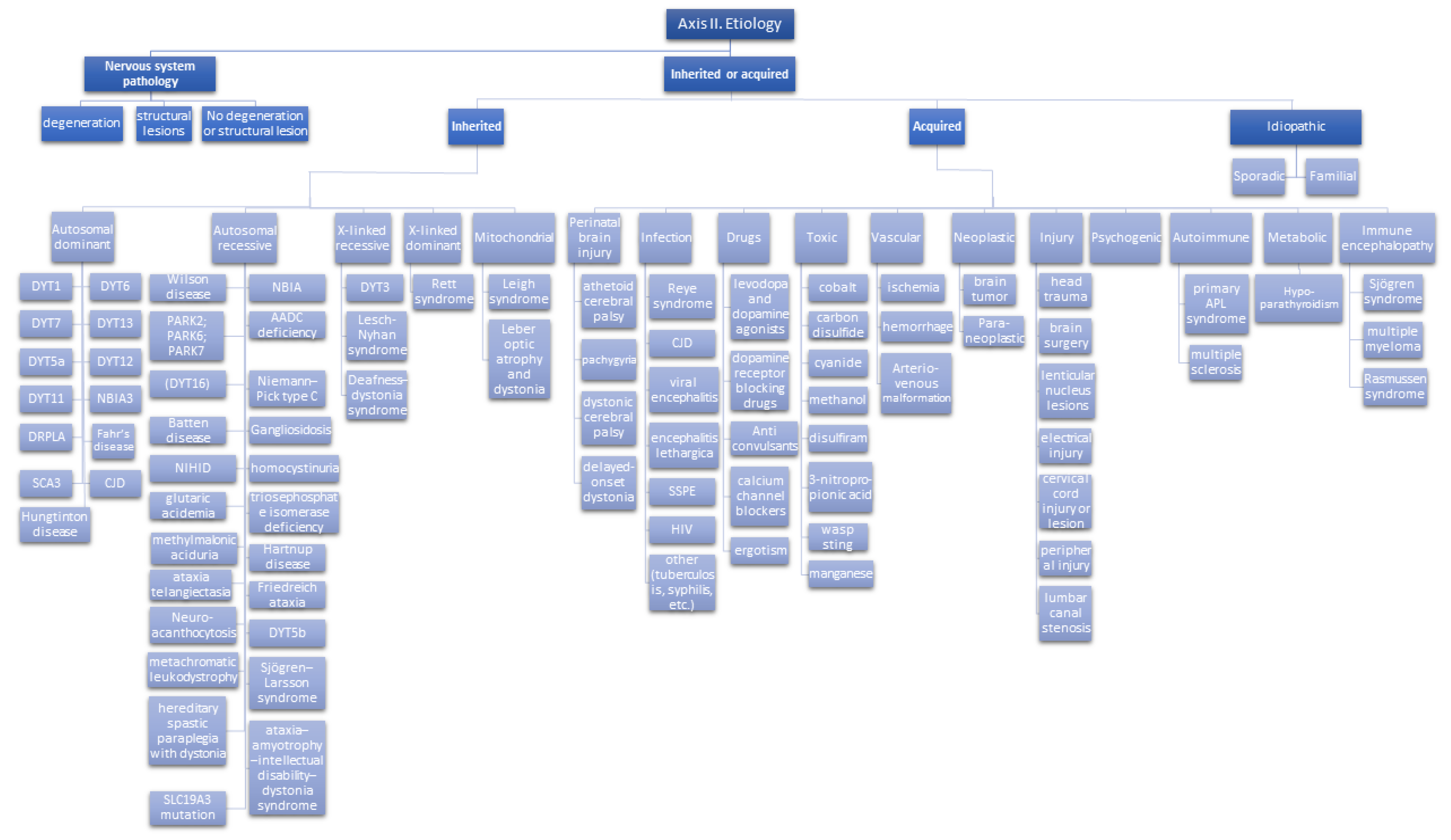
Figure 2. Classification of dystonia. Axis 2 Etiology.
The two axes are needed since each pattern of clinical characteristics could lead to different etiologies, and therefore there isn’t a unique link between the clinical spectrum and the etiology.
In addition, for a single patient, the classification on the 2 axes can be updated over time in a nonparallel way, since the clinical spectrum can evolve during the disease course, but the etiology remains unchanged unless new evidence updates this axis [1].
Axis 1 allows a snapshot of the clinical features of the patient to be taken and to recognize the syndromic pattern. Axis 1 characterization will orient the selection of diagnostic tests to define the etiology (i.e., genetic testing, imaging, lab, or instrumental tests) [1].
This entry is adapted from the peer-reviewed paper 10.3390/life12020206
References
- Albanese, A.; Bhatia, K.; Bressman, S.B.; DeLong, M.R.; Fahn, S.; Fung, V.S.; Hallett, M.; Jankovic, J.; Jinnah, H.A.; Klein, C. Phenomenology and classification of dystonia: A consensus update. Mov. Disord. 2013, 28, 863–873.
- Elia, A.; Lalli, S.; Albanese, A. Differential diagnosis of dystonia. Eur. J. Neurol. 2010, 17, 1–8.
- Fahn, S.; Eldridge, R. Definition of dystonia and classification of the dystonic states. Adv. Neurol. 1976, 14, 1–5.
- Fahn, S.; Marsden, C.D.; Calne, D.B. Classification and investigation of dystonia. Mov. Disord. 1987, 2, 332–358.
- Fahn, S.; Bressman, S.B.; Marsden, C.D. Classification of dystonia. Adv. Neurol. 1998, 78, 1–10.
- Albanese, A.; Asmus, F.; Bhatia, K.P.; Elia, A.E.; Elibol, B.; Filippini, G.; Gasser, T.; Krauss, J.K.; Nardocci, N.; Newton, A.; et al. EFNS guidelines on diagnosis and treatment of primary dystonias. Eur. J. Neurol. 2011, 18, 5–18.
- Fahn, S.; Jankovic, J.; Hallett, M. Principles and Practice of Movement Disorders; Elsevier Health Sciences: Oxford, UK, 2011.
This entry is offline, you can click here to edit this entry!